CRPC with Bone Metastases
Prevention of Skeletal-Related Events in Advanced Prostate Cancer
Patients with advanced prostate cancer are at significant risk of skeletal-related events (SREs) due to a complex interplay between bone health and prostate cancer due to cancer biology and the predilection of prostate cancer to spread to bone, the toxicity of prostate cancer treatments, and shared epidemiology of the two conditions.
Skeletal-related events are used to denote events related to osseous metastases, including pathologic bone fractures, spinal cord compression, orthopedic surgical intervention, and palliative radiation directed at the bone.1 This definition has been widely used in the design of randomized controlled trials and for drug approval. In some circumstances, authors include a change in systemic anti-neoplastic therapy as a result of bony pain in the definition of skeletal-related events. The key to this definition is that skeletal-related events may be clinically manifested due to symptoms or only radiographically detected. Thus, skeletal-related events may or may not be symptomatic. In contrast, symptomatic skeletal-related events (SSEs) is a relatively newer outcome representing a subset of skeletal-related events which symptomatically affect the patient experience. This outcome was first used in the Alpharadin in Symptomatic Prostate Cancer (ALSYMPCA) trial,2 wherein symptomatic skeletal-related events were defined as bone-directed radiotherapy to relieve bony pain, new symptomatic pathologic fractures, spinal cord compression, or tumor-related orthopedic surgery. While there is a significant overlap between these conditions, there are important differences that relate to both study design and patient care: namely, detection of SREs requires routine radiographic evaluation to detect asymptomatic skeletal-related events while detection of SSEs can be driven by patient evaluation.
Skeletal related events contribute significantly to the disease-related morbidity and mortality of prostate cancer, in addition to being very costly. A range of lifestyle, nutritional, and pharmaceutical interventions can be undertaken to decrease the risk of skeletal-related events in patients with advanced prostate cancer.
Lifestyle and nutrition-based interventions
These recommendations are not unique to patients with prostate cancer, but rather apply to all men with osteoporosis or decreased bone mineral density to reduce the risk of fractures.
The Endocrine Society Clinical Practice Guideline on Osteoporosis in Men recommends the following lifestyle interventions:3
- Calcium intake: it is recommended that men with or at risk for osteoporosis consume 1000 to 1200 mg of calcium daily. While dietary sources are preferable, calcium supplementation should be used if dietary calcium intake is inadequate.
- Vitamin D intake: men with low vitamin D levels (< 30 ng/mL or < 75 nmol/L) should receive vitamin D supplementation to raise serum vitamin D levels to at least these levels.
- Exercise: men at risk of osteoporosis are recommended to participate in weight-bearing activities at least three or four times per week, for 30 to 40 minutes per session.
- Alcohol intake: it is recommended that men at risk of osteoporosis reduce their alcohol intake to fewer than three units of alcohol. One unit of alcohol is defined as 10 mL of pure alcohol. This amount could be found in 25 mL of spirits (40% alcohol by volume), one third to one half a pint of beer (5-6% alcohol by volume), or half a standard glass of wine (12% alcohol by volume).
- Smoking cessation: it is recommended that all men at risk of osteoporosis stop smoking.
The American Urological Association 2018 Amendment of the Castration-Resistant Prostate Cancer similarly endorses preventative therapy in the form of supplemental calcium and vitamin D in men with castration-resistant prostate cancer.4 However, such interventions are likely advisable much earlier in the disease trajectory given the relatively minor risks of these supplements in contrast to the potentially debilitating and costly consequences of skeletal-related events. To this end, the NCCN and the National Osteoporosis Foundation recommend these interventions in all men over the age of 50 years who are receiving androgen deprivation therapy.
Pharmacologic interventions
In addition to calcium and vitamin D as highlighted above, the American Urological Association 2018 Amendment of the Castration-Resistant Prostate Cancer endorses pharmacotherapy with denosumab or zoledronic acid in men with castration-resistant prostate cancer.4
While further indications exist, the Endocrine Society Clinical Practice Guideline on Osteoporosis in Men recommends pharmacologic therapy in men at high risk for fracture based on, but not limited to, the following factors:3
- Men with a history of previous non-traumatic hip or vertebral fracture.
- Men with bone mineral density (T-score) that is 2.5 standard deviations or more below the mean of normal young white men, in the absence of spine or hip fractures.
- Men with a bone mineral density (T-score) from 1.0 to 2.5 standard deviations who also have an increased risk of fracture. In the United States, the suggested criteria for increased risk of fracture are a 10-year risk of any fracture equal to or exceeding 20% or a 10-year risk of hip fracture equal to or exceeding 3%, as determined using the FRAX tool. In other regions, the Guidelines recommend the utilization of region-specific guidelines.
- Men who are receiving long-term glucocorticoid treatment in significant doses defined by the 2010 American Society of Rheumatology as > 7.5 ng per day of prednisone or equivalent.
Pharmaceuticals - bisphosphonates
Bisphosphonates were among the first agents successfully used to prevent skeletal-related events in advanced prostate cancer. They function by reducing bone resorption through a variety of mechanisms including decreased osteoclast differentiation and survival and increased osteoblast survival. To do so, they compete with pyrophosphate for hydroxyapatite crystal binding sites, thus reducing osteoclast adherence to the bone. While there are a number of bisphosphonates used for a variety of clinical indications, zoledronic acid is most commonly used in patients with metastatic prostate cancer due to the Zometa 039 trial which demonstrated a reduction in SREs for patients who received zoledronic acid as compared to placebo.5 Based on these data, zoledronic acid is the only bisphosphonate approved for the prevention of skeletal-related events in men with metastatic prostate cancer.
