Post-Operative Radiotherapy in Prostate Cancer – The State of the Data
- Details
- Published in Everyday Urology - Oncology Insights: Volume 5, Issue 4
Contemporary treatment options for patients with clinically localized prostate cancer include radical prostatectomy, radiotherapy, and active surveillance. Surgery can be curative for approximately two-thirds of patients choosing radical prostatectomy.1 However, men with adverse pathologic findings at the time of radical prostatectomy, such as the presence of positive surgical margins, extraprostatic extension, or seminal vesicle invasion,2,3 experience up to a 60% risk of recurrence at 10 years and may require subsequent radiation therapy.2

The Evolving Landscape of First-Line Therapy for Metastatic Clear Cell Renal Cell Carcinoma
- Details
- Published in Everyday Urology - Oncology Insights: Volume 5, Issue 4
When examined at a national level in the United States, cancers of the kidney and renal pelvis (despite different histology) are considered in aggregate and represent the sixth most common newly diagnosed tumors in men and eighth most common in women in the United States in 2020,1 representing an estimated 73,750 new diagnoses and 14,830 deaths. The vast majority of these cancers will be renal parenchymal tumors with renal cell carcinoma (RCC) comprising the preponderance of these lesions.
Update on Low-Grade Upper Tract Urothelial Carcinoma
- Details
- Published in Everyday Urology - Oncology Insights: Volume 5, Issue 3
Published Date: October 2020
Upper tract urothelial carcinomas (UTUCs) are a heterogeneous group of malignancies arising from the urothelium at the level of the renal pelvis or ureter. They comprise 5% to 10% of all urothelial carcinomas and are diagnosed in approximately two per 100,000 persons in the United States annually, the majority of whom are adults older than 70 years.1-3 A significant percentage of UTUCs are low-grade; these primarily papillary tumors are substantially less aggressive than high-grade UTUCs and demonstrate a low rate of cancer-specific mortality, but hematuria and urinary obstruction are common and require management.4-6
Non-muscle Invasive Bladder Cancer: Overcoming Diagnostic and Therapeutic Challenges
- Details
- Published in Everyday Urology - Oncology Insights: Volume 5, Issue 3
In 2020, approximately 81,000 cases of urothelial carcinoma of the bladder will be diagnosed in the United States, with nearly 18,000 associated deaths.1 Bladder cancer disproportionally affects men and is associated with well-defined environmental risk factors—tobacco use underlies approximately 50% of cases.2 Nonmuscle-invasive bladder cancer (NMIBC) is primarily managed by transurethral resection, risk-stratified use of intravesical chemotherapeutic or immunotherapeutic agents, and close surveillance.

