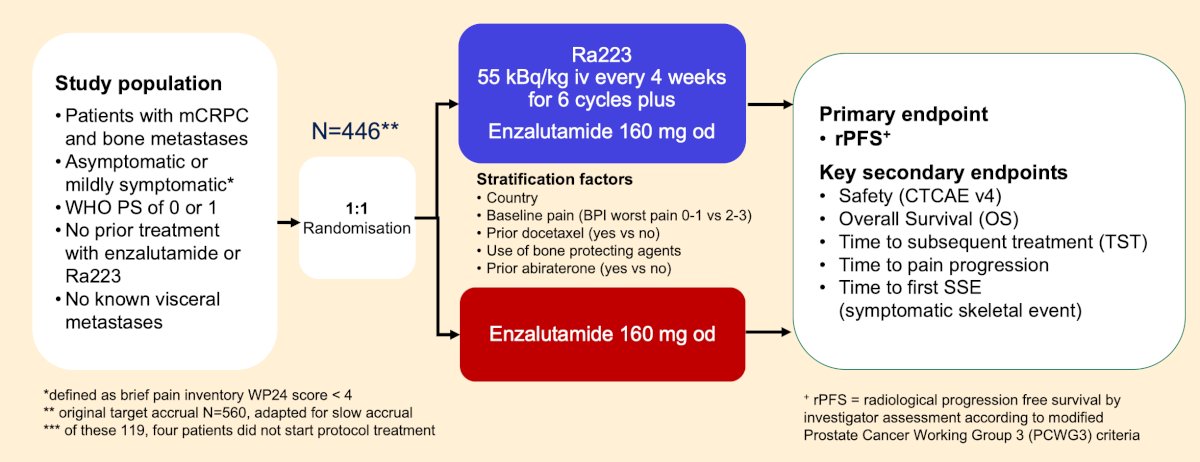
(UroToday.com) The 2025 EAU annual meeting featured a prostate cancer session and a presentation by Dr. Fred Saad discussing a subgroup analysis of the PEACE 3 phase III trial assessing the impact of bone-protecting agents on the efficacy and safety of enzalutamide versus a combination of radium-223 and enzalutamide in asymptomatic or mildly symptomatic patients with bone metastatic castration-resistant prostate cancer (mCRPC). PEACE-3 was an international study in 446 patients with mCRPC and bone metastases randomized 1:1 to a combination of enzalutamide and radium-223 versus enzalutamide alone:
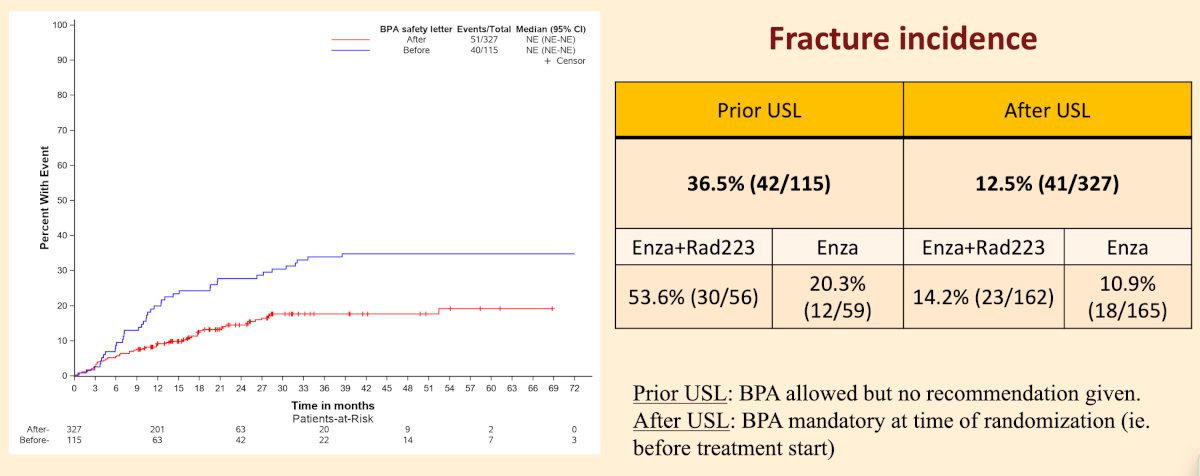