Pharmaceuticals - denosumab
Denosumab is another agent which targets osteoclast activity. Bone exists in homeostasis between formation (driven by osteoblasts) and resorption (driven by osteoclasts). This homeostasis is regulated by the RANK (receptor activator of nuclear factor κB)/RANK-ligand system. Denosumab is a fully human monoclonal antibody that targets the RANK-ligand by mimicking OPG. Denosumab was first examined in postmenopausal women to prevent the development of osteoporosis and reduce the risk of fracture. Subsequently, denosumab was examined in women with breast cancer. Most relevantly, the Denosumab Protocol 20050103 compared denosumab and zoledronic acid in 1901 men with castrate-resistant prostate cancer.6 After a median follow-up of approximately one year, patients receiving denosumab had a significantly prolonged time to first-SRE (3.6 months incremental benefit, hazard ratio 0.82, 95% confidence interval 0.71 to 0.95). As a result of these data, denosumab was approved for the prevention of SREs in patients with metastatic solid tumors.
Pharmaceuticals – radio-isotopes
In addition to these osteoclast targeting agents, radio-isotopes may be used in the prevention of skeletal-related events. While beta-emitting particles (strontium-89 and samarium-153) may be used in the palliation of disease-related bony pain, they don’t have proven benefit in the prevention of SREs. In contrast, the alpha-emitting particle radium-223 has proven both palliative benefit as well as improvements in time to first SRE and overall survival. In the pivotal ALSYMPCA trial, 922 men with castrate-resistant prostate cancer and at least two symptomatic bony metastases who had either previously received or were unfit to receive docetaxel were randomized to radium-223 or placebo. Patients receiving radium-223 had significant improvements in time to first SRE (incremental benefit 5.2 months) as well as overall survival (incremental benefit in median survival of 2.8 months).2
Approach to preventing skeletal-related events
Philosophically, there are a number of times in the natural history of prostate cancer where a clinician may intervene to reduce the risk of prostate cancer related skeletal-related events. These relate to the complex interplay between prostate cancer and bone disease.
First, treatment may be directed at reducing or preventing fragility fractures due to prostate cancer-related therapy. In this disease space, lifestyle and nutrition-based interventions are paramount and are recommended by AUA guidelines as well as the National Comprehensive Cancer Network (NCCN). Pharmacologic interventions, including the use of osteoclast targeting therapies (bisphosphonates and RANK-ligand inhibitors), should be considered in this setting for patients at increased risk of fragility related fracture. Denosumab is FDA approved for this indication on the basis of the HALT 138 trial which found an increase in bone mineral density and a decrease in vertebral fractures among men receiving ADT for non-metastatic hormone-sensitive prostate cancer who receiving denosumab versus placebo.
Second, treatment may be directed at preventing bone metastases. In this disease space, bone-targeting agents including bisphosphonates and denosumab have been examined. The MRC PR04 trial demonstrated no benefit to clodronate in metastasis-free survival. Unfortunately, the Zometa 704 trial assessing the role of zoledronic acid in men with non-metastatic castration-resistant prostate cancer failed to accrue. However, the ZEUS trial accrued 1393 men with high-risk localized prostate cancer. Treatment with zoledronic acid failed to demonstrate an improvement in bone metastasis compared to placebo.7 The Denosumab Protocol 20050147 randomized men with high-risk nonmetastatic castrate-resistant prostate cancer to denosumab or placebo. Men receiving denosumab had prolonged metastasis-free survival (incremental benefit of 4.2 months).8
However, other approaches utilizing the suppression of the androgen axis in patients with non-metastatic castration-resistant prostate cancer (enzalutamide, apalutamide, and darolutamide) have demonstrated improvements in metastasis-free survival. While not a primary endpoint of these studies, it would be anticipated that delaying metastasis may improve skeletal-related events in these patients.
Third, we may seek to prevent skeletal-related events in men with known metastatic prostate cancer. This applies whether these men are in the castrate-sensitive or castrate-resistant disease space and it is here that the bulk of the evidence for prevention of SREs lies. In men with castrate-sensitive disease, CALGB 90202 demonstrated no improvement in skeletal-related events with the administration of zoledronic acid while castrate-sensitive rather than delayed initiation at the time of castration resistance.9 In contrast, there is significant evidence for the role of bone targeting agents in men with castrate-resistant disease. As previously mentioned, Zometa 039 demonstrated improvements in SREs for men receiving zoledronic acid compared with a placebo. Interestingly, CGP 032 and INT 05 failed to demonstrate a benefit to pamidronate. Thus, zoledronic acid is the only bisphosphonate approved in this space. The Denosumab Protocol 20050103 demonstrated an improvement in time to first SRE, as previously mentioned. Further, radio-isotope therapy using radium-223 was demonstrated in ALSYMPCA to improve time to first SRE in men with castrate-resistant prostate cancer and at least two symptomatic bony metastases.
Written by: Zachary Klaassen, MD, MSc, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md
Published Date: February 2020
- Written by: Zachary Klaassen, MD, MSc
- References:
1. Morgans, Alicia K., and Matthew R. Smith. "Bone-targeted agents: preventing skeletal complications in prostate cancer." Urologic Clinics 39, no. 4 (2012): 533-546.
2. Parker, Christopher, S. Nilsson, Daniel Heinrich, Svein I. Helle, J. M. O'sullivan, Sophie D. Fosså, Aleš Chodacki et al. "Alpha emitter radium-223 and survival in metastatic prostate cancer." New England Journal of Medicine 369, no. 3 (2013): 213-223.
