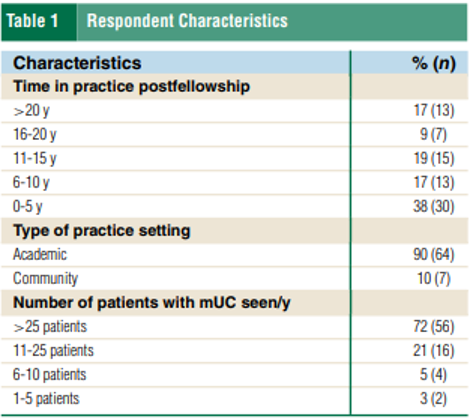
The study surveyed 227 U.S. genitourinary medical oncologists between May and August 2024, achieving a 34% response rate (78 respondents). Respondent characteristics (Table 1) included 62% with more than 5 years of practice and 72% managing more than 25 patients with metastatic urothelial carcinoma (mUC) annually.
The central finding—that 51% of respondents were somewhat or very likely to use enfortumab vedotin plus pembrolizumab (EVP) after progression on adjuvant ICI—reflects the gravitational pull of the EV-302 data.2,3 That landmark trial demonstrated a median overall survival of 31.5 months with EVP versus 16.1 months with platinum-based chemotherapy (HR 0.47; 95% CI, 0.38–0.58; P 0.001), with updated 2.5-year follow-up confirming a durable benefit (median OS 33.8 months; HR 0.51).2 These results have established EVP as the NCCN-preferred first-line regimen for locally advanced or metastatic disease (category 1).4 Yet the critical caveat is that EV-302 excluded patients with prior ICI exposure, leaving the efficacy of EVP in ICI-pretreated patients fundamentally unproven.
The survey's exploration of the ICI-free interval is also instructive (Table 2). For patients progressing on adjuvant ICI, 1/3 of respondents would consider first-line EVP irrespective of the interval from prior ICI completion, while 43–45% would consider EVP only if more than 6 months had elapsed since ICI completion (for NMIBC and MIBC settings, respectively). This time-dependent threshold mirrors clinical reasoning applied in other oncologic contexts—such as platinum re-challenge after a prolonged treatment-free interval—but lacks prospective validation in the ICI-to-EVP sequence. Whether the pembrolizumab component of EVP retains meaningful activity after recent ICI exposure, or whether EV alone drives the benefit in this population, remains an open question.

Several methodological considerations warrant discussion. First, survey-based research inherently captures stated preferences rather than actual practice patterns, and the gap between the two can be substantial. Real-world data from electronic health records or registry studies would complement these findings. Second, the survey was conducted before the full integration of several practice-changing developments, including the FDA approval of durvalumab for perioperative MIBC based on the NIAGARA trial (approved March 2025), which demonstrated improved event-free survival (HR 0.68) and overall survival (HR 0.75) with perioperative durvalumab plus neoadjuvant gemcitabine-cisplatin.5 As perioperative ICI-containing regimens become standard, the population of patients developing mUC after prior ICI exposure will expand considerably, making the questions posed by this survey even more urgent.
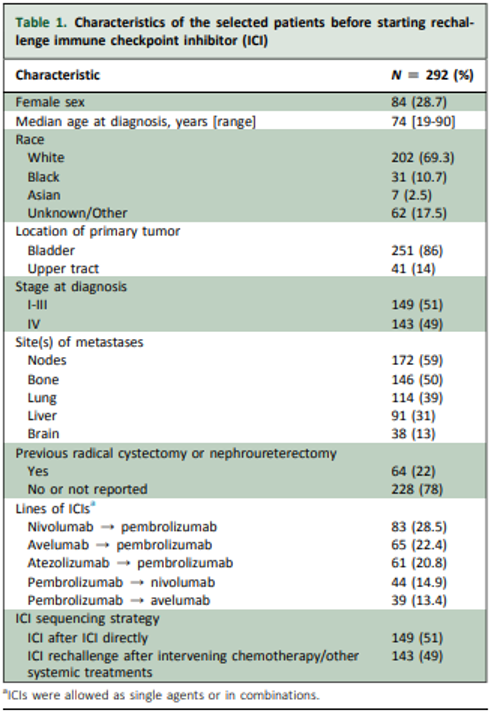
Since this survey was conducted, the largest real-world analysis on ICI rechallenge in mUC was published by Maiorano et al.6 The cohort comprised predominantly bladder cancer (86%) versus upper tract UC (14%). Notably, 51% had stage I–III disease at initial diagnosis, while 49% had stage IV, reflecting the increasing use of ICIs in earlier disease settings (Table 1). The median time on prior ICI was 19.5 months, and the median interval from the end of prior ICI to rechallenge was 9.4 months.
After a median follow-up of 21.7 months, ICI rechallenge yielded a median OS of 20.5 months and a median PFS of 10.3 months.6 These outcomes compare favorably with historical benchmarks for ICI monotherapy in the metastatic setting. The results also align with the pooled post hoc analysis of pembrolizumab retreatment across KEYNOTE-045, KEYNOTE-052, and KEYNOTE-361, which reported a median PFS of 9.5 months and a median OS of 25.7 months in 49 patients who had previously responded to first-course pembrolizumab.7 However, the KEYNOTE pooled analysis was restricted to patients who had achieved at least stable disease on initial ICI, representing a more favorable prognostic population.
