Our retrospective, multicenter analysis focused on real-world outcomes of ICIs, such as pembrolizumab, in patients with advanced or metastatic PSCC. Despite the small sample size, our findings contribute valuable evidence supporting the use of immunotherapy in select patients and provide a foundation for future research.
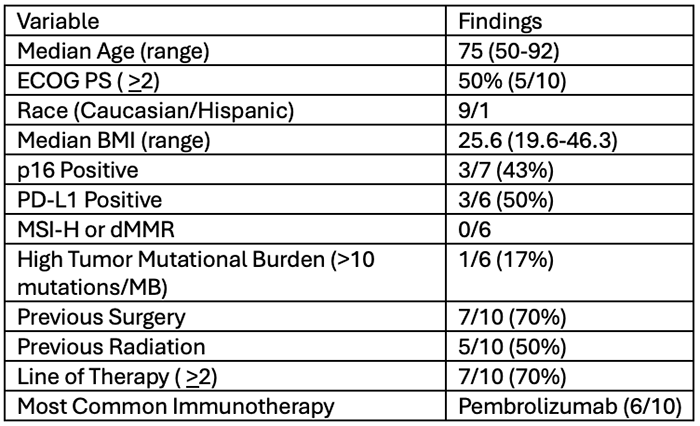
Table 1: Patients’ Characteristics
Key Findings and Clinical Implications
- Meaningful Responses in Select Patients: We observed an overall response rate (ORR) of 30%, including one complete response (CR). While this is lower than response rates seen in some other cancers treated with ICIs, the disease control rate (DCR) was 40%, suggesting that some patients experience prolonged benefit.
- Durability of Responses and Disease Control: In patients with response or disease control, the duration exceeded 12 months and 8 months, respectively—an impressive finding given the historically poor prognosis of metastatic PSCC.
- Response or disease control was observed in two cisplatin-ineligible patients in the first-line setting, and in two additional patients who achieved response or disease control after progression on cisplatin-based therapy in the second line.
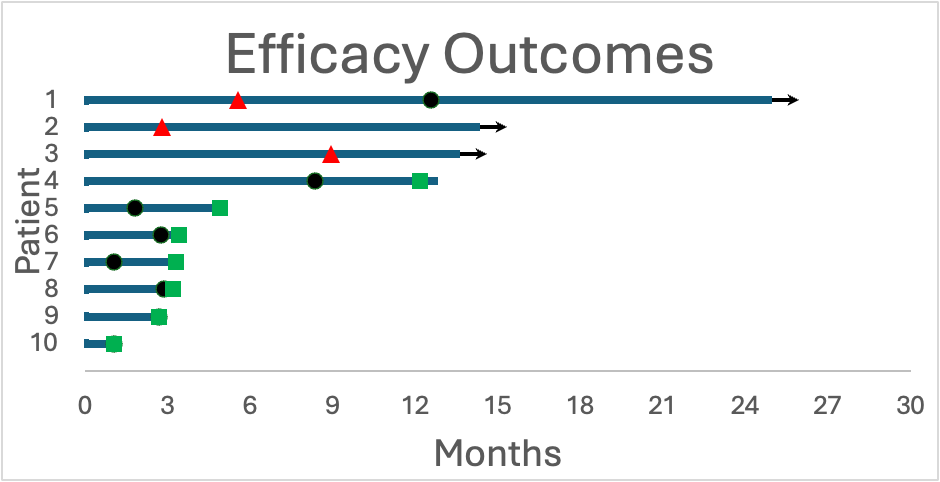
Figure 1: Treatment Responses and Duration of Treatment
- PD-L1 and HPV Status May Predict Response: Among patients with available biomarker data, those with PD-L1 or HPV-positive tumors had a 67% response rate, suggesting that these factors may be predictive biomarkers for immunotherapy benefit.
- Well-Tolerated Treatment: No patients developed serious (grade 3 or 4) immune-related adverse events (irAEs), and there were no treatment discontinuations due to toxicity. This is particularly important in a frail patient population who often struggle with the side effects of chemotherapy.
Traditional chemotherapy options, such as cisplatin plus fluorouracil (5-FU) or paclitaxel, ifosfamide, and cisplatin (TIP), offer response rates of 25-50% but come with significant toxicity.1-3 In contrast, ICIs offer a more tolerable option, particularly for cisplatin-ineligible patients.
The HERCULES trial, a recent phase 2 study, evaluated pembrolizumab plus platinum chemotherapy as first-line therapy for PSCC, reporting a 39.4% ORR and a median overall survival (OS) of 9.6 months.4 Our study complements these findings by providing real-world data on ICI monotherapy, showing that some patients can achieve durable responses even without chemotherapy.
Furthermore, prior reports on single-agent cetuximab and paclitaxel in the second-line setting show ORRs of ~20%, with responses lasting only a few months.5,6 Our data suggest that ICIs may provide a more durable option, particularly for biomarker-selected patients.
What’s Next for Immunotherapy in PSCC?
- Biomarker-Driven Approaches: Our findings reinforce the need for better patient selection using PD-L1 expression, HPV status, and tumor mutational burden (TMB) to optimize ICI use.
- Combination Strategies: Given that some patients do not respond to single-agent ICIs, combining them with chemotherapy, targeted therapy (e.g., anti-EGFR agents), or novel immune-modulating drugs may enhance response rates.
- Larger Prospective Studies: While our study is an important step forward, larger trials are needed to define the optimal role of immunotherapy in PSCC.
This study provides real-world evidence that immune checkpoint inhibitors offer a promising, well-tolerated treatment option in metastatic PSCC, particularly for patients who are PD-L1 or HPV-positive. While response rates remain modest, the durability of benefit in some patients underscores the potential role of ICIs in this rare and challenging disease. Further prospective studies are needed to refine patient selection strategies and optimize treatment combinations.
Written by: Haoran Li, MD, PhD, and Timothy Schieber, PharmD, The University of Kansas Cancer Center, Westwood, KS
References:
- Di Lorenzo G, Buonerba C, Federico P, et al. Cisplatin and 5-fluorouracil in inoperable, stage IV squamous cell carcinoma of the penis. BJU Int. 2012;110(11 Pt B):E661-E666.
- Pagliaro LC, Williams DL, Daliani D, et al. Neoadjuvant paclitaxel, ifosfamide, and cisplatin chemotherapy for metastatic penile cancer: a phase II study. J Clin Oncol. 2010;28:3851-3857.
- Shammas FV, Ous S, Fossa SD. Cisplatin and 5-fluorouracil in advanced cancer of the penis. J Urol. 1992;147:630-632.
- Maluf FC, Trindade K, Almeida Preto DD, et al. A phase II trial of pembrolizumab plus platinum-based chemotherapy as first-line systemic therapy in advanced penile cancer: HERCULES (LACOG 0218) trial. Presented at: 2024 American Society of Clinical Oncology Annual Meeting. May 31-June 4, 2024. Chicago, Illinois. Abstract 5009.
- Carthon BC, Ng CS, Pettaway CA, Pagliaro LC. Epidermal growth factor receptor-targeted therapy in locally advanced or metastatic squamous cell carcinoma of the penis. BJU Int. 2014;113:871-877.
- Di Lorenzo G, Federico P, Buonerba C, et al. Paclitaxel in pretreated metastatic penile cancer: final results of a phase 2 study. Eur Urol. 2011;60:1280-1284.