3. Watts, Nelson B., Robert A. Adler, John P. Bilezikian, Matthew T. Drake, Richard Eastell, Eric S. Orwoll, and Joel S. Finkelstein. "Osteoporosis in men: an Endocrine Society clinical practice guideline." The Journal of Clinical Endocrinology & Metabolism 97, no. 6 (2012): 1802-1822.
4. Lowrance, William T., Mohammad Hassan Murad, William K. Oh, David F. Jarrard, Matthew J. Resnick, and Michael S. Cookson. "Castration-resistant prostate cancer: AUA Guideline Amendment 2018." The Journal of urology 200, no. 6 (2018): 1264-1272.
5. Saad, Fred, Donald M. Gleason, Robin Murray, Simon Tchekmedyian, Peter Venner, Louis Lacombe, Joseph L. Chin, Jeferson J. Vinholes, J. Allen Goas, and Bee Chen. "A randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma." Journal of the National Cancer Institute 94, no. 19 (2002): 1458-1468.
6. Fizazi, Karim, Michael Carducci, Matthew Smith, Ronaldo Damião, Janet Brown, Lawrence Karsh, Piotr Milecki et al. "Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study." The Lancet 377, no. 9768 (2011): 813-822.
7. Wirth, Manfred, Teuvo Tammela, Virgilio Cicalese, Francisco Gomez Veiga, Karl Delaere, Kurt Miller, Andrea Tubaro et al. "Prevention of bone metastases in patients with high-risk nonmetastatic prostate cancer treated with zoledronic acid: efficacy and safety results of the Zometa European Study (ZEUS)." European urology 67, no. 3 (2015): 482-491
8. Smith, Matthew R., Fred Saad, Robert Coleman, Neal Shore, Karim Fizazi, Bertrand Tombal, Kurt Miller et al. "Denosumab and bone-metastasis-free survival in men with castration-resistant prostate cancer: results of a phase 3, randomised, placebo-controlled trial." The Lancet 379, no. 9810 (2012): 39-46.
9. Smith, Matthew R., Susan Halabi, Charles J. Ryan, Arif Hussain, Nicholas Vogelzang, Walter Stadler, Ralph J. Hauke et al. "Randomized controlled trial of early zoledronic acid in men with castration-sensitive prostate cancer and bone metastases: results of CALGB 90202 (alliance)." Journal of Clinical Oncology 32, no. 11 (2014): 1143.
Radiopharmaceuticals in Prostate Cancer: Systemic “Bone-Seeking” Agents
Radiopharmaceuticals are pharmaceutical agents containing radioisotopes and emitting radiation that may be used for diagnostic or treatment purposes.
A number of small molecules have been used in conjunction with positron emission tomography (PET) scanning for prostate cancer staging. A recent presentation reported on the role of radiopharmaceutical driven imaging, predominately using Ga-PSMA, from the 2018 American Society of Clinical Oncology Annual Meeting.
From a therapeutic perspective, as they are typically given via intravenous infusion, radiopharmaceuticals are systemic radiotherapies, emitting alpha or beta radiation. Radiopharmaceuticals are indicated in patients with castrate-resistant prostate cancer with symptomatic bone metastases. Historically, beta-particle emitting agents including strontium-89 (Metastron®), samarium-153 (Quadramet®), phosphorus-32, and rhenium-186 were used as palliative therapies for patients with symptomatic bone disease.1 In this context, they are quite effective in relieving bony pain,2 however, these agents did not significantly improve survival.3 In contrast, the ALSYMPCA trial, which will be discussed in more detail below, demonstrated an improvement in both overall survival and skeletal-related events for patients receiving the alpha-emitter radium-223.4
In December 2018, the European Association of Nuclear Medicine Focus 1 Meeting reported a consensus regarding the use of molecular imaging and theranostics in prostate cancer.5 A number of relevant conclusions were derived following a systematic review and modified Delphi process. First, traditional diphosphate bone scan and contrast-enhanced computed tomography scan are mentioned but rarely recommended in the majority of patients in clinical guidelines. Second, magnetic resonance imaging and prostate cancer-targeted positron emission tomography are frequently suggested but the specific clinical scenarios in which they are most useful are poorly defined and how they may affect practice are poorly delineated. Third, sodium fluoride-18 positron emission tomography-CT bone scanning is not widely recommended; however, gallium-68 or fluorine-18 PSMA have gained acceptance. Finally, the palliative use of bone-targeting radiopharmaceuticals strontium-89, samarium-153, and rhenium-186 has been supplanted by radium-223, as well as other systemic therapies including docetaxel, abiraterone acetate, enzalutamide, and cabazitaxel.
Radium-223
Radium-223 dichloride (Xofigo®), commonly referred to as radium-223, is a targeted alpha emitter. It functions as a calcium mimetic and selectively binds newly forming bone stroma in regions of high bone turnover in osteoblastic or sclerotic bone metastasis.6 It then emits high-energy alpha particles with a very short range (less than 100 μm).7 This high-energy radiation induces a highly localized cytotoxic effect due to double-stranded DNA breakage.Initial Phase I and Phase II studies in patients with bone metastasis demonstrated radium-223 to be well tolerated, with minimal myelosuppression.8,9 Phase II trials also demonstrated that radium-223 effectively reduced bone-related pain and improved disease-related biomarkers, including bone alkaline phosphatase and prostate-specific antigen (PSA).9
As a result, the Phase III, Alpharadin in Symptomatic Prostate Cancer Patients (ALSYMPCA) trial was undertaken to assess the efficacy of radium-223 versus placebo in patients with metastatic castration-resistant prostate cancer (mCRPC) and bone metastases across 136 study centers in 19 countries.4 The trial enrolled patients with two or more bone metastases, detected on skeletal scintigraphy, without visceral metastasis who had previously received docetaxel, were docetaxel ineligible or declined docetaxel. Patients were required to have symptomatic disease, based on the requirement for regular analgesics or prior treatment with external beam radiotherapy for cancer-related bone pain in the preceding 12 weeks. Additionally, patients had to have a baseline PSA of at least 5 ng/mL with at least two progressive PSA rises; an Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 2; life expectancy of at least six months; and adequate hematologic, renal and liver function. Patients who had received chemotherapy within the preceding four weeks were excluded.