Two key predictors of improved outcomes with ICI rechallenge emerged from the Maiorano et al. analysis. First, patients whose initial ICI was administered in a nonmetastatic setting (e.g., adjuvant or perioperative) had significantly longer median OS upon rechallenge compared to those who received both ICI courses in the advanced setting (P 0.001).6 This finding is clinically relevant given the expanding use of perioperative immunotherapy with nivolumab, pembrolizumab, and durvalumab in muscle-invasive bladder cancer. Second, among patients who received prior ICI in the metastatic setting, a treatment-free interval of ≥12 months before rechallenge was associated with significantly longer median OS (P = 0.027).6 This is consistent with broader ICI rechallenge literature across solid tumors, where a treatment-free interval ≥6 months has been identified as a predictor of successful rechallenge.8
While the Maiorano et al. study provides the largest cohort to date, several limitations warrant consideration. The TriNetX® database relies on ICD and procedure codes, which may introduce misclassification. The study lacked granular data on reasons for ICI discontinuation (progression vs. toxicity vs. completion of planned therapy), which is a critical determinant of rechallenge outcomes, as patients who discontinue due to immune-related adverse events tend to have better outcomes upon rechallenge than those who progress.9 Prospective studies with standardized predictive biomarkers and treatment protocols are needed to refine patient selection for ICI rechallenge in advanced urothelial carcinoma. The ECOG-ACRIN EA8231 trial is one of these trials, currently enrolling and evaluating the role of SG +/- pembrolizumab in the 2L mUC post-EVP setting.
The broader implications of this work extend beyond urothelial carcinoma. Across oncology, the success of immunotherapy in earlier disease states is creating a growing population of patients who relapse after prior ICI exposure. Understanding optimal treatment sequencing in this context represents one of the most pressing questions in contemporary oncology practice.
Written by: Karine Tawagi, MD, Assistant Professor of Medicine, Department of Medicine, Division of Hematology and Oncology, University of Illinois Cancer Center, Chicago, IL
References:
- Tawagi K, Khaki AR, Chablani PV, Hoffman-Censits J, Koshkin VS, Plimack ER, Galsky MD, Gupta S, Rosenberg JE, Grivas P, O'Donnell PH. Preferred Treatment Sequencing for Metastatic Urothelial Carcinoma (mUC) in the Era of Perioperative and First-Line (1L) Checkpoint Inhibitor: Results From a National Survey of Genitourinary Oncologists. Clin Genitourin Cancer. 2026 Mar;24(2):102487. doi: 10.1016/j.clgc.2025.102487. Epub 2025 Dec 20. PMID: 41582039.
- Powles TB, Van der Heijden MS, Loriot Y, et al. Enfortumab Vedotin Plus Pembrolizumab in Untreated Locally Advanced or Metastatic Urothelial Carcinoma: 2.5-Year Median Follow-Up of the Phase III EV-302/KEYNOTE-A39 Trial. Ann Oncol. 2025 Oct;36(10):1212-1219. doi: 10.1016/j.annonc.2025.05.536.
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024 Mar;390(10):875-888. doi: 10.1056/NEJMoa2312117.
- Bladder Cancer. National Comprehensive Cancer Network. Updated 2026-03-16.
- Powles, T., Catto, J. W., Galsky, M. D., Al-Ahmadie, H., Meeks, J. J., Nishiyama, H., ... & Van Der Heijden, M. S. (2024). Perioperative durvalumab with neoadjuvant chemotherapy in operable bladder cancer. New England Journal of Medicine, 391(19), 1773-1786.
- Maiorano BA, Cigliola A, Tateo V, et al. Outcomes of Immune Checkpoint Inhibitor Rechallenge in Advanced Urothelial Carcinoma: Results From a Global Real-World Evidence Study. ESMO Open. 2025 Dec;10(12):105862. doi: 10.1016/j.esmoop.2025.105862.
- Koshkin VS, Danchaivijitr P, Bae WK, et al. Pembrolizumab Retreatment in Patients With Advanced or Metastatic Urothelial Carcinoma Who Responded to First-Course Pembrolizumab-Based Therapy. Eur Urol. 2025 Apr;87(4):390-395. doi: 10.1016/j.eururo.2024.11.012.
- Abushukair HM, Al-Kraimeen LM, Saeed A. Predictors of response to immune checkpoint inhibitors (ICI) rechallenge post-disease progression in solid tumors: A systematic review and meta-analyses. J Clin Oncol. 2022 Jun;40(16 Suppl):2612. doi: 10.1200/JCO.2022.40.16_suppl.2612.
- Lu S, Xie Z. Advancing Immune Checkpoint Inhibitor Rechallenge: Key Insights Into Efficacy, Safety, and Personalized Strategies in Advanced Solid Tumors. Front Oncol. 2026;16:1766921. doi: 10.3389/fonc.2026.1766921.