(UroToday.com) The 2025 Western Section AUA annual meeting featured a urothelial carcinoma session and a presentation by Dr. Mark Tyson discussing the final results from BOND-003 Cohort C, a phase 3, single-arm study of intravesical cretostimogene grenadenorepvec for high-risk BCG-unresponsive non-muscle invasive bladder cancer with CIS. A significant treatment gap exists for efficacious, well-tolerated bladder-sparing treatment options for patients with high-risk BCG-unresponsive non-muscle invasive bladder cancer, which is defined as persistent or recurrent CIS +/- Ta/T1 non-muscle invasive bladder cancer within 12 months of BCG therapy per FDA guidance.
Cretostimogene grenadenorepvec, an oncolytic immunotherapy encoding a GM-CSF transgene, selectively replicates in and lyses cancer cells with Retinoblastoma-E2F pathway alterations, leading to tumor antigen release and antitumor immune activation. BOND-003 (NCT04452591) is a phase-3 study evaluating the efficacy and safety of cretostimogene in patients with high-risk BCG-unresponsive non-muscle invasive bladder cancer. Notably, cretostimogene has received Fast Track and Breakthrough Therapy Designations for BCG-unresponsive non-muscle invasive bladder cancer.
Overall, 112 adults with confirmed high-risk BCG-unresponsive non-muscle invasive bladder cancer with CIS were enrolled, with efficacy data from 110 patients. Treatment consisted of 6 weekly doses during induction, followed by maintenance. Patients with persistent HG Ta or CIS at month 3 were eligible for repeat induction. Response assessment included cystoscopy (biopsy as indicated) and urine cytology every 3 months for the first 2 years and every 6 months starting in year 3:

The primary endpoint is complete response at any time (centrally confirmed), and key secondary outcomes include duration of response and safety.
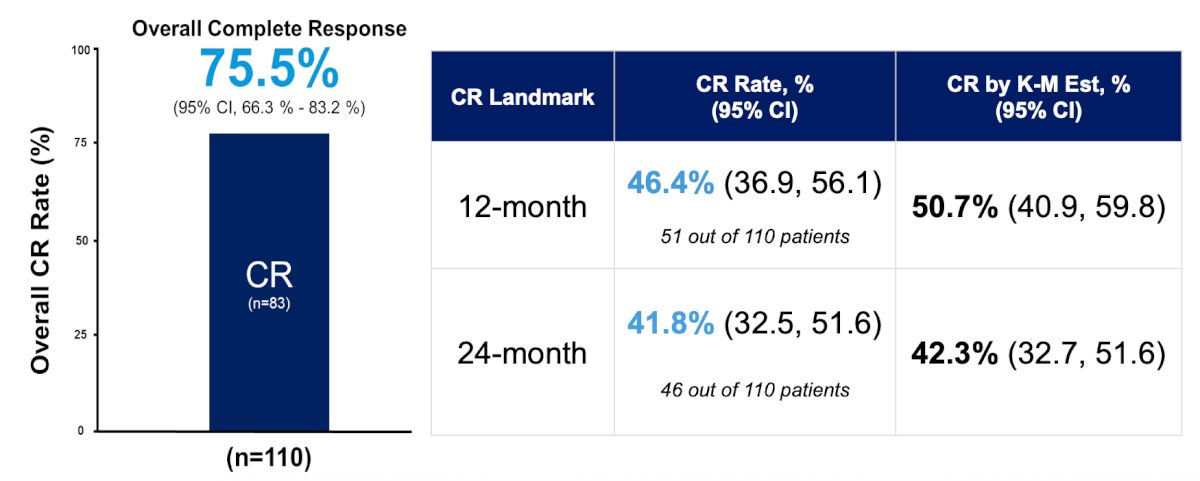
The majority of patients are male (74%), white (62%), and >65 years old (83%). As of the March 14, 2025, data cutoff, with a median follow-up time of 22.3 months, the complete response rate at any time is 75.5% (83/110) (95% CI 66.3-83.2%). Kaplan-Meier estimates of 12- and 24-month duration of response are 64.1% (95% CI 52.4-73.7%) and 58.3% (95% CI 46.3-68.5%), respectively, with an ongoing median duration of response of 27.9 months (95% CI 13.8% to not reached):