A total of 921 patients were enrolled and were randomized in a 2:1 ratio to radium-223 (50 kBq per kilogram of body weight intravenously), once every four weeks, plus best standard of care or placebo plus best standard of care.
The primary study endpoint was overall survival and secondary outcomes included time to first symptomatic skeletal event; biochemical endpoints including time to increase in total alkaline phosphatase level, total alkaline phosphatase response, normalization of alkaline phosphatase, time to increase in PSA; safety endpoints; and quality of life.
An initial, pre-specified, interim analysis was undertaken when 314 deaths had occurred. This demonstrated longer median overall survival among patients who received radium-223 (14.0 months) than those receiving placebo (11.2 months) with a resulting 30% decrease in the risk of death (hazard ratio 0.70, 95% 0.55 to 0.88). A subsequent, updated analysis was performed following 528 deaths. This demonstrated consistent results with longer median overall survival among patients who received radium-223 (14.9 months) than those receiving placebo (11.3 months). Similarly, the updated analysis confirmed a 30% reduction in the risk of death (hazard ratio [HR] 0.70, 95% confidence interval [CI] 0.58 to 0.83) for patients receiving radium-223. This benefit was observed across subgroups including total alkaline phosphatase level at randomization, current bisphosphonate use, previous docetaxel treatment, baseline ECOG score (0/1 vs 2), extent of disease (<6 metastases, 6-20 metastases, >20 metastases, and super scan), and opioid use.
Assessment of the secondary endpoints demonstrated a consistent benefit for radium-223. Notably, radium-223 delayed time to first symptomatic skeletal event (median, 15.6 months vs 9.8 months; HR 0.66, 95% CI 0.52 to 0.83). Unlike many systemic therapies, patients who received radium-223 were less likely to experience adverse events than those who received placebo: all adverse events (93% vs 96%), grade 3 or 4 adverse events (56% vs 62%), serious adverse events (47% vs 60%), and treatment-discontinuation as a result of adverse events (16% vs 21%). Finally, patients who received radium-223 were significantly more likely to have an improvement in the quality of life compared to patients receiving a placebo (p=0.02).
The authors subsequently published a pre-planned analysis with stratification according to receipt of prior docetaxel.10 Radium-223 prolonged survival both in patients who had previously received docetaxel (HR 0.70, 95% CI 0.56 to 0.88) and those who had not previously received docetaxel (HR 0.69 (95% CI 0.52 to 0.92).
As both radium-223 and abiraterone acetate11,12 have demonstrated survival benefits in patients with metastatic castrate-resistant prostate cancer, there was interest in combining these two agents. The ERA 223 trial randomized 806 patients with chemotherapy-naïve, metastatic castrate-resistant prostate cancer with bone metastasis to radium-223 or placebo, in addition to abiraterone acetate. Symptomatic skeletal event-free survival was the primary outcome. Somewhat unexpectedly, the trial was unblinded prematurely as more fractures and deaths were identified in the radium-223 arm than among patients receiving placebo. Median skeletal event-free survival was 22.3 months (interquartile range 17.0 to 25.8 months) among patients receiving radium-223 and abiraterone acetate and 26.0 months (interquartile range 21.8 months to 28.3 months) in patients receiving placebo and abiraterone acetate (HR 1.12, 95% CI 0.92 to 1.37). Fractures were more common among patients receiving radium-223 and abiraterone acetate (29%) than those receiving placebo and abiraterone acetate (11%). Thus, the combination of radium-223 and abiraterone acetate is not recommended in combination, however other combinations of agents with radium-223 are currently being tested (ie. enzalutamide).
Role of Radiopharmaceuticals in the AUA Guideline
The American Urological Association Guideline on Castrate-Resistant Prostate Cancer (amended in 2018) defines a number of clinical scenarios in which radiopharmaceuticals may be considered.13
First, among patients with good performance status and have not yet received docetaxel but who are symptomatic (based on a definition requiring regular use of narcotic analgesics for pain that is attributable to documented metastasis), radium-223 may be offered to patients who have symptoms attributable to bony metastatic disease in the absence of visceral disease in addition to standard of care options including abiraterone acetate plus prednisone, enzalutamide, and docetaxel. Patients with symptomatic metastases who decline these standard therapies, alternative treatments including radionuclide therapy (such as strontium-89) may be offered.13
Second, for symptomatic patients with poor performance status who have not previously received docetaxel, there is a relative paucity of direct evidence to inform treatment choices as most patients with poor performance status are excluded from clinical trials. Based on extrapolation from studies in patients with better performance status, the guideline recommends considering aggressive prostate cancer treatment where the functional impairments resulting in poor performance status are directly attributable to prostate cancer. In cases where the poor performance status is related to bony metastatic disease, radium-223 is a recommended option.13
Third, among patients with metastatic castrate-resistant prostate cancer who have previously received docetaxel-based chemotherapy, radium-223 is one of four agents with a proven survival benefit, along with abiraterone acetate plus prednisone, enzalutamide, and cabazitaxel.
