Dr. Joshua Meeks discussed current and future approaches in muscle-invasive bladder cancer, highlighting three key phases in 2025—neoadjuvant, local, and adjuvant—which formed the framework for his talk.

There are several neoadjuvant therapy options:
- Cisplatin-based chemotherapy (dose dense MVCA): reasonable, and may be better for variant histologies and for those patients with higher performance status
- Gemcitabine + cisplatin + durvalumab (the NIAGARA regimen):1 easy to deliver and improves survival
- Likely, enfortumab vedotin + pembrolizumab after ESMO 2025: awaiting FDA approval post-ESMO
Dr. Meeks then discussed the VESPER trial, which attempted to answer the question of what type of chemotherapy to use in the neoadjuvant setting.2 Patients with pT2 disease were randomized to 4 cycles of gemcitabine + cisplatin versus 6 cycles of dose-dense MVAC, with 89% of patients receiving treatment in the neoadjuvant setting. Notably, dose dense MVAC in a subgroup analysis was favored for neoadjuvant chemotherapy and the endpoint of overall survival:

The pathological complete response rate for dose-dense MVAC was 42% and for gemcitabine + cisplatin was 36%. However, the increased efficacy with dose-dense MVAC came at the cost of increased toxicity, specifically febrile neutropenia, fatigue, and gastrointestinal symptoms.
NIAGARA was the first global phase 3 study to evaluate a perioperative immunotherapy, durvalumab, combined with neoadjuvant chemotherapy in cisplatin-eligible patients with muscle-invasive bladder cancer:1

The first-line results were initially presented at ESMO 2024, noting that event-free survival, as assessed by blinded independent central review in the intention-to-treat population, showed an event-free survival at 2 years of 67.8% in the durvalumab arm compared to 59.8% in the comparator arm. The hazard ratio for event-free survival was 0.68 (95% CI 0.56–0.82, p < 0.0001):