As of March 18, 2018, with 119 (27%) of 446 patients enrolled, an urgent safety letter made co-administration of zoledronic acid or denosumab obligatory. As previously reported, the proportion of patients who experience fractures was reduced from 36.5% to 12.5% with the addition of a bone protecting agents:
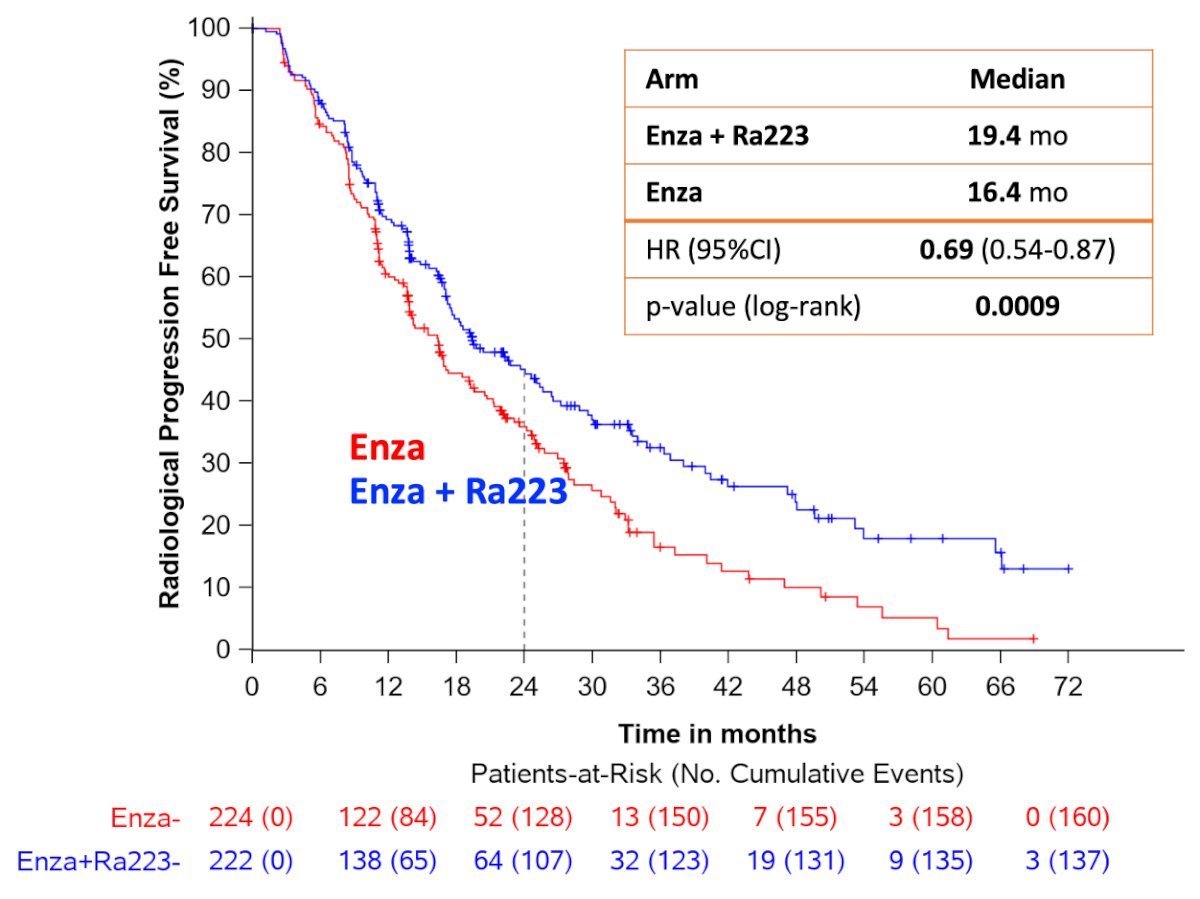
The trial demonstrated significant improvement in the primary endpoint of radiological progression-free survival: HR 0.69 (95% CI 0.54-0.87; p = 0.0009), with a median radiological progression-free survival of 16.4 (95% CI 13.8-19.2) months in the enzalutamide arm and 19.4 (95% CI 17.1-25.3) months in the enzalutamide and radium-223 arm:
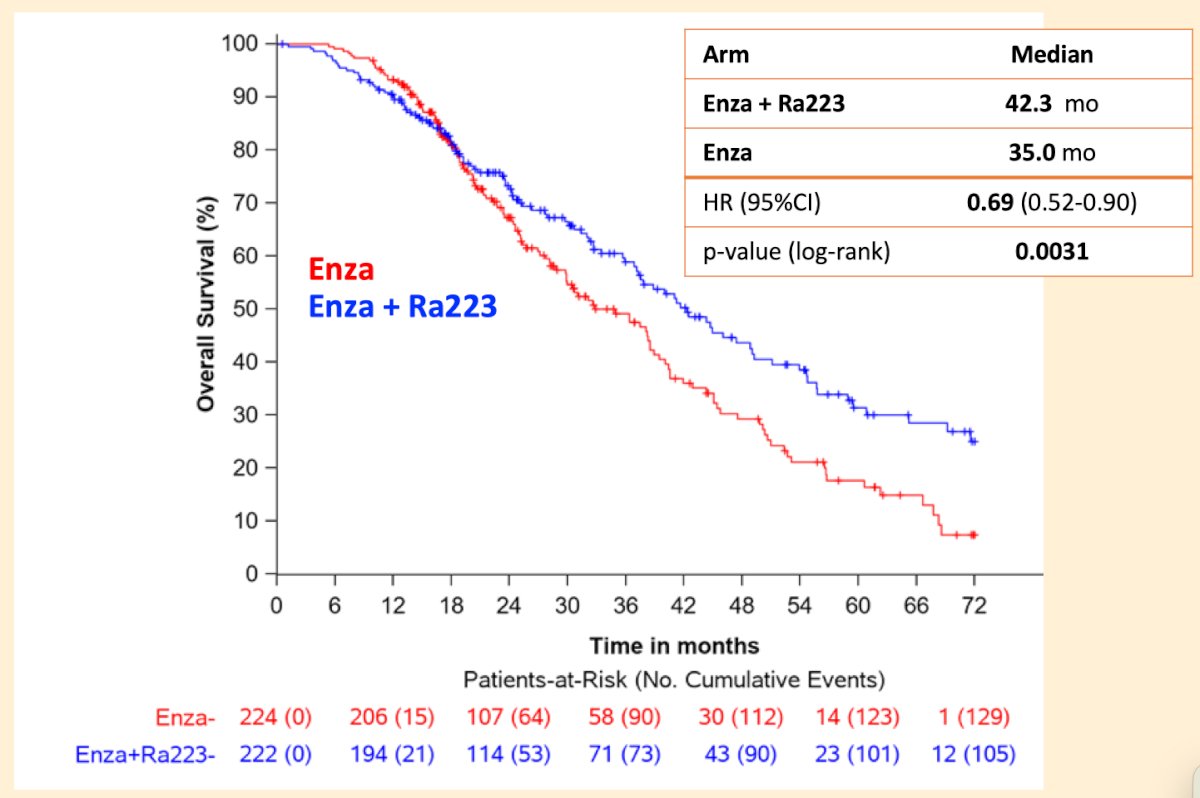
Additionally, the interim analysis (at 80% of events) showed that the key secondary endpoint of overall survival also favored the enzalutamide and radium-223 arm (HR 0.69, 95% CI 0.52-0.90, p = 0.0031):
The objective of this analysis presented at EAU 2025 by Dr. Saad was to determine whether the use of a bone protecting agent added to the therapeutic efficacy of the treatment in the subgroup of patients who were treated with or without bone protecting agents prior to the urgent safety letter.
A total of 115 patients enrolled prior to the urgent safety letter and received protocol treatment were included in this analysis. Of these, 59 (51%) received either no bone protecting agent or only after a fracture had occurred, while 56 (49%) received a bone protecting agent prior and/or during study treatment. Efficacy outcomes included radiological progression-free survival and overall survival.