Fourth, and finally, in patients with advanced mCRPC who are symptomatic and have poor performance status following previous docetaxel chemotherapy, symptom management is strongly advocated in keeping with the American Society for Clinical Oncology’s guidance regarding the treatment of patients with advanced solid tumors. However, judicious use of radionuclide therapy, along with abiraterone acetate plus prednisone, enzalutamide, ketoconazole plus steroids, are offered within the AUA guidelines13 despite the lack of strong data to support the use of these agents in this patient population.
The Canadian Urologic Association Guidelines similarly recommend radium-223 in patients with metastatic castrate-resistant prostate cancer who have bone pain related to their metastases and no visceral disease.14
New directions
The ALSYMPCA trial was the first to demonstrate that radiopharmaceuticals could improve overall survival, in addition to skeletal-related events,4 in patients with metastatic castrate-resistant prostate cancer. On the basis of this observation, there is an ongoing effort to identify molecular targets for linkage to radiopharmaceuticals. Proposed targets have included prostate-specific membrane antigen (PSMA) and gastrin-releasing peptide receptors (GRPr),15 These have the advantage of targeting prostate cancer cells, rather than being inherently bone targeting as is the case for current radiopharmaceuticals. Thus far, preliminary data based on prostate-specific membrane antigen targeted beta-emitters such as lutetium-177 suggest a promise to this approach but further work remains prior to the adoption of this approach.1 Further, ongoing research assessing prostate-specific membrane antigen targeted alpha-emitters is ongoing.
Written by: Zachary Klaassen, MD, MSc, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Atlanta, Georgia
Published Date: December 2019
- Written by: Christopher J.D. Wallis, MD, PhD and Zachary Klaassen, MD, MSc
- References:
1. Sartor, Oliver. "Isotope therapy for castrate-resistant prostate cancer: unique sequencing and combinations." The Cancer Journal 22, no. 5 (2016): 342-346.
2. Ye, Xiaojuan, Da Sun, and Cen Lou. "Comparison of the efficacy of strontium-89 chloride in treating bone metastasis of lung, breast, and prostate cancers." Journal of cancer research and therapeutics 14, no. 8 (2018): 36.
3. James, Nicholas, Sarah Pirrie, Ann Pope, Darren Barton, Lazaros Andronis, Ilias Goranitis, Stuart Collins et al. "TRAPEZE: a randomised controlled trial of the clinical effectiveness and cost-effectiveness of chemotherapy with zoledronic acid, strontium-89, or both, in men with bony metastatic castration-refractory prostate cancer." Health Technology Assessment 20 (2016).
4. Parker, Christopher, S. Nilsson, Daniel Heinrich, Svein I. Helle, J. M. O'sullivan, Sophie D. Fosså, Aleš Chodacki et al. "Alpha emitter radium-223 and survival in metastatic prostate cancer." New England Journal of Medicine 369, no. 3 (2013): 213-223.
5. Fanti, Stefano, Silvia Minozzi, Gerald Antoch, Ian Banks, Alberto Briganti, Ignasi Carrio, Arturo Chiti et al. "Consensus on molecular imaging and theranostics in prostate cancer." The Lancet Oncology 19, no. 12 (2018): e696-e708.
6. Henriksen, Gjermund, Knut Breistøl, Øyvind S. Bruland, Øystein Fodstad, and Roy H. Larsen. "Significant antitumor effect from bone-seeking, α-particle-emitting 223Ra demonstrated in an experimental skeletal metastases model." Cancer research 62, no. 11 (2002): 3120-3125.
7. Bruland, Øyvind S., Sten Nilsson, Darrell R. Fisher, and Roy H. Larsen. "High-linear energy transfer irradiation targeted to skeletal metastases by the α-emitter 223Ra: adjuvant or alternative to conventional modalities?." Clinical cancer research 12, no. 20 (2006): 6250s-6257s.
8. Nilsson, Sten, Roy H. Larsen, Sophie D. Fosså, Lise Balteskard, Kari W. Borch, Jan-Erik Westlin, Gro Salberg, and Øyvind S. Bruland. "First clinical experience with α-emitting radium-223 in the treatment of skeletal metastases." Clinical cancer research 11, no. 12 (2005): 4451-4459.
9. Nilsson, Sten, Lars Franzén, Christopher Parker, Christopher Tyrrell, René Blom, Jan Tennvall, Bo Lennernäs et al. "Bone-targeted radium-223 in symptomatic, hormone-refractory prostate cancer: a randomised, multicentre, placebo-controlled phase II study." The lancet oncology 8, no. 7 (2007): 587-594.
10. Hoskin, Peter, Oliver Sartor, Joe M. O'Sullivan, Dag Clement Johannessen, Svein I. Helle, John Logue, David Bottomley et al. "Efficacy and safety of radium-223 dichloride in patients with castration-resistant prostate cancer and symptomatic bone metastases, with or without previous docetaxel use: a prespecified subgroup analysis from the randomised, double-blind, phase 3 ALSYMPCA trial." The Lancet Oncology 15, no. 12 (2014): 1397-1406.
11. Ryan, Charles J., Matthew R. Smith, Johann S. De Bono, Arturo Molina, Christopher J. Logothetis, Paul De Souza, Karim Fizazi et al. "Abiraterone in metastatic prostate cancer without previous chemotherapy." New England Journal of Medicine 368, no. 2 (2013): 138-148.
12. De Bono, Johann S., Christopher J. Logothetis, Arturo Molina, Karim Fizazi, Scott North, Luis Chu, Kim N. Chi et al. "Abiraterone and increased survival in metastatic prostate cancer." New England Journal of Medicine 364, no. 21 (2011): 1995-2005.
13. Lowrance, William T., Mohammad Hassan Murad, William K. Oh, David F. Jarrard, Matthew J. Resnick, and Michael S. Cookson. "Castration-resistant prostate cancer: AUA Guideline Amendment 2018." The Journal of urology 200, no. 6 (2018): 1264-1272.