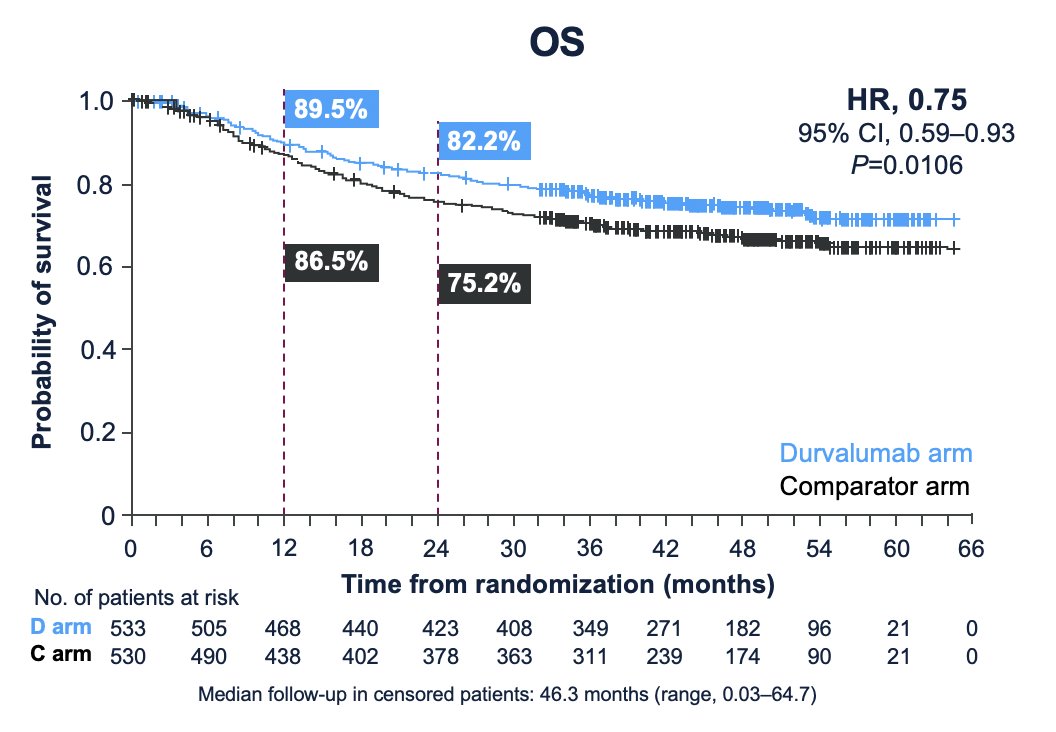
The median follow-up for the overall survival analysis in censored patients was 46.3 months (range 0.03–64.7). At 24 months, 82.2% of patients in the durvalumab arm were alive, compared to 75.2% in the comparator arm. The hazard ratio for overall survival was 0.75 (95% CI 0.59–0.93, p = 0.016):
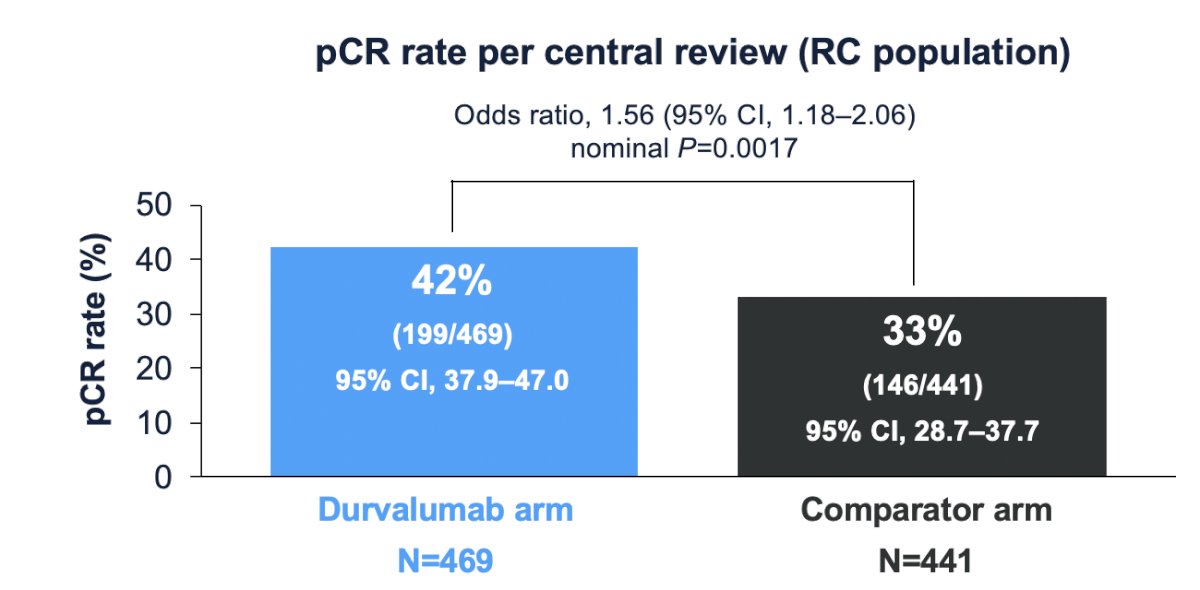
Pathological complete response per central review (in the radical cystectomy population) was 42% (95% CI 37.9%-47.0%) in the durvalumab arm versus 33% (95% 28.7%-37.7%) in the comparator arm (OR 1.56, 95% CI 1.18-2.06):
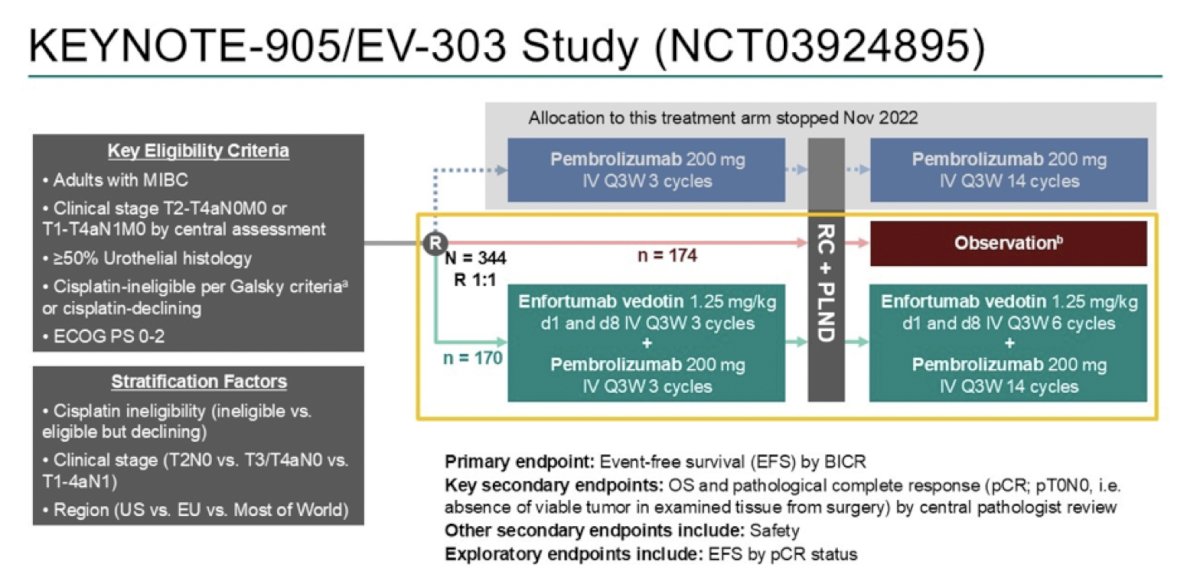
The KEYNOTE-905/EV-303 trial was first presented at ESMO 2025 by Dr. Christof Vulsteke. KEYNOTE-905/EV-303 enrolled adults with muscle invasive bladder cancer (≥50% urothelial histology) who were either cisplatin ineligible per Galsky criteria or declined cisplatin, had an ECOG performance status of 0-2, and clinical stage T2-T4aN0M0 or T1-T4aN1M0 disease. Patients were randomized across three study arms: two experimental perioperative arms, one with pembrolizumab alone and one with enfortumab vedotin + pembrolizumab, and a control arm of radical cystectomy + pelvic lymph node dissection followed by observation. Treatment in the experimental arms included three neoadjuvant cycles of pembrolizumab (with or without enfortumab vedotin), followed by radical cystectomy + pelvic lymph node dissection, and continued with 14 adjuvant cycles of pembrolizumab (plus six cycles of enfortumab vedotin in the enfortumab vedotin combination arm):
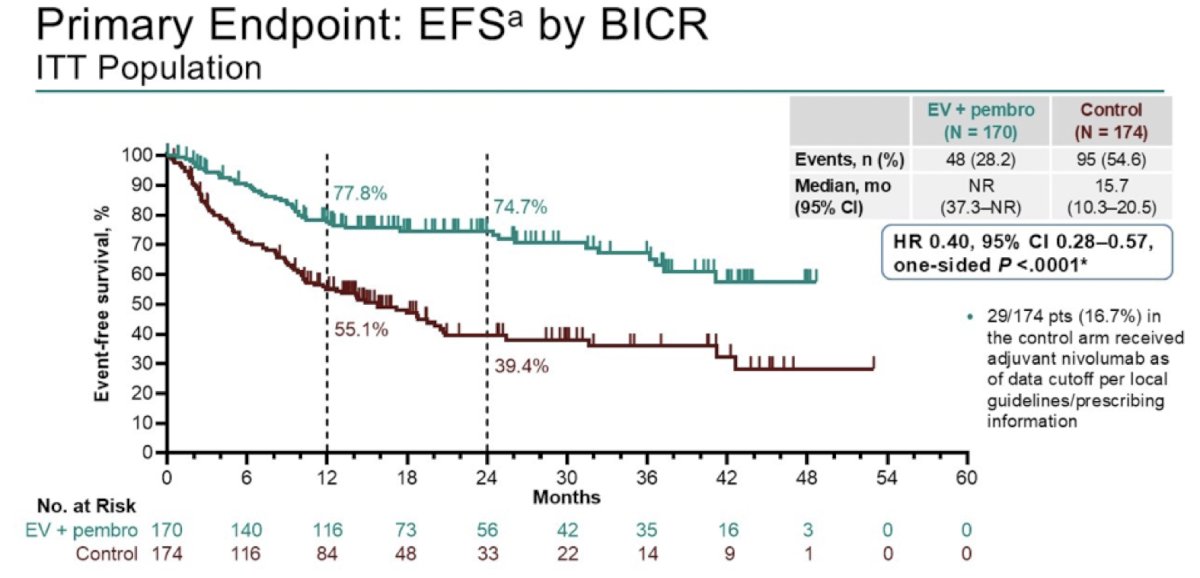
