(UroToday.com) Thursday’s morning plenary session brought together a distinguished panel of experts to discuss evolving strategies for percutaneous renal access in percutaneous nephrolithotomy (PCNL).
Moderated by Dr. Thomas Chi (UAB), the panel featured Dr. Vernon Pais (Dartmouth), Dr. Karen Stern (Mayo Clinic Arizona), Dr. Matt Dunn (UCLA), and Dr. Candace Granberg (Mayo Clinic Children’s Hospital). Presenters offered various unique perspectives on PCNL access with fluoroscopy, ultrasound, robotic-assisted, and pediatric malformations.

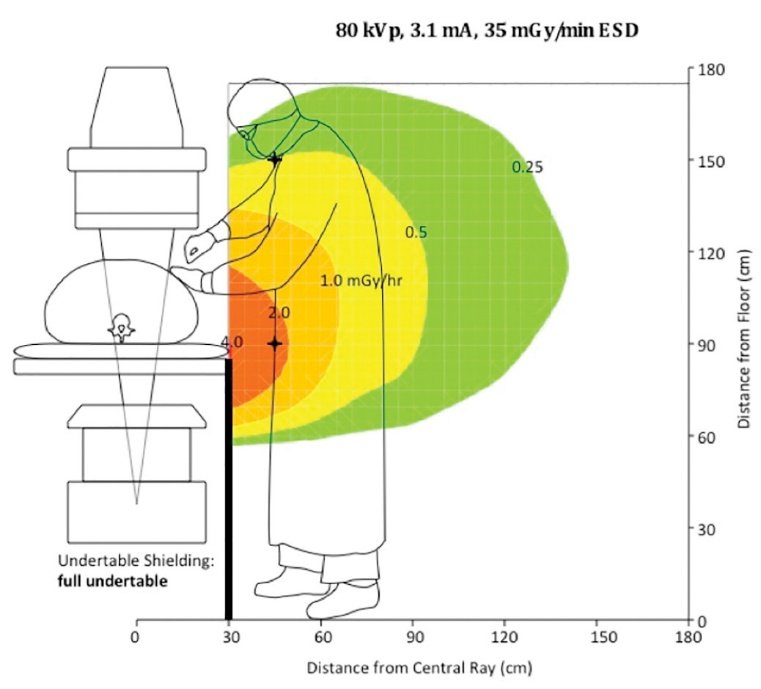
Next, Dr. Karen Stern spoke in strong support of ultrasound for PCNL access. She stressed radiation safety, referencing data showing increased breast cancer prevalence amongst female orthopedic surgeons. She noted, “Fluoroscopy means we stand over the table saying ‘go live’ again and again. With ultrasound, radiation can be brought down to nearly zero.”
She emphasized the ability of ultrasound to avoid pleural and visceral injuries, citing Monga’s series, in which 4% of upper pole cases required intervention for thoracic injury: “That should now be a never event. With ultrasound, you can clearly see the pleura, liver, spleen, and bowel before you puncture.”
Stern also highlighted ultrasound’s versatility: “Whether prone or supine, ultrasound doesn’t require relearning. It adapts to the approach, and it’s invaluable when retrograde access isn’t possible - like in urinary diversions or transplants.” She underscored its versatility in patients with infundibulopelvic stenosis, transplant kidneys, and pediatric populations.
Regarding the learning curve, Stern reassured trainees: “You can start simple, with ultrasound monitoring of fluoroscopic puncture, then progress to needle guidance, and eventually perform entirely fluoroscopy-free PCNL. The curve is not as steep as people fear.” She cited evidence of ultrasound-guided PCNL significantly reducing both total access time and total fluoroscopy time for novice and expert surgeons alike, highlighting its broad applicability.