14. Saad, Fred, Kim N. Chi, Antonio Finelli, Sebastien J. Hotte, Jonathan Izawa, Anil Kapoor, Wassim Kassouf et al. "The 2015 CUA-CUOG Guidelines for the management of castration-resistant prostate cancer (CRPC)." Canadian Urological Association Journal 9, no. 3-4 (2015): 90.
15. Maffioli, L., L. Florimonte, D. Costa, C. Correia, C. Grana, M. Luster, L. Bodei, and M. Chinol. "New radiopharmaceutical agents for the treatment of castration-resistant prostate cancer." Quart J Nuclear Med Molec Imaging 59 (2015): 420-438.
Evidence-Based Therapeutic Approaches for mCRPC
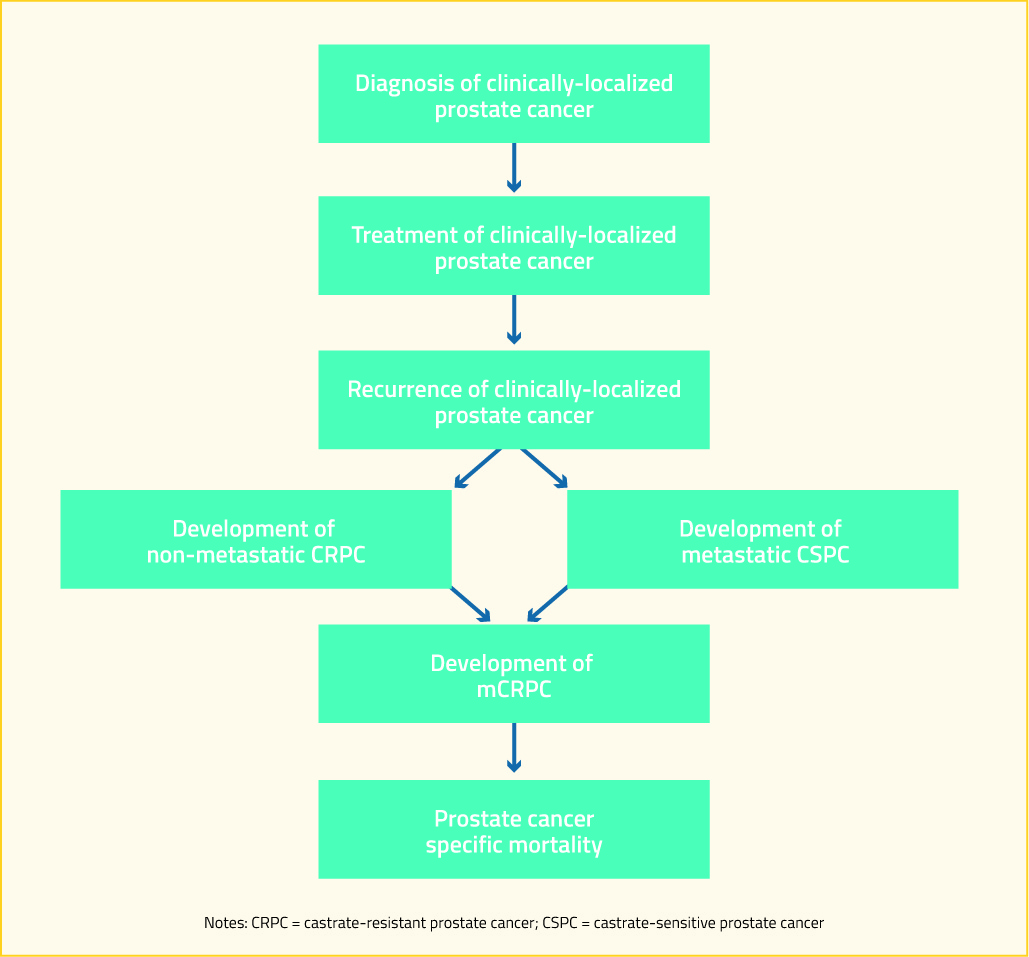
There is a large spectrum of prostate cancer progression. For patients who are initially diagnosed with a clinically-localized disease, such a pathway is highlighted in the following diagram. For patients who present with de novo metastatic disease, they join this algorithm at “development of metastatic hormone-sensitive prostate cancer (mHSPC)”.
Advanced androgen axis targeting agents (such as abiraterone and enzalutamide) and chemotherapeutics (such as docetaxel) are increasingly used earlier in the disease process, including in de novo metastatic castrate-sensitive prostate cancer and in non-metastatic castrate resistant prostate. While there is some evidence that re-challenge with docetaxel may provide benefit in patients who previously demonstrate docetaxel response, 2, 3 the use of advanced androgen axis targeting agents and docetaxel earlier in the disease trajectory may preclude their use at the development of mCRPC. Acknowledging the changes this utilization has on the treatment of mCRPC, this article will focus on guideline-recommended treatment options.
As the androgen axis continues to be important in patients who have developed castration resistance, ongoing continuous treatment with androgen-deprivation therapy is recommended.4 Historically, a number of secondary hormonal maneuver have been employed. However, routine use of these preceded the availability of therapies with proven survival benefits. As no secondary hormonal maneuver has been shown to prolong survival, they are not widely recommended. However, there is evidence that, for patients who are currently receiving LHRH agonist or antagonist monotherapy, the addition of androgen receptor antagonists and resulting total androgen blockade is associated with short-term PSA-responses. Conversely, for patients who are currently receiving total androgen blockage, anti-androgen withdrawal is recommended as some patients may experience an antiandrogen withdrawal response.
