In DISS, the working channel (WC) diameter plays a pivotal role in the system's overall performance. A fine and homogeneous dusting pattern is essential to enable efficient aspiration of stone particles and to prevent obstruction of the working channel. Maaden et al. demonstrated that integrated suction achieved 100% clearance of stone dust particles smaller than 250 μm, and that real-time endoscopic clearance rates were significantly faster compared with manual aspiration alone (3.01 g/min vs. 0.41 g/min) for particles ranging between 125 and 250 μm.2 These findings may challenge the traditional definition of ‘stone dust’,3 as performing an effective DISS procedure requires the generation of finer particles to facilitate continuous suction and prevent channel obstruction. Consequently, achieving a ‘real dusting’ becomes essential not only for optimizing laser efficiency but also for ensuring the proper function of the integrated suction system. This hypothesis underscores the importance of using a laser with very low peak power to achieve a micro dusting effect.4 Considering that true dusting likely corresponds to particles between 125 and 250 µm, the use of a laser with very low peak power, such as the thulium fiber laser (TFL) or the Ho:YAG Magneto, may represent a preferable option to optimize the performance of integrated in-scope suction systems.
Producing smaller and more homogeneous particles minimizes the risk of working channel obstruction, thereby allowing continuous aspiration and efficient renal clearance. Such optimization not only enhances postoperative outcomes but also helps prevent a rise in intrarenal pressure, which may occur if the working channel becomes blocked because it serves simultaneously for both irrigation and suction. By maintaining an unobstructed flow, the system can operate safely and effectively, reducing the likelihood of serious postoperative complications. The TFL should be considered the primary laser for use in an ideal DISS. This is because TFL, often referred to as a “dust laser”, produces microdust particles (<150 μm),5 thereby reducing the risk of suction channel blockage during DISS procedures. This concept can also be extrapolated to the ablative effect achieved by the new Magneto Ho:YAG laser pulse modulation technology. This innovation, integrated into high-power holmium laser platforms (CyberHo, Quanta System, Samarate, Italy), is specifically designed to improve lithotripsy performance, enhancing dusting efficacy while minimizing stone retropulsion. The Magneto mode accomplishes this by extending pulse duration up to 2000 μs and markedly reducing the Ho:YAG peak power to 500 W.6
Pre-stenting before retrograde intrarenal surgery (RIRS) remains a matter of debate, with studies and clinical guidelines providing differing recommendations. Several studies have concluded that pre-stenting is not always required if the procedure is performed carefully, as RIRS remains anatomically and physiologically safe without it.7 Historically, emphasis has been placed on the feasibility of performing sheathless RIRS. However, this approach has faced criticism, particularly due to concerns about elevated intrarenal pressure during procedures performed without a sheath, despite there are some reports that reported similar postoperative outcomes.8 In this context, DISS represents an attractive alternative for endourologists aiming to perform procedures without a UAS or in cases where the FANS cannot be introduced. Through intermittent suction, DISS could at least help mitigate intrarenal pressure, thereby enhancing procedural safety.
Therefore, this study aimed to evaluate the feasibility, safety, and effectiveness of DISS in non-prestented and sheathless flexible ureteroscopy.
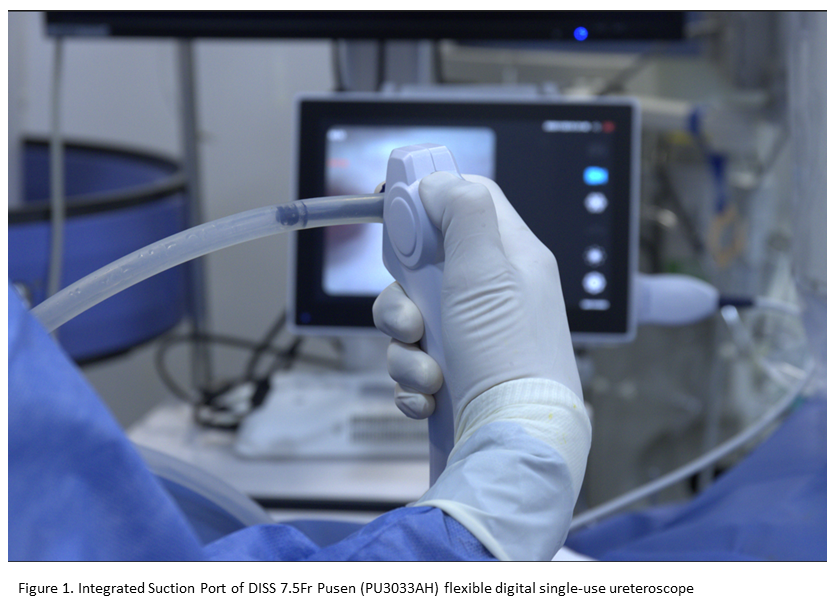
A retrospective analysis was conducted on consecutive patients who underwent DISS procedures at Hospital Alemán of Buenos Aires between March 2025 and September 2025. We included only patients who underwent DISS without the use of a UAS and who did not have a pre-existing ureteral stent. Additionally, we included cases initially planned with FANS in which an intraoperative change of strategy was required, switching to DISS due to the inability to introduce the sheath into the ureter or the renal pelvis. It is noteworthy that the availability of a ureteroscope with integrated suction has significantly modified our usual clinical practice. In the past, patients in whom UAS insertion was unsuccessful typically underwent placement of a double-J stent and were rescheduled for a subsequent procedure. With the introduction of the integrated suction ureteroscope, our current approach is to attempt renal stone treatment during the same session by inserting a 7.5Fr ureteroscope and performing a sheathless procedure with in-scope suction. Although DISS was performed in cases where the FANS could not be used due to the inability to advance the sheath into the ureter, we excluded patients with complex or large-volume renal stones. In such cases, DISS was carried out as an initial or staged procedure; however, these patients were not included in the present analysis in order to avoid confounding the final outcomes. The DISS 7.5Fr Pusen™ (PU3033AH) is a single-use digital flexible ureteroscope with a 7.5Fr outer diameter and a 3.6Fr working channel for the insertion of instruments. The system incorporates an integrated suction mechanism that can be activated via a button located on the ventral aspect of the handle, allowing the surgeon to independently regulate both suction and irrigation (Figure 1).