The primary endpoint of event-free survival by blinded independent central review demonstrated a significant improvement with enfortumab vedotin + pembrolizumab versus control, with median event-free survival not reached compared to 15.7 months (HR 0.40, 95% CI 0.28–0.57; one-sided p < 0.0001):
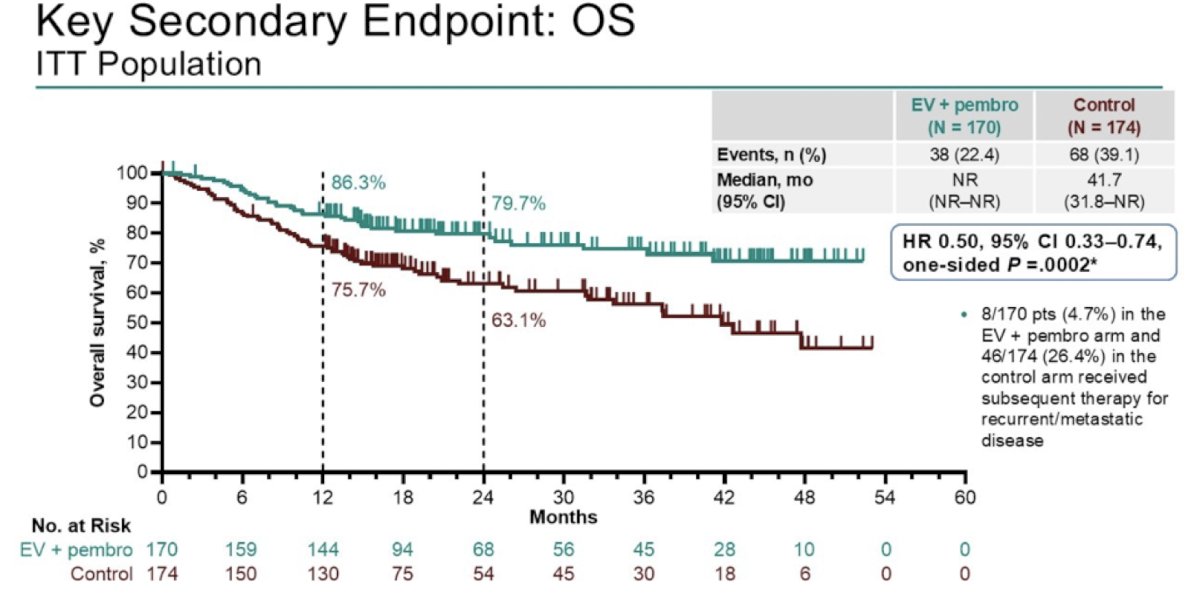
The key secondary endpoint of overall survival showed a median of 41.7 months in the control arm versus not reached with enfortumab vedotin + pembrolizumab (HR 0.50, 95% CI 0.33–0.74; one-sided p = 0.0002), with early and sustained separation of the curves. This represents the first trial to demonstrate an overall survival benefit in cisplatin-ineligible muscle-invasive bladder cancer patients:
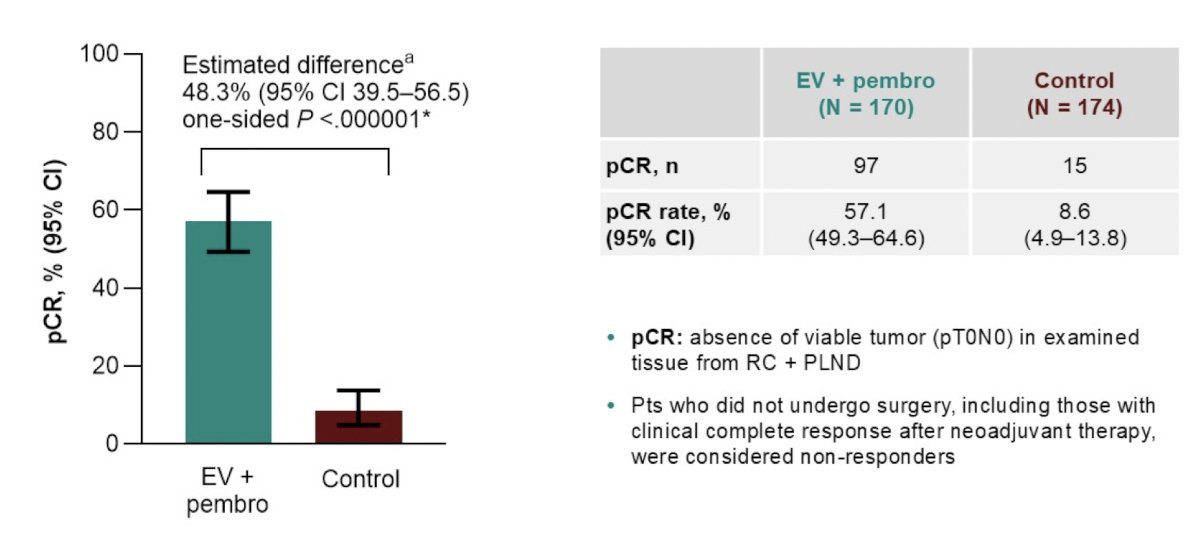
Pathological complete response, defined as the absence of viable tumor (pT0N0) in radical cystectomy specimens, was a key secondary endpoint of the study. The pathological complete response rate was 57.1% with enfortumab vedotin + pembrolizumab versus 8.6% with control (estimated difference 48.3%, one-sided p < 0.000001). This represents the highest pathological complete response rate ever reported in a phase 3 muscle-invasive bladder cancer trial:
Local therapy options for muscle-invasive bladder cancer patients include radical cystectomy or trimodal therapy. Dr. Meeks noted that the RAZOR trial3 was a 15-center multi-center non-inferiority trial of 350 patients undergoing open versus robotic radical cystectomy with a primary endpoint of 2-year progression-free survival. Overall, this study found no difference in recurrence rates, progression rates, or margin status, in addition to similar rates of complications. Estimated blood loss and transfusion rates were higher for open radical cystectomy, whereas length of stay was shorter and operative time was longer for robotic radical cystectomy.