For patients who are asymptomatic or minimally-symptomatic, have good performance status, and have not yet received docetaxel chemotherapy, there are numerous treatment options. These include docetaxel, abiraterone plus prednisone, enzalutamide, and sipuleucel-T5. Docetaxel was the first agent shown to have a survival benefit in patients with mCRPC in 20046 and it quickly became standard of care for these patients as there were no alternatives with a demonstrated survival benefit. In 2012, COU-AA-302 was the first study to demonstrate a survival benefit for a non-cytotoxic agent in the treatment of mCRPC: patients treated with abiraterone plus prednisone demonstrated approximated 4 months longer overall survival (OS) than those receiving prednisone alone.7 Subsequently, in 2014, the PREVAIL study demonstrated similar benefits for enzalutamide in this patient population.8 Both abiraterone and enzalutamide target the androgen axis. In contrast, sipuleucel-T is an autologous active cellular immunotherapy. Published in 2010, the IMPACT study demonstrated that this approach was associated with approximately 20% improved overall survival.9 For patients who opt against these standard treatments, observation alone, first-generation anti-androgens, or ketoconazole accompanied by steroids may be offered.5 While not included in these guidelines, the FIRSTANA trial compared docetaxel and two doses of cabazitaxel in chemotherapy naïve patients with mCRPC. Overall, no large differences between the regimes were seen with respect to oncologic efficacy or tolerability.10
For patients who have good performance status and have not yet received docetaxel but who are symptomatic (again, based on a definition requiring regular use of narcotic analgesics for the pain that is attributable to documented metastasis), there are again a number of treatment options. Abiraterone plus prednisone, enzalutamide, and docetaxel form the standard of care for these patients. In addition, the alpha-emitter radium-223 may be offered to patients who have symptoms attributable to bony metastatic disease in the absence of visceral disease on the basis of the results of the ALSYMPCA trial. This phase 3 trial demonstrated that treatment with radium-223 significantly improved overall survival as well as skeletal-related events.11 As with asymptomatic or minimally-symptomatic patients who have good performance status and are chemotherapy-naïve, symptomatic patients who decline standard treatments may be offered alternative therapies though these do not have proven survival benefit. In this patient population, these treatments include ketoconazole with steroids, mitoxantrone, or radionuclide therapy.5
For symptomatic patients with poor performance status who have not previously received docetaxel, there is a relative paucity of direct evidence to inform treatment choices as most patients with poor performance status are excluded from clinical trials. However, guidelines typically extrapolate from studies in patients with better performance status to guide therapy in these patients.5 Aggressive prostate cancer treatment may especially be warranted where the functional impairments resulting in poor performance status are directly attributable to prostate cancer. In contrast, patients with poor performance status as a result of other medical conditions have less to gain from aggressive prostate cancer therapy. Considering these factors, individual, tailored therapy is warranted with a thorough discussion of potential risks and benefits of therapy. The AUA guidelines currently recommend either abiraterone plus prednisone or enzalutamide for these patients.5 For patients with poor performance status that is attributable to their disease burden, docetaxel or mitoxantrone may be offered whereas, when the poor performance status is related to bony metastatic disease, radium-223 is a recommended option. For patients unable or unwilling to receive standard therapies, ketoconazole with steroids or radionuclide therapy remain options though these have not demonstrated survival benefit5. In contrast, the CUA guidelines do not stratify by performance status and recommend docetaxel with abiraterone plus prednisone or enzalutamide as alternatives for patients who cannot receive or refuse docetaxel and radium-223 as an alternative for patients who have bony pain related to their metastases and no visceral disease.4
Among patients with mCRPC who have previously received docetaxel-based chemotherapy, treatment options may again be stratified by performance status. There are 4 agents with a proven survival benefit in this population: abiraterone plus prednisone; enzalutamide; cabazitaxel; and radium-223. Given that this is a relatively advanced disease state and these treatments remain non-curative and yet have a significant potential burden of toxicity, care should be taken to provide prostate cancer treatments which preserve these patients’ excellent quality of life. It is also at this time that sequencing of agents becomes particularly relevant as many patients will have received an advanced androgen axis targeting agent (abiraterone or enzalutamide) prior to receiving docetaxel and will now be on their third line of mCRPC treatment.
In 2011, the COU-AA-301 trial demonstrated that abiraterone plus prednisone could improve overall survival approximately 4 months for patients with advanced mCRPC following docetaxel chemotherapy.12 Subsequently, in 2012, the AFFIRM trial demonstrated similar results for enzalutamide in this patient population.13 TROPIC tested cabazitaxel versus mitoxantrone, each with prednisone, in patients who had progressed following docetaxel for mCRPC and demonstrated an improvement of approximately 2.5 months overall survival for patients receiving cabazitaxel.14 As discussed previously among patients who had not yet received docetaxel, ALSYMPCA demonstrated an improvement in both survival and skeletal-related events for patients receiving radium-223.11 In addition to these agents, docetaxel re-challenge is suggested for patients who discontinued therapy due to reversible toxicity. The AUA guidelines again offer ketoconazole plus steroids for patients who are unable or unwilling to take other agents.
In patients with advanced mCRPC who are symptomatic and have poor performance status following previous docetaxel chemotherapy, symptom management is strongly advocated in keeping with the American Society for Clinical Oncology’s guidance regarding the treatment of patients with advanced solid tumors. Aggressive treatment at this time may lead to unnecessary cost and toxicity, may delay access to the end of life care, and is unlikely to provide meaningful benefit. Therefore, palliative care is prioritized. Abiraterone plus prednisone, enzalutamide, ketoconazole plus steroid or radionuclide therapy are offered within the AUA guidelines5 but there is no strong data to support the use of these agents in this patient population.