What is Changing in Advanced Prostate Cancer?
- Details
- Published in Everyday Urology - Oncology Insights: Volume 5, Issue 2
Introduction
Prostate cancer, while commonly diagnosed in early forms, remains the second leading cause of cancer mortality in the United States and Europe.1 For patients who die of prostate cancer, some will be initially diagnosed and treated for metastatic castration-sensitive disease (mCSPC) while others will progress through non-metastatic castration-resistant disease (nmCPRC) following initial local therapy followed by androgen deprivation therapy (ADT) for biochemical recurrence. In either case, nearly all men who die of prostate cancer will have metastatic castration-resistant disease (mCRPC) prior to death.
ARAMIS: Favorable Overall Survival and Safety Findings for Darolutamide in Nonmetastatic Castration-Resistant Prostate Cancer
- Details
- Published in Everyday Urology - Oncology Insights: Volume 5, Issue 2
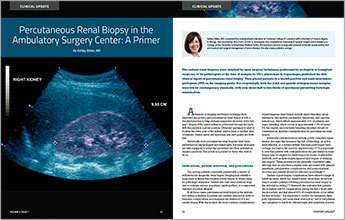
Percutaneous Renal Biopsy in the Ambulatory Surgery Center: A Primer
- Details
- Published in Everyday Urology - Oncology Insights: Volume 5, Issue 1
The earliest renal biopsies were obtained by open surgical techniques performed by urologists or transplant surgeons, or by pathologists at the time of autopsy. In 1951, physicians in Copenhagen published the first clinical report of percutaneous renal biopsy.1 They placed patients in a seated position and used intravenous pyelogram (IVP) as the imaging guide. Not surprisingly, both the yield and quality of biopsy tissue samples were low by contemporary standards, with only about half to two-thirds of specimens permitting histologic examination.
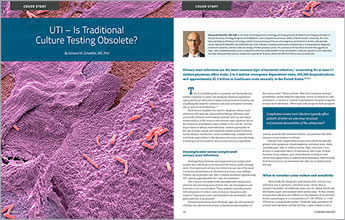
UTI – Is Traditional Culture Testing Obsolete?
- Details
- Published in Everyday Urology - Oncology Insights: Volume 5, Issue 1
Urinary tract infections are the most common type of bacterial infection,1 accounting for at least 11 million physician office visits, 2 to 3 million emergency department visits, 400,000 hospitalizations, and approximately $2.3 billion in healthcare costs annually in the United States.2,3,4,5
Choosing First-Line Treatment for Metastatic Castration-Resistant Prostate Cancer: APCCC Highlights
- Details
- Published in Everyday Urology - Oncology Insights: Volume 4, Issue 4
Published Date: December 2019
The choice of initial treatment for newly diagnosed metastatic castration-resistant prostate cancer (mCRPC) is far more complex than it was even a decade ago. Today, many patients with mCRPC have already received intensive upfront therapies during the hormone-sensitive stage— a “leftward” shift in treatment (based on the clinical states model we so frequently employ) which can spur a “rightward” shift in disease biology due to the earlier emergence of treatment-resistant clones.
Choosing First-Line Systemic Therapy for Newly Diagnosed Metastatic Hormone Sensitive Prostate Cancer
- Details
- Published in Everyday Urology - Oncology Insights: Volume 4, Issue 4
Published Date: December 2019
Metastatic hormone-sensitive prostate cancer (mHSPC) has become increasingly prevalent in the United States. Between 2009 and 2020, experts have projected a nearly 17% increase in the number of newly diagnosed mHSPC cases and a more than 18% increase in cases of mHSPC occurring after failure of local (curative-intent) treatment.1 This increase is likely multifactorial, reflecting changes in prostate-specific antigen (PSA) screening practices, the increased use of more sensitive imaging modalities, and other factors.2, 3

Controversies with PSMA-Based Imaging and Targeted Therapy
- Details
- Published in Everyday Urology - Oncology Insights: Volume 4, Issue 4
Published Date: December 2019
Prostate-specific membrane antigen (PSMA) is expressed 100 to 1,000 times more highly in prostatic adenocarcinoma than in benign prostate tissue, particularly in the setting of androgen deprivation.1 Around the world, we are seeing the rapid adoption of PSMA PET-CT/MRI, which is able to detect metastatic disease that is inapparent on conventional imaging (CT and bone scintigraphy).

A Review of Comprehensive Bone Health Management Strategies for Men with Prostate Cancer
- Details
- Published in Everyday Urology - Oncology Insights: Volume 4, Issue 4
Bone health is a critical area of unmet need among men with advanced prostate cancer. Age increases the risk for fragility fractures among both men and women, and older men with fragility fractures are at higher risk of subsequent death than are women.1-3 Systemic anti-androgen therapies for prostate cancer, while life-prolonging, accelerate bone loss by tipping the balance of bone homeostasis toward bone resorption, which further increases patients’ risk of fragility fractures.4