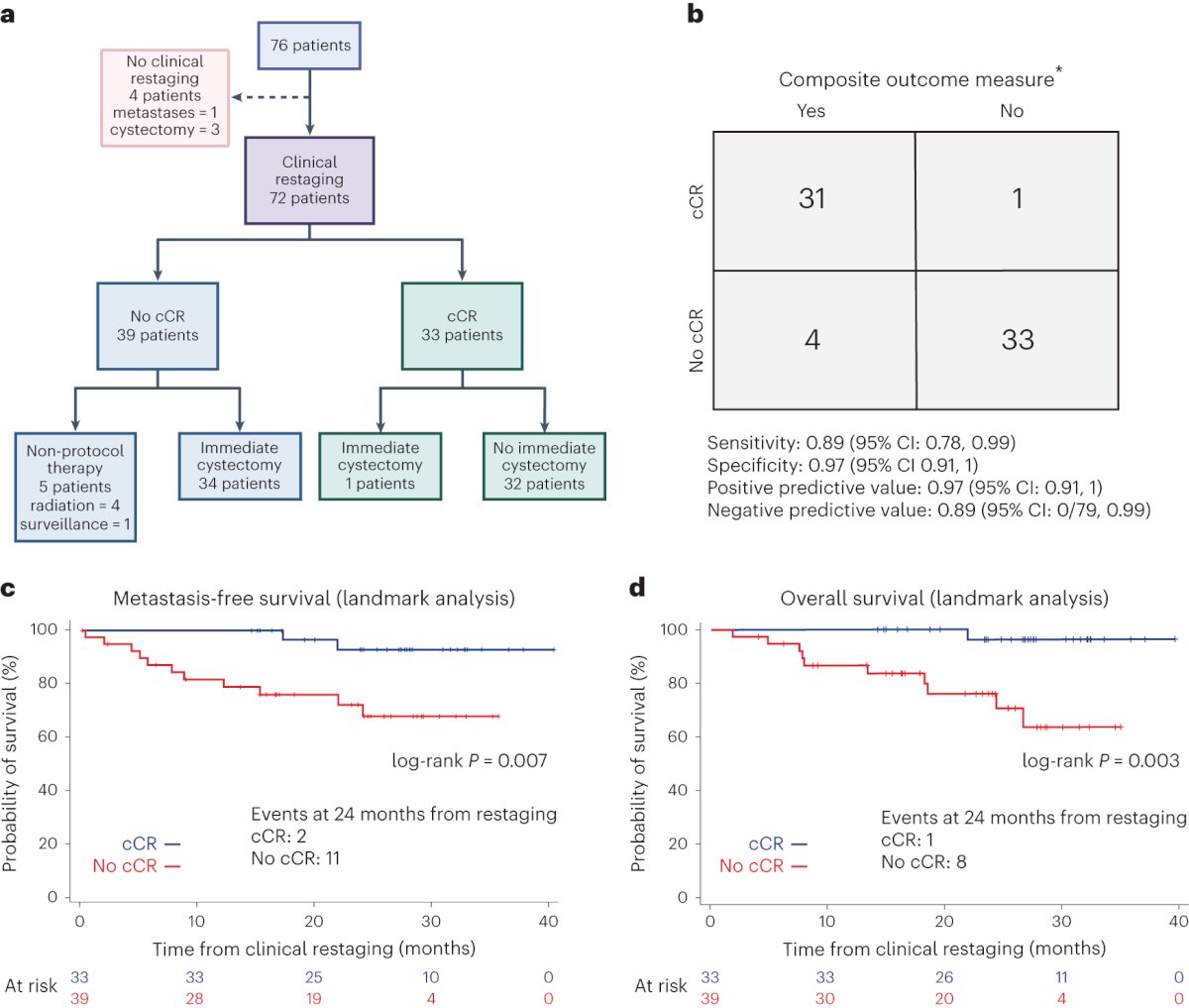
In the HCRN GU16-257 trial, all cT2-4aN0M0 patients received a combination of gemcitabine + cisplatin + nivolumab for 4 cycles. Subsequently, patients were clinically restaged using cystoscopy, biopsies, urine cytology, and MRI. Patients with a clinical complete response were offered either a radical cystectomy or no cystectomy (with a further 8 cycles of nivolumab, akin to adjuvant immune checkpoint inhibitor therapy in patients undergoing cystectomy), per patient choice. Patients without a clinical complete response proceeded to surgery:
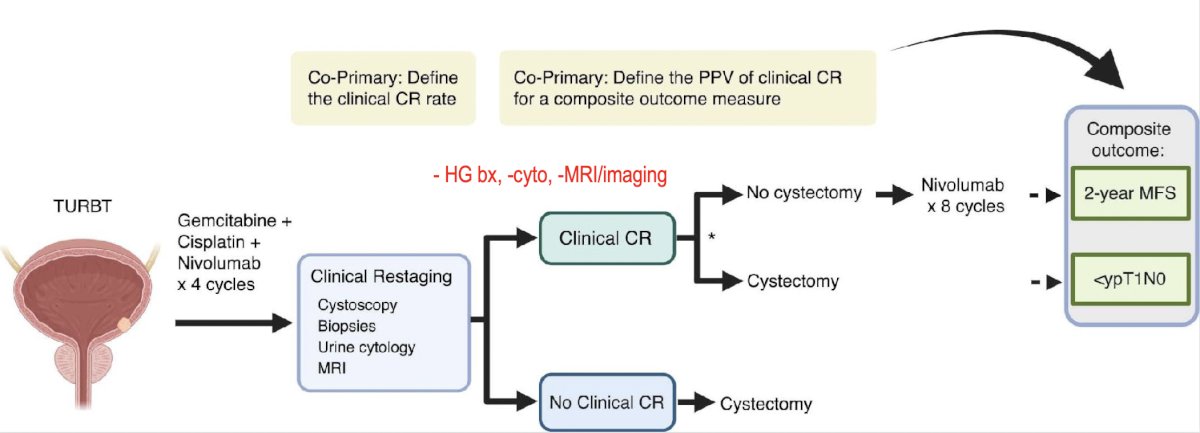
The co-primary endpoints were (i) clinical complete response rate, and (ii) performance of clinical complete response in predicting treatment benefit, defined as either 2-year metastasis-free survival if no cystectomy or pathological complete response in patients undergoing immediate cystectomy. This trial recruited 76 patients, of whom 72 underwent clinical re-staging. Of these 72 re-staged patients, 33 (43%) had a clinical response, and 32/33 chose against proceeding with cystectomy:
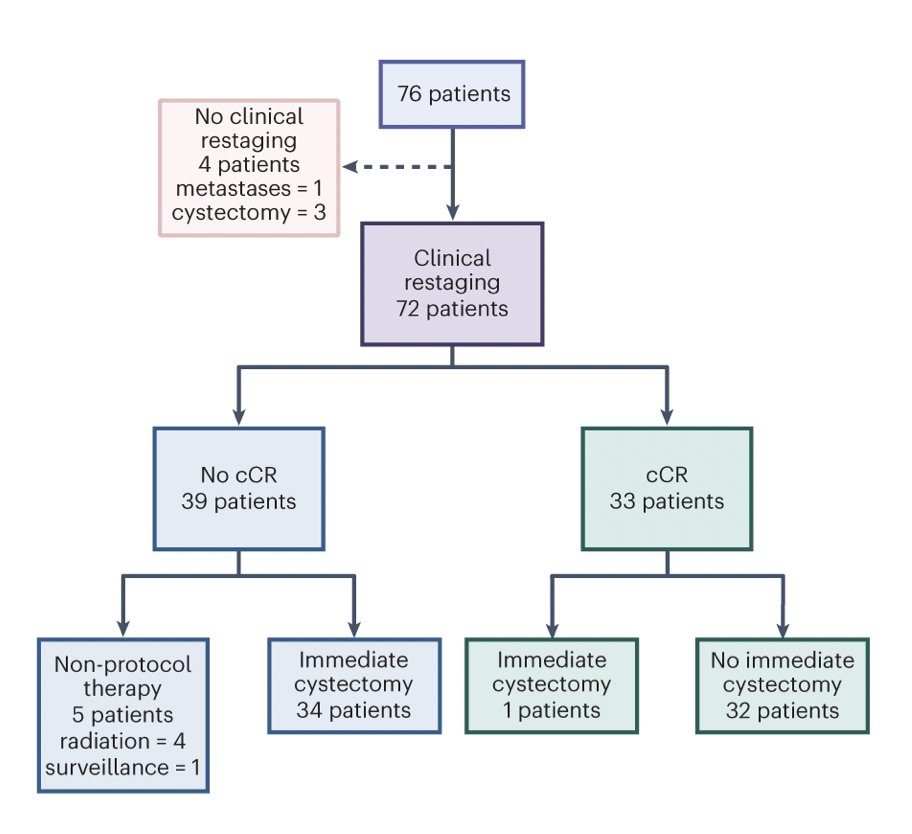
Among patients achieving a clinical complete response (n = 33), 9 patients eventually underwent a delayed radical cystectomy, often after evidence of local recurrence, with 2/33 patients developing metastases. Patients with a clinical complete response had significantly better metastasis-free survival and overall survival, as demonstrated in the Kaplan Meier curves below. Clinical complete response predicted treatment benefit with a positive predictive value of 0.96 (95% CI: 0.89 – 1.0):