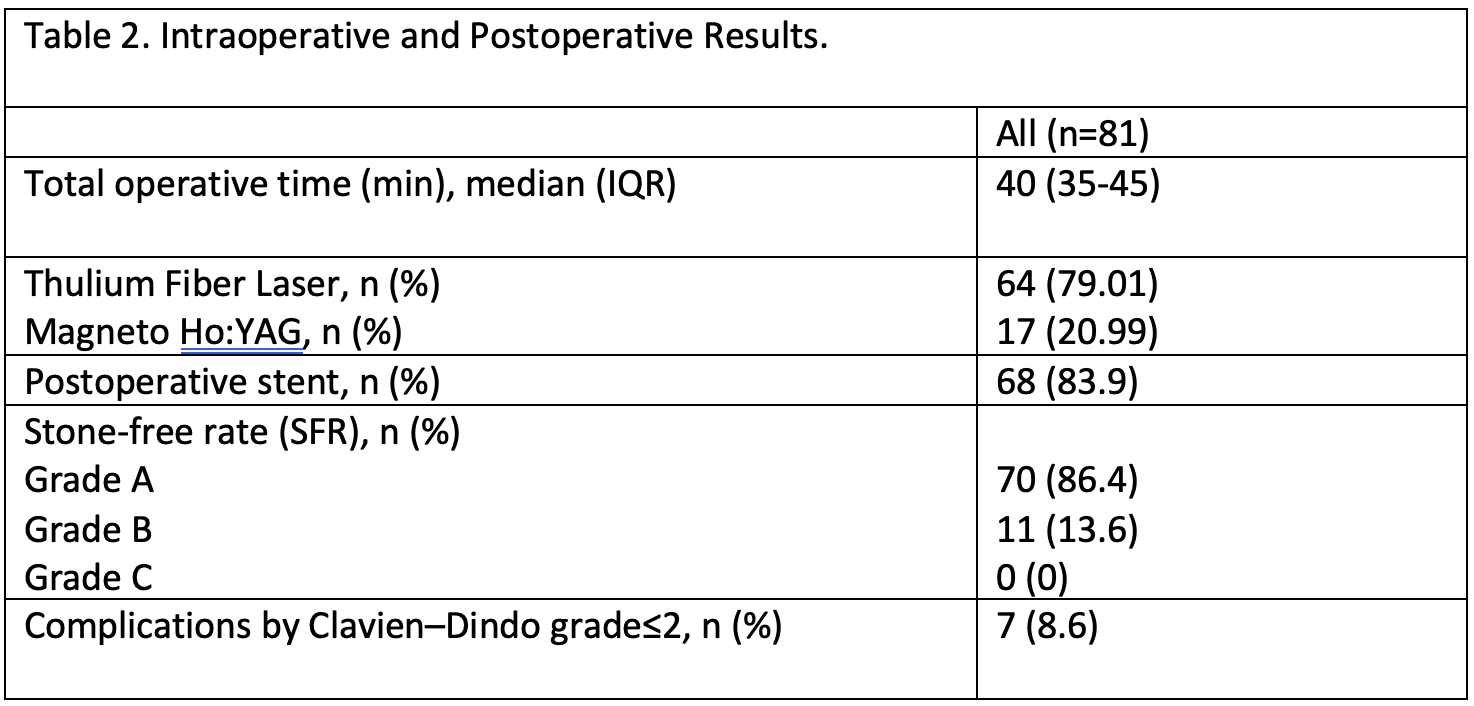
We utilized low peak power lasers in all patients: TFL (Fiber Dust, Quanta System, Samarate, Italy) and Magneto-Ho:YAG laser (CyberHo Magneto, Quanta System, Samarate, Italy). Laser lithotripsy was initiated using low pulse energy settings (typically 0.5–0.6 J, depending on the laser type) and a low frequency (5–10 Hz). Energy and frequency were gradually increased as needed, up to a maximum power of 20 W, according to intraoperative visibility and the degree of impairment caused by stone dust. SFR was assessed using non-contrast abdominal computed tomography (NCCT) performed four weeks postoperatively and categorized into three grades: Grade A, absolute stone-free, defined as the absence of residual fragments on CT scan; Grade B, relative stone-free, corresponding to Grade A plus residual fragments ≤2 mm; and Grade C, relative stone-free with fragments measuring 2.1–4 mm.