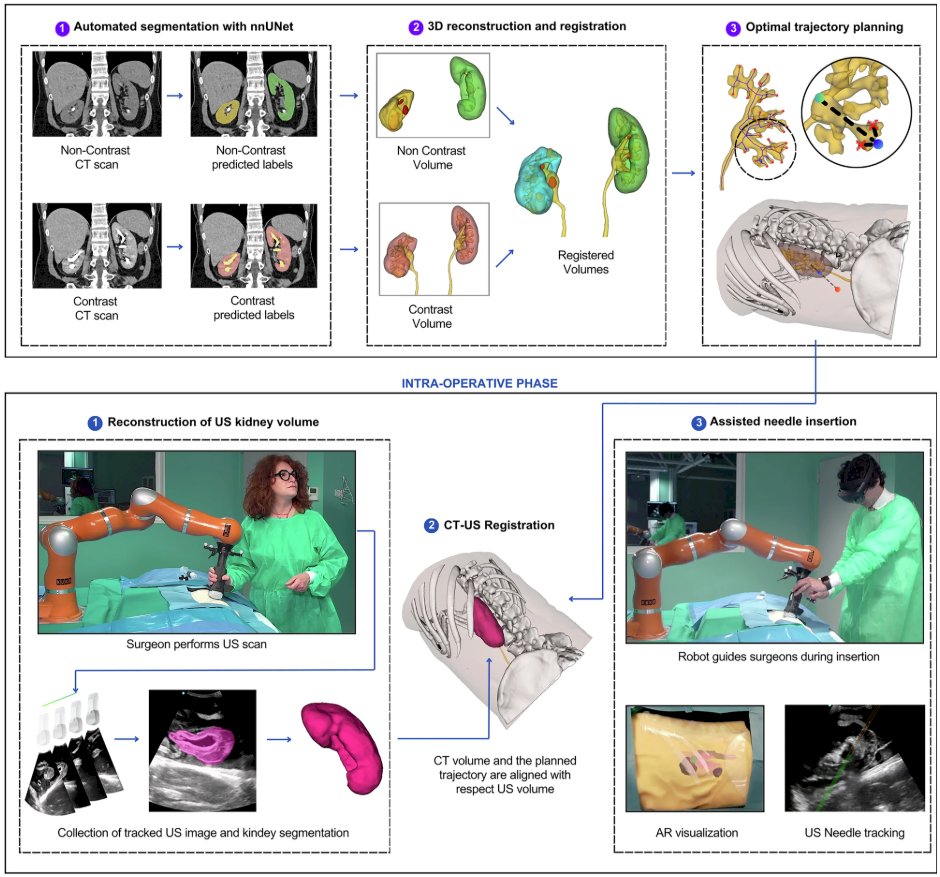
Dr. Stern concluded by presenting her experience with a newly FDA-approved robotic ultrasound-guided platform: “It’s intuitive - you tap your target on the screen, and the robotic arm tracks and aligns the needle. In our first five cases, access was achieved every time.”
Dr. Matt Dunn followed with a presentation on robotic-assisted PCNL access. “Why does it matter? Because urologist-obtained access is consistently superior to IR, but only 17% of urologists currently do their own access,” he said, citing shorter length of stay, fewer transfusions, and improved stone-free rates when urologists obtained access themselves.
Tracing history back to Johns Hopkins’ early robotic arm attempts two decades ago, Dunn noted that while early devices showed modest improvements, they failed to take hold. “Fast forward to today, and we now have clinically viable systems.”
He highlighted the Monarch™ robotic platform, which integrates ureteroscopic and percutaneous approaches with EM tracking: “It’s like a video game - you keep the ball centered on the target, and the system tells you exactly when you’re at depth.” Early clinical series demonstrated single-puncture success, low complication rates, and reduced fluoroscopy times.
Dunn also discussed EM needle guidance: “Even expert endourologists improved accuracy with EM systems. For novices, the difference was striking - 14% success with ultrasound alone versus 100% with robotic-EM assistance.” He showcased European and Japanese developments in fusion ultrasound-CT robotic arms, underscoring their potential to democratize access worldwide.
“This is no longer science fiction. Robotics will make access safer, faster, and more reproducible for both novices and experts,” he concluded.
Dr. Candace Granberg concluded the session with a discussion of PCNL access in pediatrics and complex reconstructions. “Always review prior operative notes; what reimplant was done, where the ureters drain, whether there are duplications or diversions,” she advised.
She shared cases of children with ectopic kidneys, vesicoureteral reimplantations, and duplicated systems. “Respect the ureteroureterostomy. Don’t force wires or sheaths through a tenuous anastomosis. And don’t hesitate to obtain additional imaging - MR urography or 3D reconstructions can save you in these cases.” Dr. Granberg stressed the importance of positioning: “Our spina bifida and scoliosis patients often cannot be placed in standard positions. Supine PCNL has been invaluable for these children.” For patients with neurogenic bladder, she reminded: “The most important thing is to ensure drainage during surgery. The last thing you want is a perfectly placed tract but an over-distended bladder.”She concluded with practical pearls for pediatrics: “Babies are not just small adults. Their anatomy, positioning, and physiology demand special care, especially with airway and pressure points during access.”