Dr. Meeks then discussed adjuvant therapy after radical cystectomy. CheckMate 274 trial4 is a phase 3, randomized, double-blind, multicenter study of adjuvant nivolumab (every 2 weeks) versus placebo. This was a positive trial, with a disease-free survival benefit in both the intention-to-treat analysis (HR 0.70, 98.22% CI 0.55-0.90) and the PD-L1 > 1% analysis (HR 0.55, 98.72% CI 0.35-0.85):
![Dr. Meeks then discussed adjuvant therapy after radical cystectomy. CheckMate 274 trial [4] is a phase 3, randomized, double-blind, multicenter study of adjuvant nivolumab (every 2 weeks) versus placebo. This was a positive trial, with a disease-free survival benefit in both the intention-to-treat analysis (HR 0.70, 98.22% CI 0.55-0.90) and the PD-L1 > 1% analysis (HR 0.55, 98.72% CI 0.35-0.85):](/images/com-doc-importer/240-lugpa-2025/lugpa-2025-mibc---what-you-should-be-doing-today-and-what-we-will-be-doing-tomorrow/image-13.jpg)
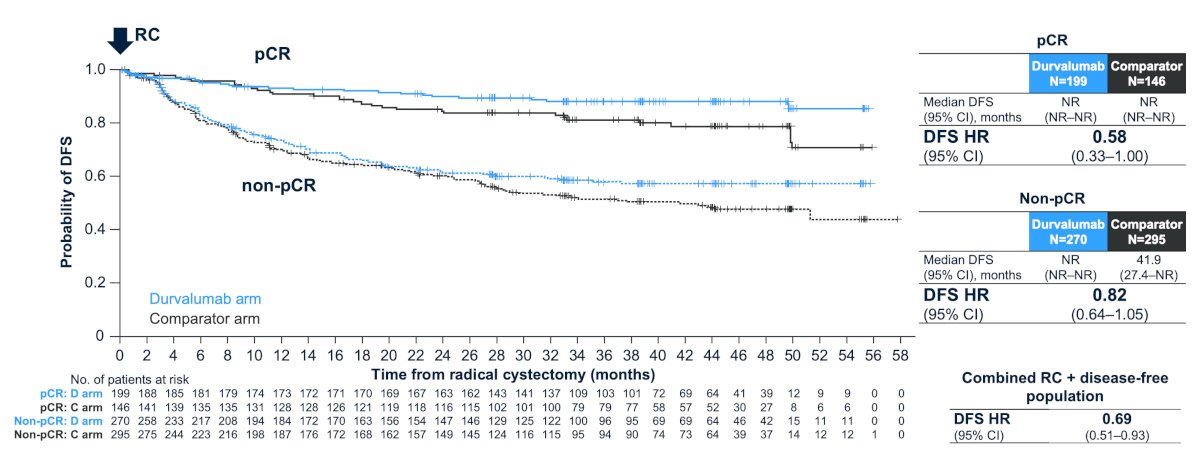
Importantly, in the NIAGARA trial, perioperative durvalumab + neoadjuvant chemotherapy improved disease-free survival in both the pathological complete responders and those without response:
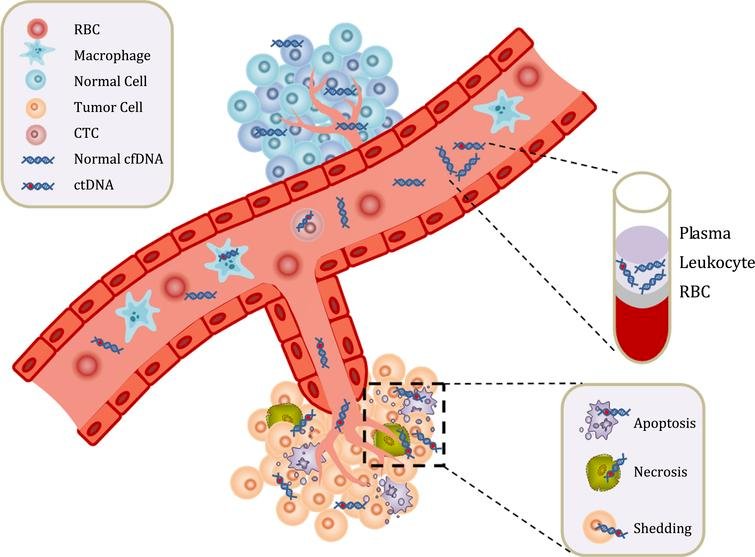
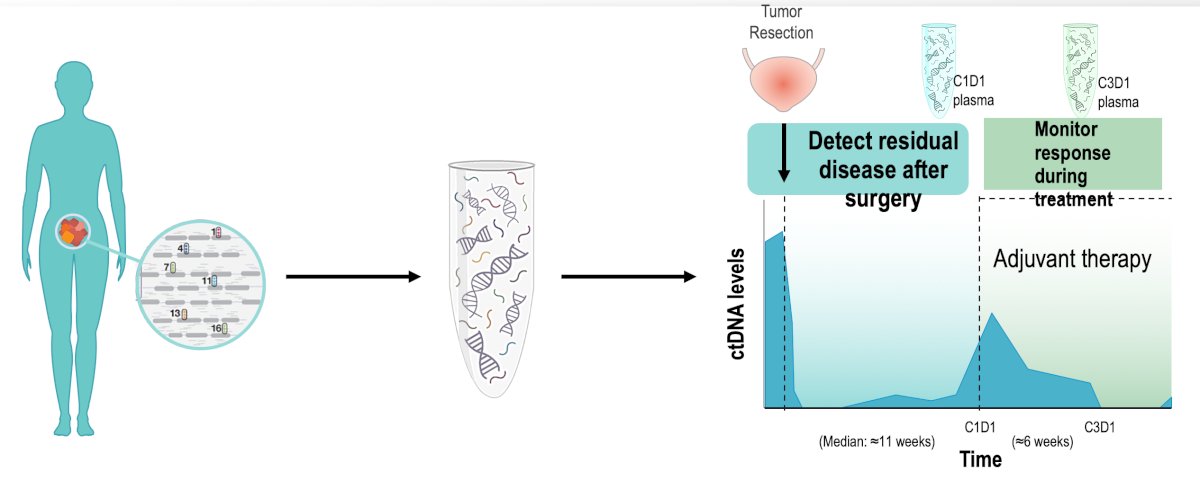
For the remainder of his presentation, Dr. Meeks discussed ctDNA, which, in his opinion, is the most important biomarker for muscle-invasive bladder cancer. ctDNA are small pieces of DNA that originate from cancerous cells and tumors. As a tumor grows, cells die and get broken down, releasing their cellular contents (including DNA) into the bloodstream. The amount