Metastatic castration-sensitive prostate cancer (mCSPC) is incurable, and the aim of treatment is tumor suppression to prolong survival.1
For patients with mCSPC, androgen deprivation therapy alone (ADT) continues to be used widely despite the availability of newer and more effective therapies. Androgen receptor pathway inhibitors, also known as ARPIs, in combination with ADT, have become available over the last decade. Clinical trials of ARPIs show that these treatments are more efficacious as life-prolonging therapies for patients with mCSPC than ADT alone.2-6
Apalutamide is a specific type of ARPI that was evaluated in the TITAN trial. When given to patients with mCSPC, the combination of APA+ADT reduced the risk of radiographic progression-free survival by 52% (p<0.001), reduced the risk of castration resistance by 66% (p<0.0001), and reduced the risk of death by 35% (p <0.0001) compared to placebo+ADT.8
The OASIS Project
The goal of the OASIS project was to see if these clinical trial findings translated into clinical practice. We evaluated the impact of apalutamide + ADT as a starting treatment for patients with mCSPC in real-world clinical practice in the US. This was a retrospective, observational study, using data from electronic records from 4937 patients in the ConcertAI RWD 360 prostate cancer dataset.
The study compared short term and long-term clinical outcomes in patients with newly diagnosed mCSPC who initiated treatment with either apalutamide + ADT, enzalutamide + ADT, abiraterone acetate plus prednisone + ADT, or ADT alone. Short terms outcomes were the time taken for the PSA levels to drop to 50% of baseline (PSA50), to 90% of baseline (PSA90), or to undetectable levels. Long term outcomes were the development of castration resistance and overall survival.
Key Findings
Our study confirmed that patients with newly diagnosed mCSPC experienced clinical benefits including significantly longer survival and longer time to castration resistance when treatment was initiated with ARPIs + ADT compared to ADT alone.
Additionally, we showed that the use of apalutamide +ADT as a starting treatment had the greatest positive impact on all short-term and long-term outcomes studied. Upfront apalutamide + ADT in mCSPC was associated with the fastest time to PSA50, PSA90%, and undetectable PSA from baseline, the longest time to castration resistance, and the highest reduction in the risk of death compared with the other ARPIs evaluated in this study (Fig. 1).
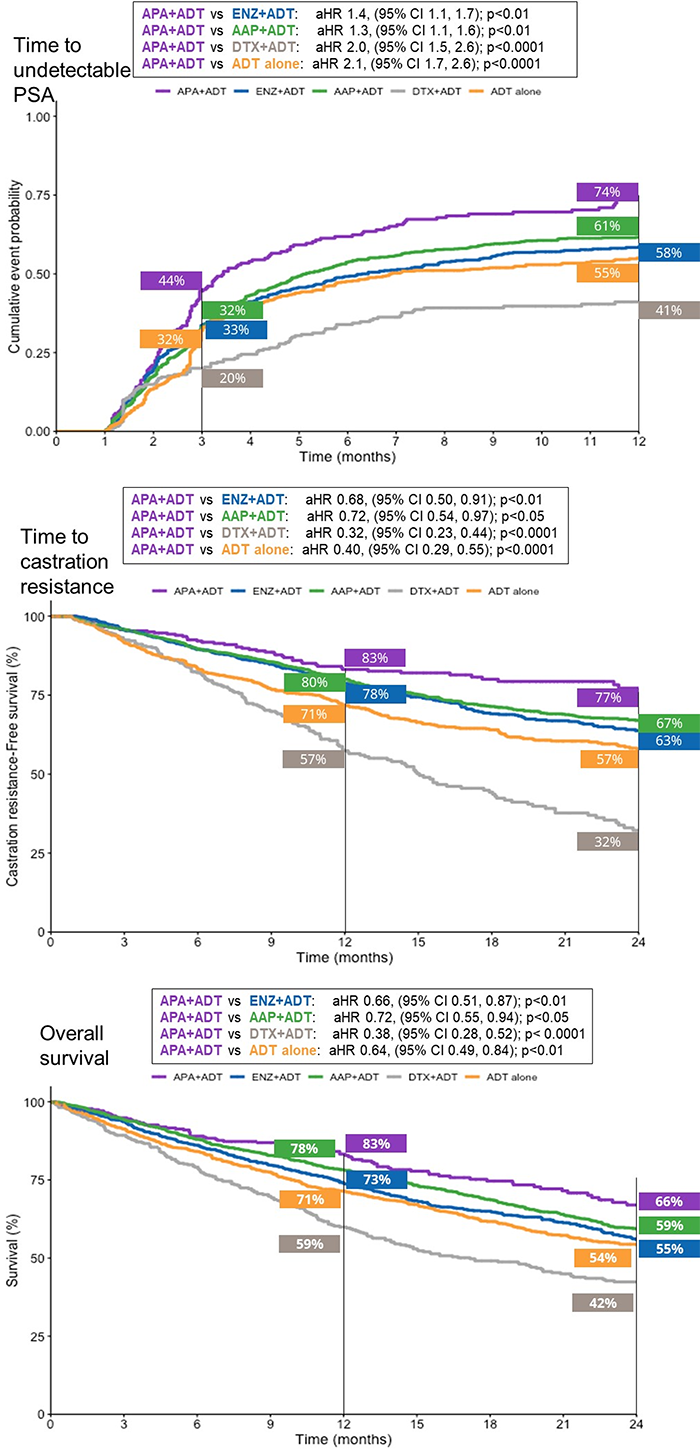
Figure caption: Kaplan-Meier curves showing the percentage of patients who reached undetectable PSA, who remained castration-sensitive, and who survived during the follow-up period. AAP, abiraterone acetate plus prednisone; ADT, androgen deprivation therapy; APA, apalutamide; ENZ, enzalutamide; Undetectable PSA, ≤0.2 ng/ml