Apart from specific mCRPC medication, bone health remains important in all patients with advanced prostate cancer due to a confluence of risk factors: age-related declines in bone mineral density, the deleterious effects of androgen-deprivation therapy on bones15 (even among patients with localized prostate cancer16), and the involvement of bony metastatic disease. Therefore, calcium and vitamin D are recommended for all patients with mCRPC. In addition, a bone-targeting agent, either denosumab or zoledronic acid, is recommended. These agents have been shown to decrease disease-related skeletal events though, unlike radium-223, they have not been found to improve survival. The timing of initiation of bone-targeted agents is somewhat unclear as there is evidence that the risk of significant toxicity (particularly, osteonecrosis of the jaw) increases substantially after 2 years of therapy17 and may patients with mCRPC will be expected to live longer than this.
Additionally, the symptomatic benefit of palliative radiotherapy should not be underestimated, and this should be offered where it is deemed clinically appropriate.
Special considerations should be undertaken for some patients as these may guide treatment choices. In heavily pre-treated patients with mCRPC, Mateo et al. found that mutations or deletions in DNA-repair genes could be found in 33% of patients.18 These patients demonstrated a notably strong response to treatment with the PARP inhibitor olaparib. A biomarker suite including BRCA 1 and 2, ATM, Fanconi’s anemia genes, and CHECK2 had a specificity of 94% for identifying treatment response. Thus, identification of these defects in DNA-repair may guide treatment choice. More recently, a phase 2 trial demonstrated that olaparib added to abiraterone plus prednisone improved overall survival compared to abiraterone plus prednisone alone in a population of patients who had previously received docetaxel but were not enriched for DNA-repair defects.19
Recently, the phase 3 trial of PROSTVAC, viral vector-based immunotherapy, in chemotherapy naïve patients with asymptomatic or minimally symptomatic mCRPC were reported. Despite promising results in a phase 2 trial where median OS was improved by 8.5 months, this phase 3 trial was unfortunately negative with a non-significant median difference in overall survival of approximately 1 month.20
Despite the survival benefits of many agents in metastatic castrate-resistant prostate cancer, these treatments remain non-curative. Therefore, consideration for enrollment in ongoing clinical trials should be considered for all eligible patients.
Published Date: April 16th, 2019
- Written by: Zachary Klaassen, MD, MSc
- References:
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018; 68(1):7-30.
- Thomas C, Brandt MP, Baldauf S, et al. Docetaxel-rechallenge in castration-resistant prostate cancer: defining clinical factors for successful treatment response and improvement in overall survival. Int Urol Nephrol 2018; 50(10):1821-1827.
- Oudard S, Kramer G, Caffo O, et al. Docetaxel rechallenge after an initial good response in patients with metastatic castration-resistant prostate cancer. BJU Int 2015; 115(5):744-52.
- Saad F, Chi KN, Finelli A, et al. The 2015 CUA-CUOG Guidelines for the management of castration-resistant prostate cancer (CRPC). Can Urol Assoc J 2015; 9(3-4):90-6.
- Lowrance WT, Murad MH, Oh WK, et al. Castration-Resistant Prostate Cancer: AUA Guideline Amendment 2018. J Urol 2018; 200(6):1264-1272.
- Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med 2004; 351(15):1502-12.
- Ryan CJ, Smith MR, de Bono JS, et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med 2013; 368(2):138-48.
- Beer TM, Armstrong AJ, Rathkopf DE, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med 2014; 371(5):424-33.
- Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med 2010; 363(5):411-22.
- Oudard S, Fizazi K, Sengelov L, et al. Cabazitaxel Versus Docetaxel As First-Line Therapy for Patients With Metastatic Castration-Resistant Prostate Cancer: A Randomized Phase III Trial-FIRSTANA. J Clin Oncol 2017:JCO2016721068.
- Parker C, Nilsson S, Heinrich D, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med 2013; 369(3):213-23.
- de Bono JS, Logothetis CJ, Molina A, et al. Abiraterone and increased survival in metastatic prostate cancer. N Engl J Med 2011; 364(21):1995-2005.
- Scher HI, Fizazi K, Saad F, et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med 2012; 367(13):1187-97.
- de Bono JS, Oudard S, Ozguroglu M, et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: a randomised open-label trial. Lancet 2010; 376(9747):1147-54.
- Shahinian VB, Kuo YF, Freeman JL, et al. Risk of fracture after androgen deprivation for prostate cancer. N Engl J Med 2005; 352(2):154-64.
- Wallis CJ, Mahar AL, Satkunasivam R, et al. Cardiovascular and Skeletal-Related Events Following Localised Prostate Cancer Treatment: Role of Surgery, Radiotherapy and Androgen-Deprivation. Urology 2016; 97:145-152.
- Barasch A, Cunha-Cruz J, Curro FA, et al. Risk factors for osteonecrosis of the jaws: a case-control study from the CONDOR dental PBRN. J Dent Res 2011; 90(4):439-44.
- Mateo J, Carreira S, Sandhu S, et al. DNA-Repair Defects and Olaparib in Metastatic Prostate Cancer. N Engl J Med 2015; 373(18):1697-708.
- Clarke N, Wiechno P, Alekseev B, et al. Olaparib combined with abiraterone in patients with metastatic castration-resistant prostate cancer: a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol 2018; 19(7):975-986.
- Gulley JL, Borre M, Vogelzang NJ, et al. Phase III Trial of PROSTVAC in Asymptomatic or Minimally Symptomatic Metastatic Castration-Resistant Prostate Cancer. J Clin Oncol 2019:JCO1802031.