of ctDNA that is detectable in the blood varies among individuals and will depend on the type of tumor, its location, and the stage of the tumour it comes from. ctDNA testing, also known as liquid biopsy, can be helpful in detecting and diagnosing a tumor, guiding more tailored, tumor-specific treatment, monitoring the effectiveness of a given treatment, and monitoring cancer recurrence:
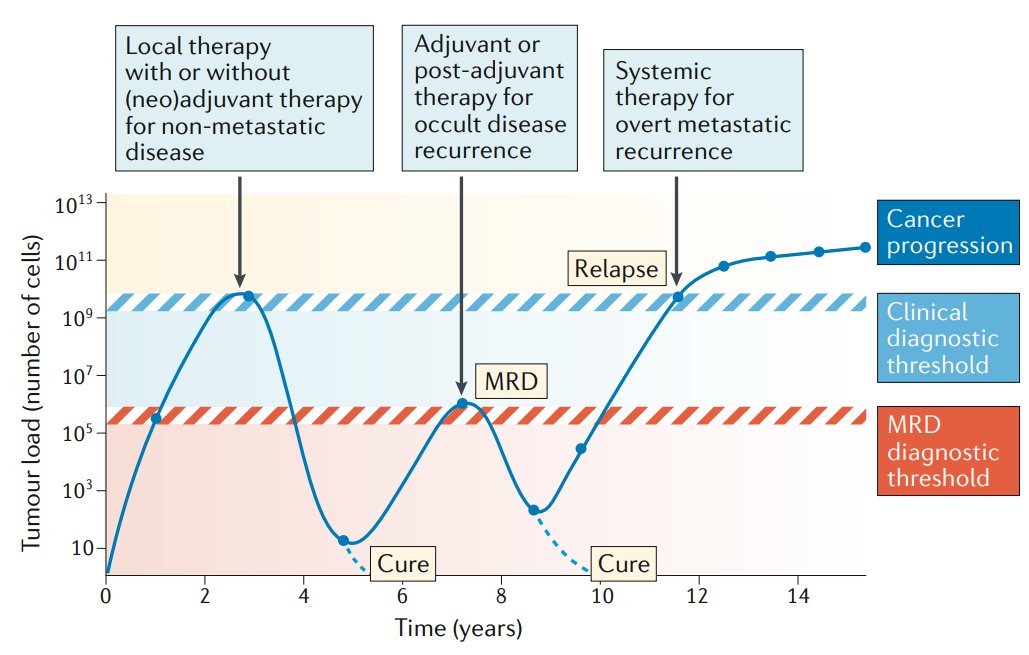
ctDNA dynamics can be used to assess disease burden in real-time, which can help to inform treatment decisions along the continuum of care:
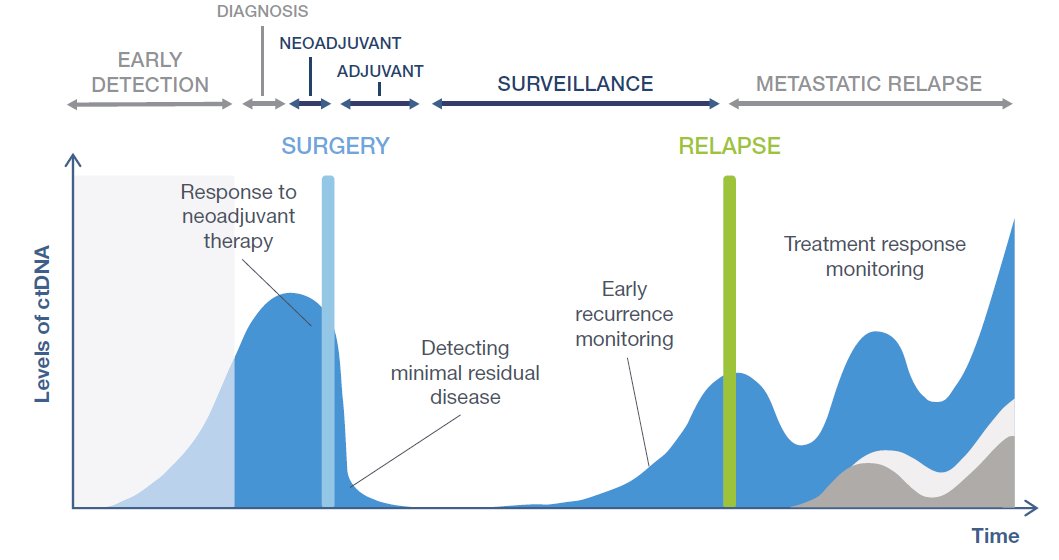
Minimal (or molecular) residual disease refers to persistent cancer after treatment that cannot be detected with current imaging tools (ie. occult metastatic disease), which has previously been widely used in hematological malignancies. However, minimal residual disease may also be used in solid malignancies to more accurately monitor tumor burden levels:
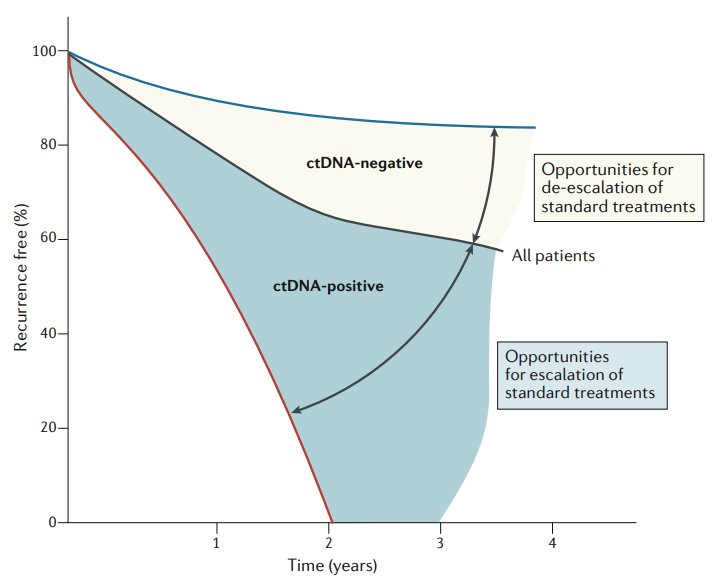
Detectable ctDNA after surgery or adjuvant therapy is strongly associated with a high risk of recurrence. Thus, ctDNA clearance should be evaluated as a surrogate endpoint in trials involving adjuvant therapy. The goal for the future is to personalize the duration of treatment based on ctDNA dynamics:
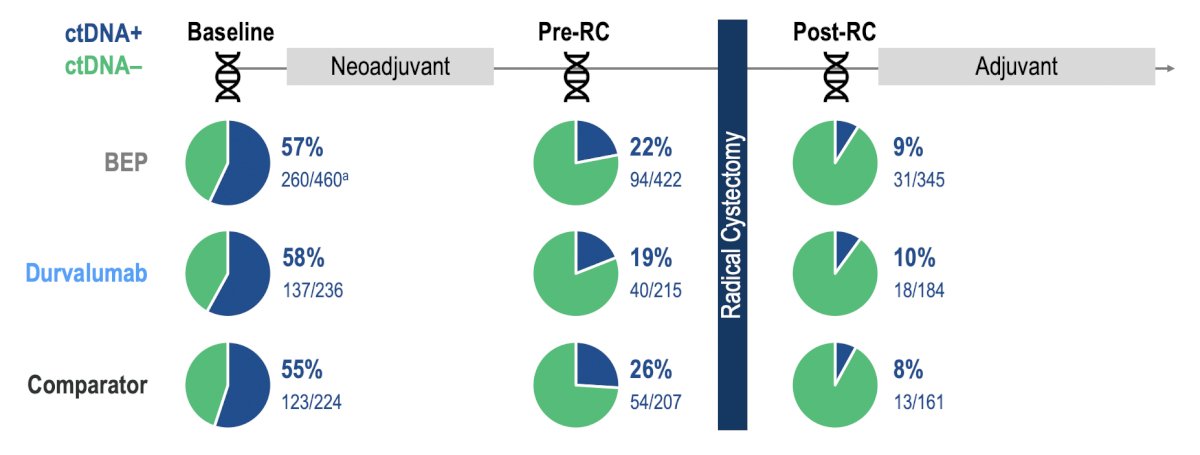
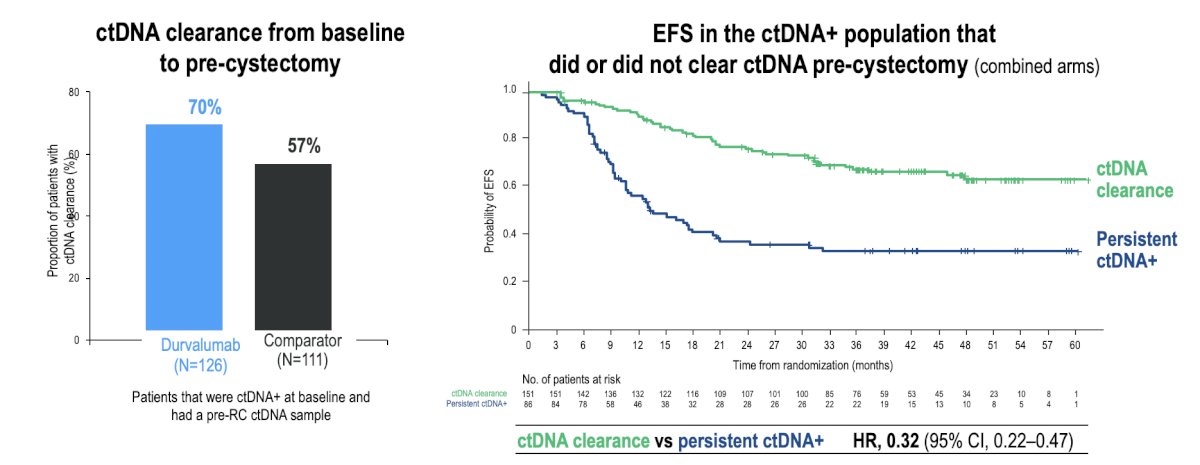
In NIAGARA, the ctDNA+ rate at baseline was 57% (260/460) and decreased to 22% (94/422) after neoadjuvant treatment at pre-radical cystectomy. ctDNA clearance rates from baseline to pre-radical cystectomy were 39% in the durvalumab arm and 29% in the comparator arm. Overall, the ctDNA+ rate post-radical cystectomy was 9% (31/345):