Implications for Cancer Treatment
We showed that the use of apalutamide + ADT as starting treatment for these patients demonstrated significantly better clinical outcomes when compared with other ARPIs +ADT, or ADT alone. These real-world data strongly suggest that apalutamide may differ from other ARPIs in its ability to induce rapid, deep, and durable PSA responses that prolong survival in patients with mCSPC.
Of concern, we also found that many patients with metastatic prostate cancer were not receiving intensified therapies such as ARPIs, even though ADT alone is no longer recommended as starting therapy in patients with mCSPC and adequate life expectancy.7,8
Future Directions
Evaluation of new drug combinations that are becoming available will need to be considered in future studies. In addition, further research to understand patient and physician determinants of treatment selection could help to optimize treatment choice and outcomes for patients with mCSPC.
Written by:
- Benjamin L. Maughan, MD, PharmD, Huntsman Cancer Institute, University of Utah, Salt Lake City, UT
- Lawrence I. Karsh, MD, Advent Health Urology Denver, Denver, CO
- Hussain M, Fizazi K, Shore ND, Heidegger I, Smith MR, Tombal B et al. Metastatic hormone-sensitive prostate cancer and combination treatment outcomes: a review. JAMA Oncol 2024; 10(6): 807-820.
- Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev B, Y et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med 2017; 377(4): 352-360.
- Davis ID, Martin AJ, Stockler MR, Begbie S, Chi KN, Chowdhury, S et al. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med 2019; 381(2): 121-131.
- Chi KN, Agarwal N, Bjartell A, Chung BH, Pereira de Santana Gomes AJ, Given R et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med 2019; 381(1): 13-24.
- Chi KN, Chowdhury S, Bjartell A, Chung BH, Pereira de Santana Gomes AJ, Given R, et al. Apalutamide in patients with metastatic castration-sensitive prostate cancer: Final survival analysis of the randomized, double-blind, phase III TITAN study. J Clin Oncol 2021; 39(20): 2294-2303.
- Armstrong AJ, Szmulewitz RZ, Petrylak DP, Holzbeierlein J, Villers A, Azad A et al. ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy With Enzalutamide or Placebo in Men With Metastatic Hormone-Sensitive Prostate Cancer. J Clin Oncol 2019; 37(32): 2974-2986.
- Lowrance W, Dreicer R, Jarrard DF, Scarpato KR, Kim SK, Kirkby, E et al. Updates to advanced prostate cancer: AUA/SUO Guideline (2023). J Urol 2023; 209(6): 1082-1090.
- Cornford P, Bellmunt J, Bolla M, Briers E, De Santis M, Gross T et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part II: treatment of relapsing, metastatic, and castration-resistant prostate cancer. Eur Urol 2017; 71(4): 630-642.