Treatment guidelines for metastatic UC (mUC) recommend platinum-based chemotherapy (cisplatin or carboplatin) as the first-line (1L) standard of care, with PD-1/L1 inhibitors as the second-line (2L) treatment following disease progression or as an alternative 1L option for platinum-ineligible patients.5,6 Treatment guidelines for mUC have evolved over time, initially with the introduction of avelumab as a 1L maintenance therapy for patients who do not progress after 1L platinum-based chemotherapy (ESMO 2022 update).5 More recently, a significant paradigm shift has positioned enfortumab vedotin plus pembrolizumab as the preferred 1L treatment for all eligible patients, regardless of their eligibility for platinum-based chemotherapy (ESMO 2024 update).6
Real-world data suggest that access to, or initiation of, 1L treatment may be suboptimal despite the strength of evidence in treatment guidelines, with even fewer patients initiating later lines of therapy. A small real-world study showed that while >80% of patients in Europe may start with platinum-based chemotherapy, of those patients who eventually received third-line (3L) treatment, nearly half receive only the best supportive care.7 This is supported by US retrospective data demonstrating that more than 25% of patients with mUC in the United States may not receive 1L systemic treatment at all.8 These findings demonstrate a disconnect between available evidence and advances in therapy and highlight the need for a comprehensive characterization of real-world treatment patterns in mUC to address challenges related to guideline adherence and education, access to innovative medicines with improved outcomes, and positioning and recognition of optimal treatment sequencing in an effort to improve patient care and outcomes.
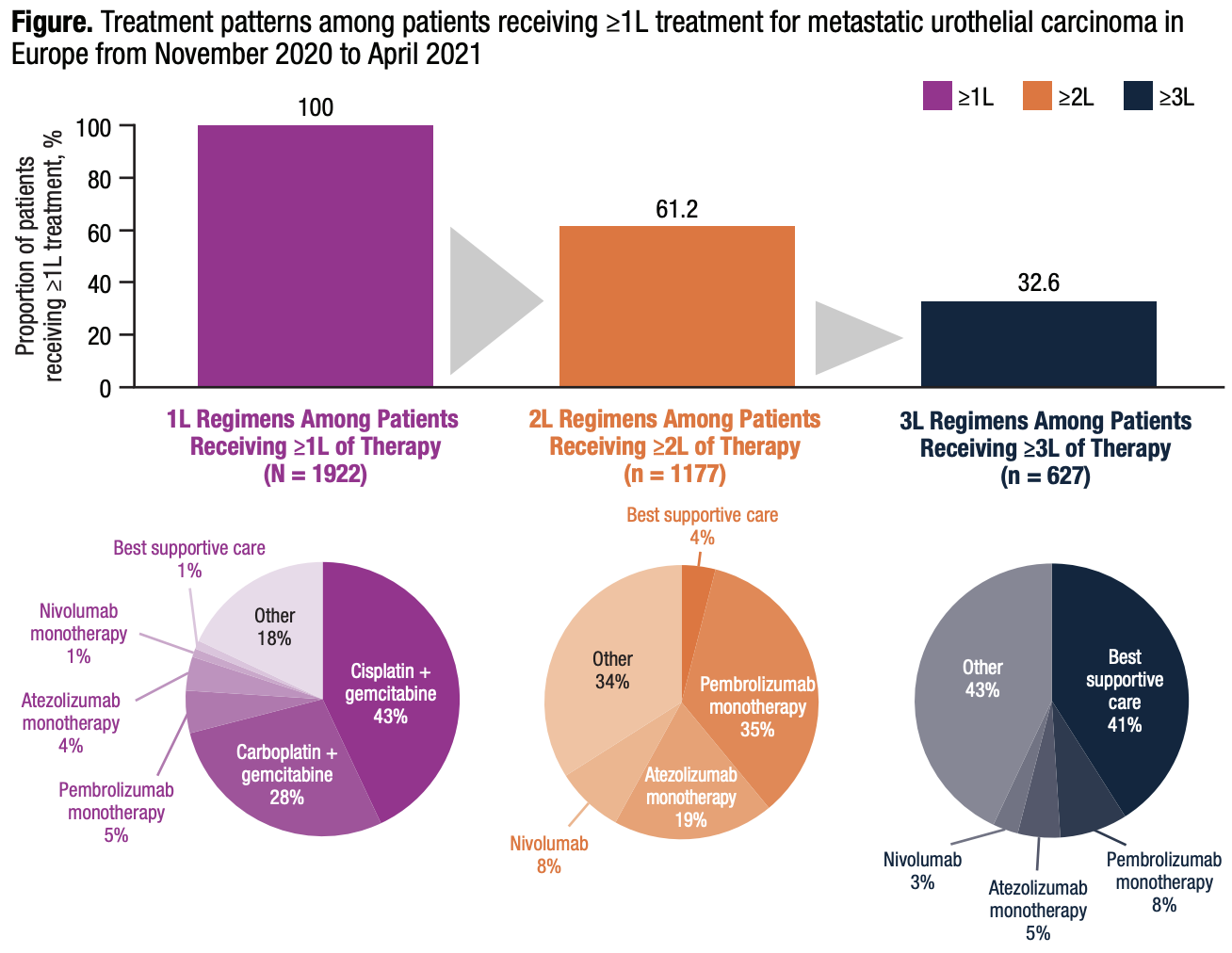
In this cross-sectional survey study, we assessed responses from 232 physicians in France, Germany, Italy, Spain, and the United Kingdom, which provided data on treatment patterns for 1922 patients with mUC. Data were derived from the Adelphi mUC Disease Specific Programme™ covering November 2020 to April 2021. According to the physician-provided data, most patients received 1L platinum-based chemotherapy followed by PD-1/L1 inhibitors in 2L therapy, in accordance with treatment guidelines at the time (Figure), though specific regimen use varied by country. Few patients received PD-1/L1 inhibitors as 1L therapy, suggesting adherence to guidelines that recommended reserving these treatment options for platinum-ineligible patients.