In closing, there is no one-access-fits-all solution. The ideal approach is to master multiple modalities to adapt to different patient anatomy, surgeon expertise, and available technology. As Dr. Chi summarized, “Access is the key to success in PCNL.”
Presented by:
Moderator: Thomas Chi, MD, MBA, University of Alabama at Birmingham
Panelists: Vernon Pais, MD, MS, Dartmouth Geisel School of Medicine, Karen Stern, MD, Mayo Clinic Arizona, Matt Dunn, MD, UCLA, Candace Granberg, MD, Mayo Clinic Children’s Hospital
Written by: Helen Gao, Medical Student at Robert Wood Johnson Medical School, Leadership and Innovation Fellowship Training (LIFT) Scholar at Department of Urology, University of California, Irvine. @helengao295 on X during the 2025 World Congress of Endourology and Uro-Technology, September 8 – September 12, 2025, Phoenix, Arizona
References:- Altschuler J, Jain R, Ganesan V, Monga M. Supracostal Upper Pole Endoscopic-Guided Prone Tubeless “Maxi-Percutaneous Nephrolithotomy”: A Contemporary Evaluation of Complications. Journal of endourology. 2019;33(4):274-278. doi:10.1089/end.2018.0502
- Ballantyne CC, Wymer KM, Sehgel NL, et al. Robotic-Assisted Electromagnetic Guidance Improves Success of Percutaneous Access for Nephrolithotomy: A Study of Novices and Experts. J Endourol. 2025;39(8):772-780. doi:10.1177/08927790251368775
- Bazzani S, Puliatti S, Ferretti S, Bianchi G, Secchi C, Ferraguti F. Ultrasonographic-guided robotic-assisted percutaneous nephrolithotomy. Communications engineering. 2025;4(1). doi:10.1038/s44172-025-00451-0
- Birowo P, Rustandi R, Risky Raharja PA, Putra HW, Rasyid N, Atmoko W. The learning curve for a single surgeon using ultrasonography to guide supine percutaneous nephrolithotomy with an alken metal telescopic dilator. Heliyon. 2022;8(12):e12524. Published 2022 Dec 21. doi:10.1016/j.heliyon.2022.e12524
- Elkoushy MA, Andonian S. Lifetime Radiation Exposure in Patients with Recurrent Nephrolithiasis. Current urology reports. 2017;18(11). doi:10.1007/s11934-017-0731-6
- Landman J, Clayman RV, Cumpanas AD, et al. Initial Clinical Experience With a Novel Robotically Assisted Platform for Combined Mini-Percutaneous Nephrolithotomy and Flexible Ureteroscopic Lithotripsy. The Journal of urology. 2024;212(3):483-493. doi:10.1097/JU.0000000000004079
- Manzo BO, Gómez F, Figueroa A, et al. A New Simplified Biplanar (0-90°) Fluoroscopic Puncture Technique for Percutaneous Nephrolithotomy. Reducing Fluoroscopy Without Ultrasound. Initial Experience and Outcomes. Urology (Ridgewood, NJ). 2020;140:165-170. doi:10.1016/j.urology.2020.03.002
- Marchini GS, Lima FS, Campos MEC, et al. Modified biplanar (0-90o) endoscopic-guided puncture technique for percutaneous nephrolithtomy: refinement with endoscopic combined intrarrenal surgery to reduce fluoroscopy and operative time. International Brazilian Journal of Urology. 2023;49(6):785-786. doi:10.1590/s1677-5538.ibju.2023.0346
- Meisinger QC, Stahl CM, Andre MP, Kinney TB, Newton IG. Radiation Protection for the Fluoroscopy Operator and Staff. American journal of roentgenology (1976). 2016;207(4):745-754. doi:10.2214/AJR.16.16556
- Metzler, Ian S., Sarah Holt, and Jonathan D. Harper. "Surgical trends in nephrolithiasis: increasing de novo renal access by urologists for percutaneous nephrolithotomy." Journal of Endourology 35.6 (2021): 769-774.
- Su, Li-Ming, Stoianovici, D., Jarrett, T.W., et al. "Robotic percutaneous access to the kidney: comparison with standard manual access." Journal of Endourology 16.7 (2002): 471-475.
- Taguchi K, Hamamoto S, Okada A, et al. A Randomized, Single-Blind Clinical Trial Comparing Robotic-Assisted Fluoroscopic-Guided with Ultrasound-Guided Renal Access for Percutaneous Nephrolithotomy. The Journal of urology. 2022;208(3):684-694. doi:10.1097/JU.0000000000002749