Monitoring and Managing Toxicities in Patients with Metastatic Hormone-Sensitive Prostate Cancer
- Details
- Published in Everyday Urology - Oncology Insights: Volume 4, Issue 4
A 65-year-old man presents with skeletal pain. His PSA is 101 ng per mL, computed tomography (CT) reveals pelvic lymphadenopathy, a 99mTc bone scan shows extensive bone metastases, and prostate biopsy cores are interpreted as Gleason score 9 with intraductal features. The patient starts long-term androgen-deprivation therapy (ADT) and completes five cycles of docetaxel. His pain resolves. His PSA declines but remains persistently elevated at 2.6 ng per mL, so the decision is made to add enzalutamide, a next-generation androgen receptor (AR)-targeted therapy, to ADT.
Genetic Evaluation of Hereditary Prostate Cancer
- Details
- Published in Everyday Urology - Oncology Insights: Volume 4, Issue 2
During much of the past 30 years, genetic tests for heritable disorders have assessed limited numbers of genes and have often employed serial testing algorithms in which the next test was determined by the results of the prior test.¹ The advent of next-generation (also known as massively parallel high-throughput) sequencing has transformed this picture by making it possible to sequence the entire human genome for less than $1,000.1,2
Darolutamide: Approved For Non-Metastatic Castration-Resistant Prostate Cancer
- Details
- Published in Everyday Urology - Oncology Insights: Volume 4, Issue 3
Published Date: September 2019
Androgen deprivation therapy (ADT) is the longstanding initial treatment for advanced hormone-sensitive prostate adenocarcinoma. Nonetheless, patients who are initiated on ADT will invariably progress by developing prostate cancer cellular clonal populations, which creates a phenotype of more castration-resistant disease with more aggressive biology.1
Preparing Your Practice for the New Era of Theranostics
- Details
- Published in Everyday Urology - Oncology Insights: Volume 4, Issue 3
Published Date: September 2019
Patients whose metastatic castration-resistant prostate cancer (mCRPC) has progressed on taxane chemotherapy and second-generation anti-androgen agents have few alternatives to palliative care. However, radiolabeled prostate-specific membrane antigen (PSMA) conjugates are now in latephase studies. In this article, I discuss theranostics, the phase 3 VISION trial, and the questions we will need to consider when PSMA-targeted radioligand therapies become available for use in our advanced prostate cancer clinics.
Optimizing Bone Health in Prostate Cancer
- Details
- Published in Everyday Urology - Oncology Insights: Volume 4, Issue 2
Protecting and improving bone health is critical when managing all stages of prostate cancer. Androgen deprivation therapy (ADT) accelerates bone resorption, which compromises bone mass and integrity starting early in treatment.1 Metastatic prostate cancer is associated with a marked increase in risk of skeletal events (fracture, spinal cord compression, and bone surgery or radiotherapy) associated with both bone metastases and treatment-induced bone loss.
Optimizing TURBT and Optical Diagnostics in Bladder Cancer
- Details
- Published in Everyday Urology - Oncology Insights: Volume 4, Issue 1
The detection of recurrent tumor is a benchmark by which the success of intravesical agents is determined. Because the U.S. Food and Drug Administration (FDA) will now consider data from single-arm trials for patients with Bacillus Calmette-Guérin (BCG)-unresponsive bladder cancer, the complete response (CR) rates (i.e. absence of disease on biopsy) is a key factor that impacts the success of many registration studies.
Update on ADT in Advanced Prostate Cancer
- Details
- Published in Everyday Urology - Oncology Insights: Volume 3, Issue 4
Prostate cancer is the leading incident cancer among men, and population growth and aging have fueled a 40% rise in global case burden since 2006.1,2 Despite recent improvements in treatment, patients with locally advanced and advanced prostate cancer experience significant emotional distress, diminished quality of life, and increased risk of cancer-specific mortality.1,2,3
Practice-Changing Applications of Radiology and Nuclear Medicine in Genitourinary Malignancies
- Details
- Published in Everyday Urology - Oncology Insights: Volume 3, Issue 4
Experts at Harvard Business School first coined the term disruptive innovation to describe how small, poorly resourced companies could successfully challenge larger ones.1 More than two decades later, this concept is central in medicine, where innovations in everything from proteomics and wearables to electronic health records and health economics are upending our status quo.2,41