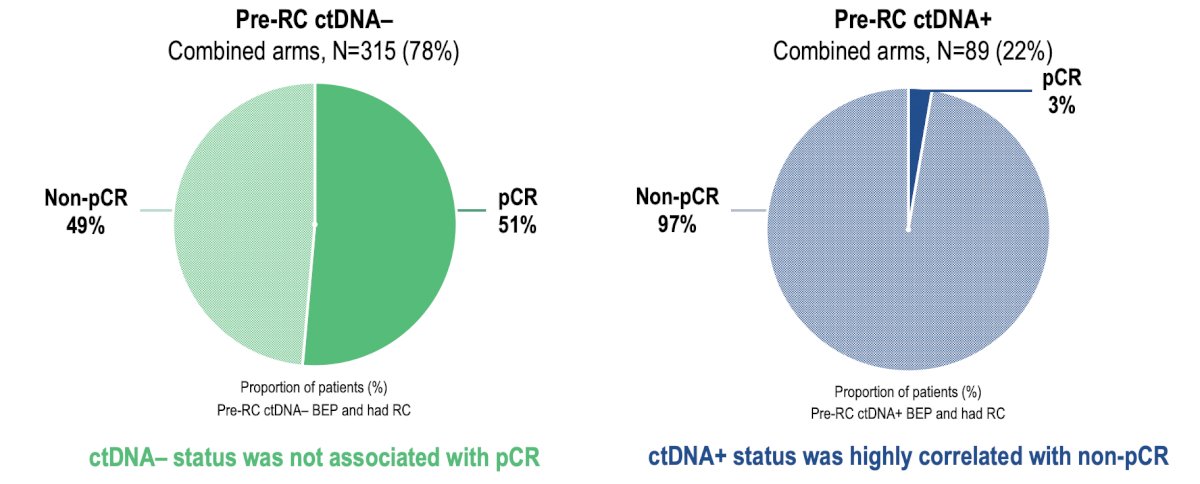
Pre-radical cystectomy ctDNA- status was not associated with pathological complete response; however, ctDNA+ status was highly correlated with non-pathological complete response:
Additionally, ctDNA clearance was higher in the durvalumab arms and prognostic for event-free survival (HR 0.32, 95% CI 0.22-0.47):
Previously, in the phase 3 IMvigor010 trial,5 adjuvant atezolizumab did not provide a significant disease-free survival or overall survival benefit to unselected patients with muscle-invasive bladder cancer:
![Previously, in the phase 3 IMvigor010 trial [5], adjuvant atezolizumab did not provide a significant disease-free survival or overall survival benefit to unselected patients with muscle-invasive bladder cancer:](/images/com-doc-importer/240-lugpa-2025/lugpa-2025-mibc---what-you-should-be-doing-today-and-what-we-will-be-doing-tomorrow/image-22.jpg)
Even though IMvigor010 was a negative trial, a vigorous ctDNA collection program was included in the trial, with the following key steps:
- Tumor tissue and germline material were sequenced (whole exome sequencing)
- Up to 16 mutations for personalized PCR ctDNA were identified for each patient
- Plasma samples were sequenced to ~100,000x
- If 2+ mutations were detected, the sample was defined as ctDNA positive
- The minimal residual disease sample time point before adjuvant treatment (C1D1) was collected
- On treatment samples (C3D1; week 6) were also collected
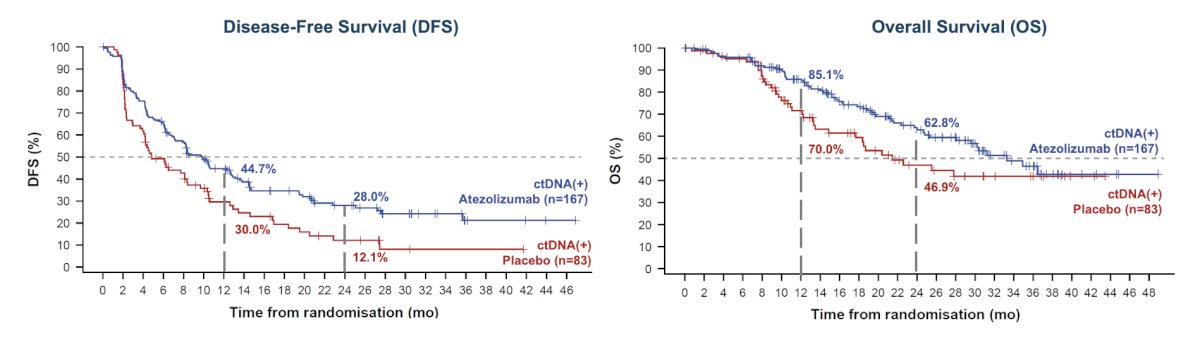