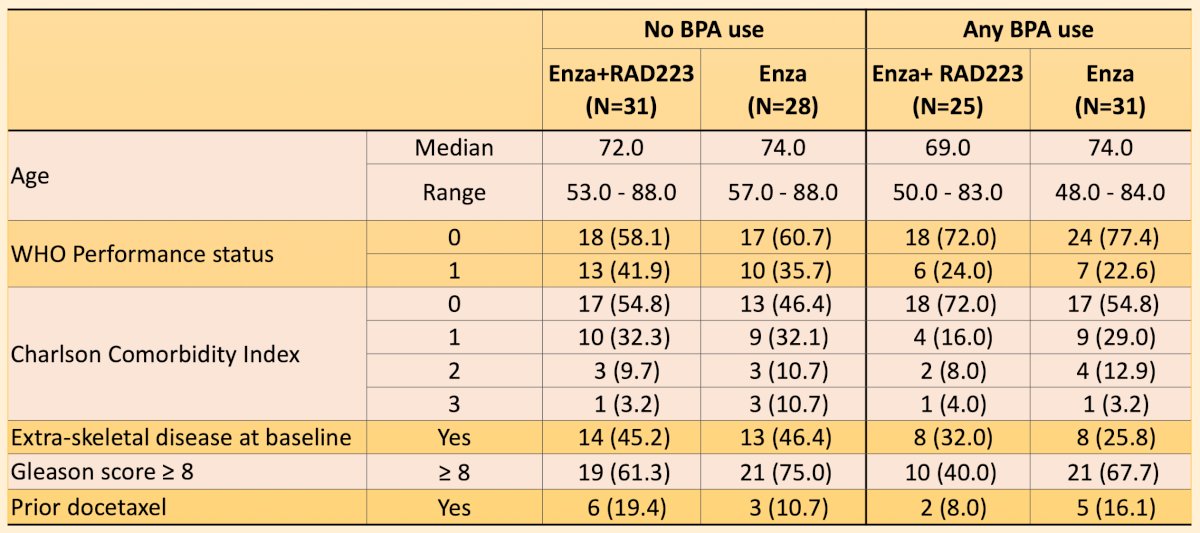
Patients with bone protecting agent use versus no bone protecting agents had similar baseline characteristics:
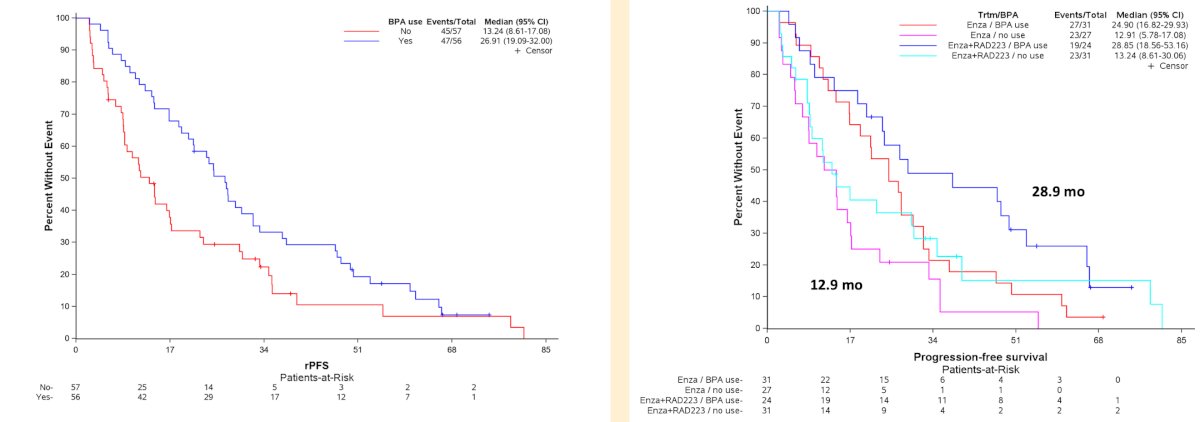
Median enzalutamide treatment duration was 12 months (IQR: 7-27) without and 26 months (IQR: 13-44) with bone protecting agent use. Median radiological progression-free survival was longer by 14 months from 13.24 months without to 26.91 months with bone protecting agents use (HR 0.60, 95% CI 0.39-0.93) and this difference was similar across both arms. Patients in the enzalutamide and radium-223 arm with bone protecting agents had a median radiological progression-free survival of 28.85 months versus only 12.9 months for those in the enzalutamide arm without bone protecting agents:
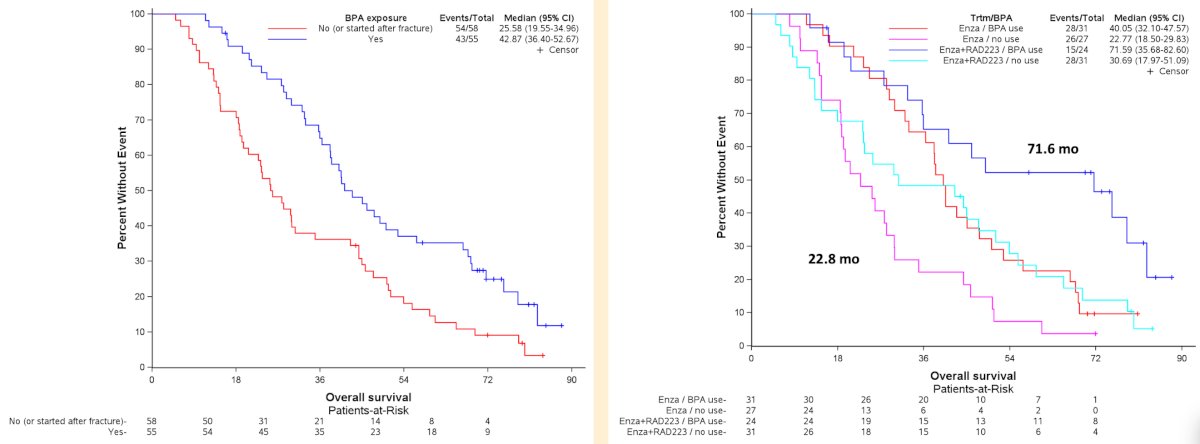
Median overall survival was longer by 17 months from 25.58 months without to 42.87 months with bone protecting agents use (HR 0.56, 95%CI 0.37-0.86). Again, this difference was notable between the enzalutamide and radium-223 arm with bone protecting agents and the enzalutamide arm without bone protecting agents with median overall survival of 71.59 months versus 22.77 months, respectively:
The fracture rate for patients not receiving a bone protecting agent was 49.2% (29/59) versus 23.2% (13/56) receiving any bone protecting agent. Patients without bone protecting agents reported more severe (CTCAE grade ≥3) blood and lymphatic system disorders (10.2% [6/59] versus 1.8% [1/56]) and renal and urinary disorders (8.5% [5/59] versus 1.8% [1/56]) compared to those receiving bone protecting agents.
Dr. Saad concluded his presentation by discussing the impact of bone protecting agents on the efficacy and safety of enzalutamide versus combination of radium-223 and enzalutamide in asymptomatic or mildly symptomatic patients with bone mCRPC with the following take home points:
- In the overall population, radiographic progression free survival was significantly improved with the addition of radium-223 to enzalutamide
- Bone protecting agent use led to a 14 month improvement in radiographic progression free survival (HR 0.60, 95% CI 0.39-0.93)
- There was a similar advantage in both arms
- Enzalutamide and radium-223 with bone protecting agents had a median radiographic progression free survival of 28.9 months versus 12.9 months for enzalutamide arm without bone protecting agents.
- Bone protecting agent use led to a 17 month improvement in overall survival (HR 0.56, 95% CI 0.37-0.86)
- These exploratory findings suggest that bone protecting agents in combination with life prolonging therapeutic options in mCRPC is safe and may provide additional therapeutic benefit
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
Related Content: Bone-Protective Agents and Survival Benefits in PEACE-3 Trial Subgroup Analysis - Fred Saad