BMI body mass index, HU Hounsfield units, IQR: interquartile range.

eGFR = estimated glomerular filtration rate.
Beyond technical feasibility, the main clinical relevance of DISS in a sheathless and non-prestented setting lies in its potential to avoid routine pre-stenting or staged procedures in selected patients. In daily practice, failed UAS insertion traditionally leads to aborting the procedure and placing a double-J stent, exposing patients to additional anesthesia, costs, radiation, and stent-related morbidity. The availability of an integrated suction ureteroscope allows stone treatment to be attempted during the same session while maintaining adequate visualization and fragment evacuation, potentially reducing the need for secondary procedures.
In conclusion, DISS without the use of a ureteral access sheath and no preoperative double-J stent placement is effective and safe in non-complex kidney stones. Further clini¬cal trials are needed to reaffirm the results obtained in this initial experience.
Written by: Luis Rico, Department of Urology, Hospital Alemán, Buenos Aires, Argentina.
References:
- Gauhar V, Somani BK, Heng CT, Gauhar V, Chew BH, Sarica K, Teoh JY, Castellani D, Saleem M, Traxer O. Technique, Feasibility, Utility, Limitations, and Future Perspectives of a New Technique of Applying Direct In-Scope Suction to Improve Outcomes of Retrograde Intrarenal Surgery for Stones. J Clin Med. 2022 Sep 27;11(19):5710. doi: 10.3390/jcm11195710.
- Madden A, Altez C, Lueza JP, Popescu RI, Cabrera J, Corrales M, Traxer O. Direct in-scope suction: an in vitro evaluation of a single use flexible ureteroscope with integrated suction capability. World J Urol. 2024 Sep 1;42(1):500. doi: 10.1007/s00345-024-05203-x.
- Keller EX, De Coninck V, Doizi S, Daudon M, Traxer O. What is the exact definition of stone dust? An in vitro evaluation. World J Urol. 2021 Jan;39(1):187-194. doi: 10.1007/s00345-020-03178-z. Epub 2020 Apr 8.
- Kartalas Goumas I, Panthier F, De Coninck V, Salonia A, Traxer O, Ventimiglia E. Thulium Fiber Laser and the Quest for Optimal Laser Parameters: May Peak Power Be the Answer? J Endourol. 2024 May;38(5):531-532. doi: 10.1089/end.2023.0409. Epub 2024 Apr 1.
- Corrales M, Traxer O. Initial clinical experience with the new thulium fiber laser: first 50 cases. World J Urol. 2021 Oct;39(10):3945-3950. doi: 10.1007/s00345-021-03616-6. Epub 2021 Feb 15.
- Rico L, Blas L, Jaramillo JÁ, Filgueira G, Soldano J, Contreras P. Magneto Ho:YAG laser versus Thulium Fiber Laser for laser lithotripsy during flexible ureteroscopy with a flexible and navigable ureteral access sheath. Int Urol Nephrol. 2025 Oct 10. doi: 10.1007/s11255-025-04819-1.
- Jahrreiss V, Gauhar V, Traxer O, Fong KY, Bin Hamri S, Tan K, Malkhasyan V, Persaud S, Elshazly M, Kamal W, Yuen S, Sridharan V, Castellani D, Gökce MI, Gadzhiev N, Ragoori D, Soebhali B, Chai CA, Tursunkulov AN, Tanidir Y, Tefik T, Shrestha A, Zawadzki M, Lakmichi MA, Seitz C, Somani BK. Influence of pre-stenting on flexible and navigable suction (FANS) access sheath outcomes. Results of a prospective multicentre study by the EAU Section of Endourology and the global FANS collaborative group. Cent European J Urol. 2025;78(1):85-93. doi: 10.5173/ceju.2024.0197. Epub 2024 Nov 28.
- Damar E, Senocak C, Ozbek R, Haberal HB, Sadioglu FE, Yordam M, Bozkurt OF. Does ureteral access sheath affect the outcomes of retrograde intrarenal surgery: a prospective study. Minim Invasive Ther Allied Technol. 2022 Jun;31(5):777-781. doi: 10.1080/13645706.2021.1941117.