Based on the ctDNA collection in IMvigor010, an exploratory analysis demonstrated that patients who tested ctDNA+ after cystectomy benefited from adjuvant atezolizumab (overall survival HR 0.59), while patients who tested ctDNA– did not (overall survival HR 1.31):6

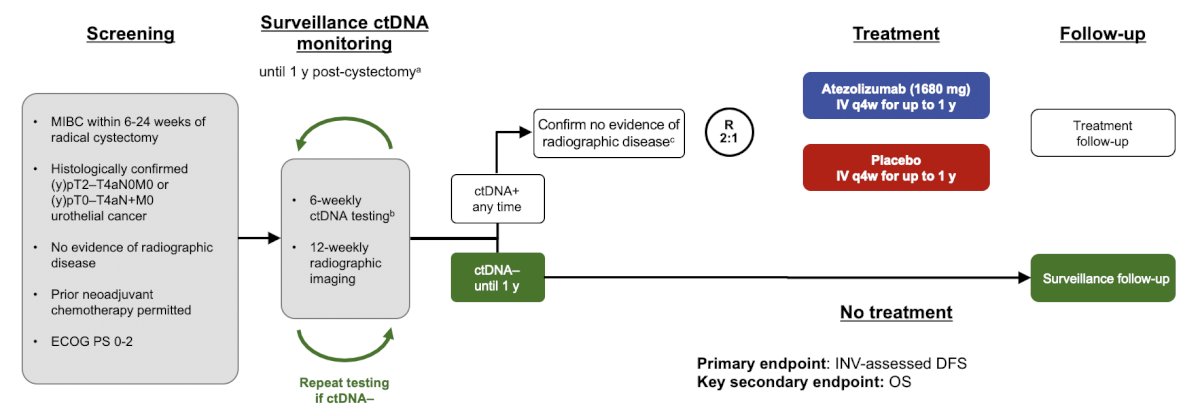
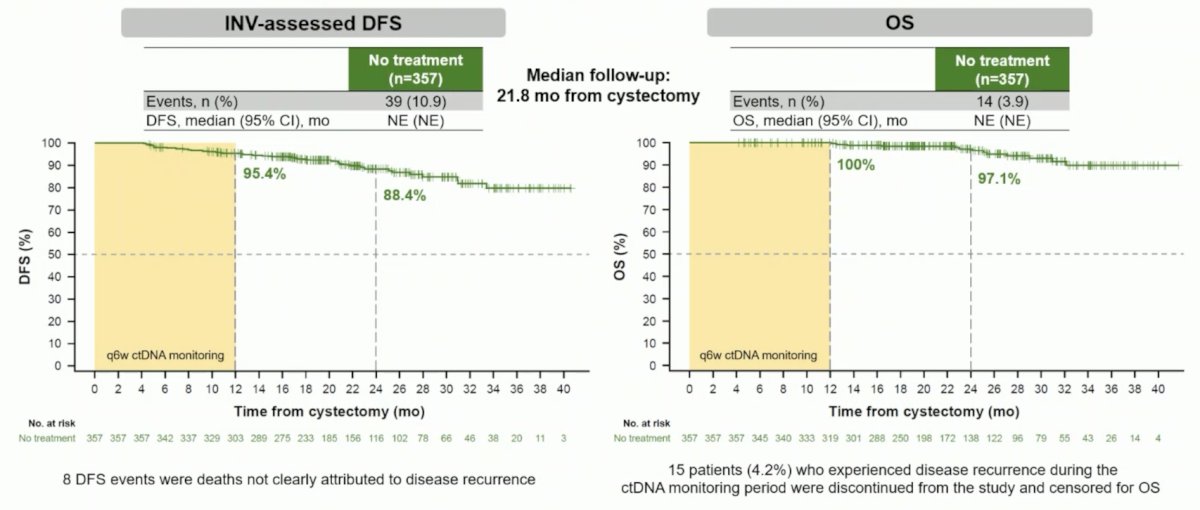
These results from IMvigor010 informed the trial design for IMvigor011, the first minimal residual disease-informed phase 3 study with registrational intent assessing clinical outcomes in high-risk and post-cystectomy muscle invasive bladder cancer patients, informed by ctDNA status on serial testing:
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter
References:
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(1):1773-1786.
- Pfister C, Gravis G, Flechon A, et al. Perioperative dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin in muscle-invasive bladder cancer (VESPER): Survival endpoints at 5 years in an open-label, randomized, phase 3 trial. Lancet Oncol. 2024 Feb;25(2):255-264.
- Parekh DJ, Reis IM, Castle EP, et al. Robot-assisted radical cystectomy versus open radical cystectomy in patients with bladder cancer (RAZOR): An open-label, randomized, phase 3, non-inferiority trial. Lancet 2018 Jun 23;391(10139):2525-2536.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021 Jun 3;384(22):2102-2114.
- Bellmunt J, Hussain M, Gschwend JE, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): A multicentre, open-label, randomized, phase 3 trial. Lancet Oncol. 2021 Apr;22(4):525-537.
- Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021 Jl;595(7867):432-437.