The 12-month complete response rate is 46.4% (51/110) (95% CI 36.9-56.1%). Landmark and Kaplan-Meier estimated 24-month complete response rates are 41.8% (46/110) (95% CI 32.5-51.6%) and 42.3% (95% CI 32.7-51.6), respectively. Complete responses are consistent across all patient subgroups:
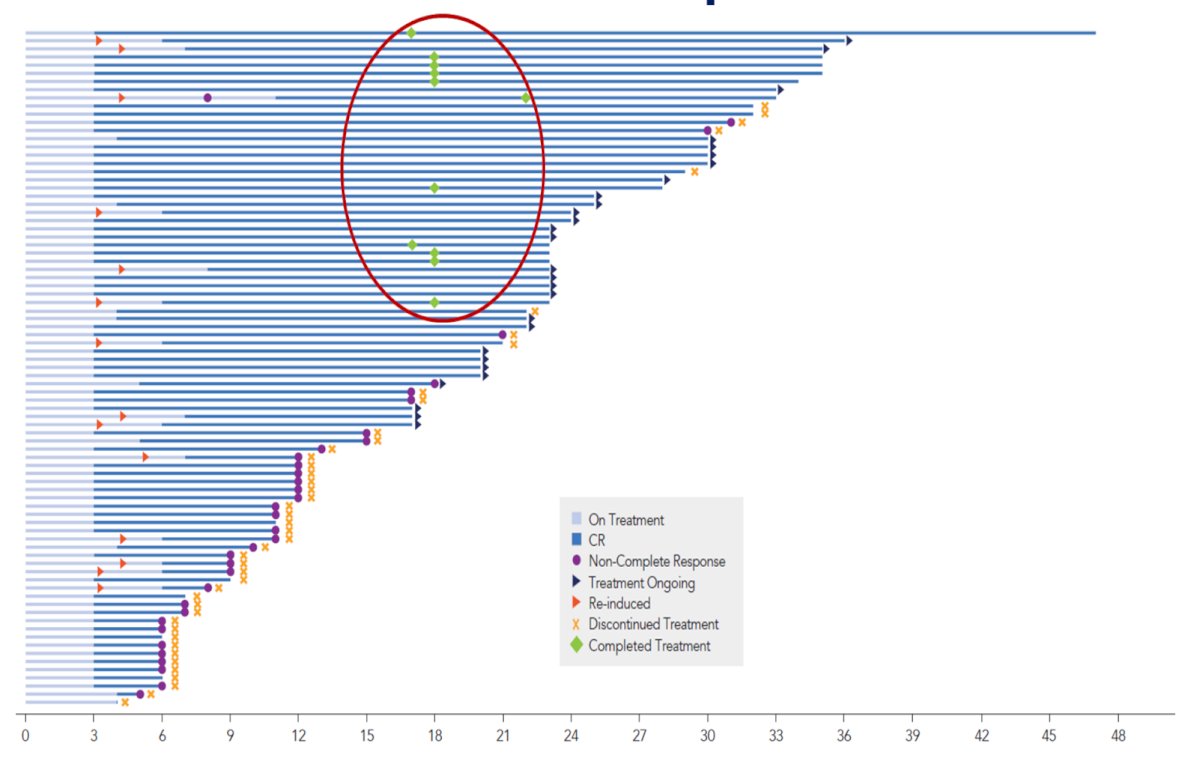
The Swimmer’s plot for individual treatment response in months is as follows:
At 24 months, 97.3% (107/110) are free from ≥T2 progression during the treatment phase, and 84.5% (93/110) have avoided radical cystectomy. There were 82.4% (14/17) of patients who underwent radical cystectomy and were T0 or non-muscle invasive bladder cancer on final pathology. Cretostimogene has a very well-tolerated safety profile, with no grade ≥3 treatment-related adverse events. Grade 1 and 2 related adverse events (ie. bladder spasm, pollakiuria, urgency) are transient, with a median resolution time of 1 day:

Dr. Tyson concluded his presentation discussing the final results from BOND-003 Cohort C with the following take-home points:
- Cretostimogene offers distinct advantages with its efficacy, durability, and safety profile for the treatment of high-risk BCG-unresponsive non-muscle invasive bladder cancer
- Ongoing and future investigations of this promising therapy may address the considerable unmet need for bladder cancer patients
Presented by: Mark Tyson II, MD, MPH, Urologic Oncologist, Mayo Clinic, Scottsdale, AZ
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Western Section American Urological Association (AUA) Annual Meeting, Napa Valley, CA, Sun, Nov 2 – Thurs, Nov 6, 2025.