Additionally, consistent with findings from the previous analysis using the same sample of physicians reported in Milloy et al., of the patients who received 3L therapy (n = 627), a substantial portion (n = 254; 41%) received only the best supportive care, indicating a high unmet need for more effective treatment options in this setting.
In this study, physicians reported that just 1% (n = 26) of patients did not receive 1L systemic therapy; however, because the study was based on physician survey responses and therefore likely based on data from patients actively seeking treatment, the proportion of patients receiving supportive care alone may be underestimated. It should also be noted that newer treatments that were approved and/or included in guideline recommendations after April 2021, such as enfortumab vedotin in combination with pembrolizumab as a preferred 1L therapy and avelumab maintenance for patients not progressing after 1L platinum-based chemotherapy, are not reflected in this analysis due to the study cutoff date. Our study did find that a few patients (n = 23) received avelumab maintenance, as the marketing authorization date in Europe (December 2020) fell just within the study time frame; however, this is likely not reflective of current patterns of use.
With this continuously evolving treatment landscape, studies evaluating the impact of the updated recommendations on treatment patterns and outcomes will be critical to understanding current management approaches for patients with locally advanced or mUC in real-world clinical practice. For example, the EVOLVE 2 study, which evaluated treatment patterns in patients with mUC in France from January 1, 2020, to December 31, 2022, and used data extracted from the French hospital discharge database, showed that 64.5% of patients received only 1L therapy.9,10 From 2020 to 2022, avelumab maintenance was reported in 11.9% to 19.3% of patients, indicating modest adoption of the ESMO 2022 updated guidelines. Further studies are needed to evaluate the impact of the 2024 guideline updates, including the recommendation for 1L enfortumab vedotin in combination with pembrolizumab, on real-world treatment patterns.
Written by: Torsten Strunz-McKendry, PhD, Astellas Pharma Europe Ltd., Addlestone, UK
Medical writing support from Bethany Reinecke, PhD, CMPP of Lumanity Scientific Inc., funded by Astellas Pharma Inc.
References:
- Saginala K, Barsouk A, Aluru JS, et al. Epidemiology of bladder cancer. Med Sci (Basel). 2020;8(1):15.
- Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Explorer: An interactive website for SEER cancer statistics [Internet]. National Cancer Institute
- Cancer Research UK. Bladder cancer survival [Internet]. London: Cancer Research UK
- Ripoll J, Ramos M, Montaño J, et al. Cancer-specific survival by stage of bladder cancer and factors collected by Mallorca Cancer Registry associated to survival. BMC Cancer. 2021;21(1):676.
- Powles T, Bellmunt J, Comperat E, et al. Bladder cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(3):244–258.
- Powles T, Bellmunt J, Comperat E et al. ESMO clinical practice guideline interim update on first-line therapy in advanced urothelial carcinoma. Ann Oncol. 2024;35(6):485–490.
- Milloy N, Kirker M, Unsworth M, et al. Real-world analysis of treatment patterns and platinum-based treatment eligibility of patients with metastatic urothelial cancer in 5 European countries. Clin Genitourin Cancer. 2024;22(1):e136–e147.
- Geynisman DM, Broughton E, Hao Y, et al. Real-world treatment patterns and clinical outcomes among patients with advanced urothelial carcinoma in the United States. Urol Oncol. 2022;40(5):195.e1–195.e11.
- Lobbedez FJ, Roupret M, Culine S, et al. 2001P Epidemiology and treatment patterns of patients with locally advanced or metastatic urothelial cancer in France: a non-interventional database study. Ann Oncol. 2024;35 (suppl 2): S1157.
- Tricotel A, Casarotto E, Minacori R, et al. Treatment patterns, healthcare resource utilization, and costs of patients with locally advanced and metastatic urothelial cancer in France: a non-interventional database study. Value in Health. 2024;27(12):s2.