(UroToday.com) The sixth plenary session of the World Congress of Endourology and Uro-Technology featured a spirited point-counterpoint debate on whether intrarenal pressure truly matters in clinical practice. The moderator, Dr. Naeem Bjohani, MD of the University of Montreal, welcomed the audience and set the stage for an interactive discussion. From Denmark, Dr. Helene Jung, MD, PhD, Hospital Lillebaelt, took the position of “Yes”, while Dr. Noah Canvasser, MD, University of California, Davis, argued the counterpoint, “No”.
The topic of intrarenal pressure (IRP) in endourology has become increasingly relevant. During ureteroscopy (URS), elevated pressure can lead to intrarenal backflow, raising concerns for unfavorable clinical outcomes. With the advent of pressure-sensing ureteroscopes and suction-enabled access sheaths, it is now part of the urologist’s armamentarium to both quantify and manage IRP directly in the operating room. Despite these advances, the clinical relevance of routinely measuring IRP remains debated.
Dr. Helene Jung opened the debate by affirming that intrarenal pressure (IRP), although out of sight and out of mind to the urologist, deserves a central place in our attention. Before beginning her argument, she wanted the audience to understand why high intrarenal pressure is a problem – who does it affect and how? While the majority of ureteroscopy patients will recover without complication, she emphasized the critical 5% who progress to sepsis and, in some cases, require ICU-level care.1 “If most patients do fine, why do some end up in the ICU?” she asked, challenging the audience to look beyond averages and consider those at highest risk.
Ureteroscopy is a fine balance. Clear visualization demands irrigation, which in turn drives intrarenal pressure higher. While starting at a baseline of 10 mmHg (Figure 1), pressure rapidly increases with the addition of high-power lasers and irrigation instillation.2 “Pressure doesn’t just rise – it skyrockets to terrifying levels.”
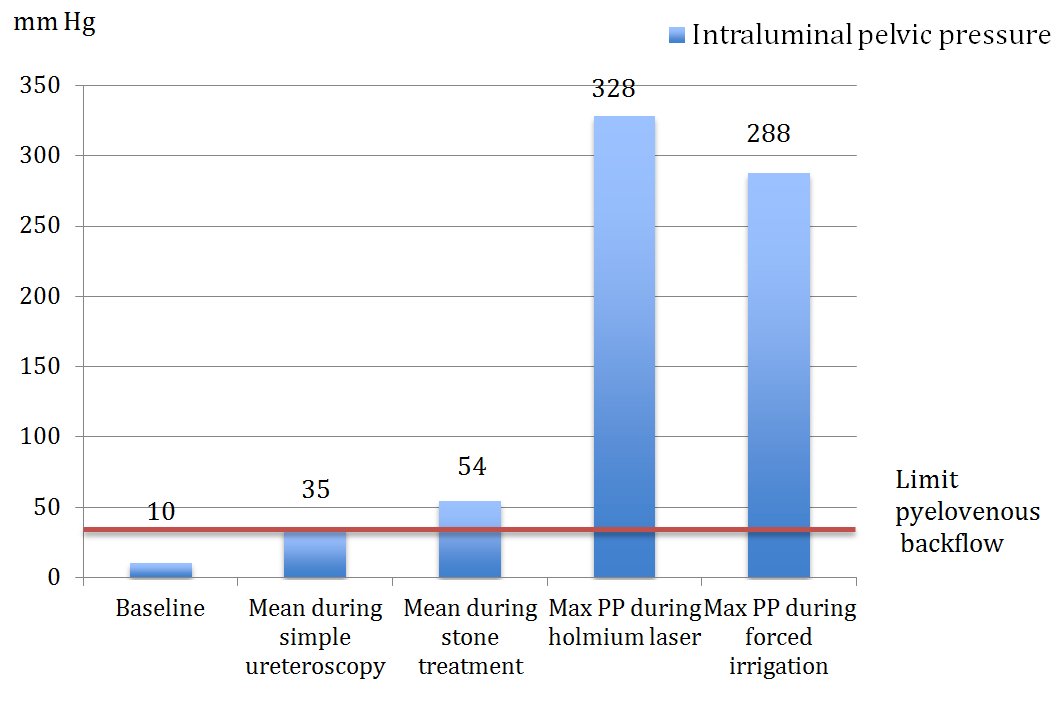
Figure 1.
This leads to intrarenal backflow, a highway for bacteria, endotoxins, and even tumor cells to enter systemic circulation. While earlier studies suggested backflow occurred at about 30 mmHg, Dr. Hung and colleagues were able to visualize backflow in live swine kidneys at 16 mmHg, illustrated in Figure 2.3
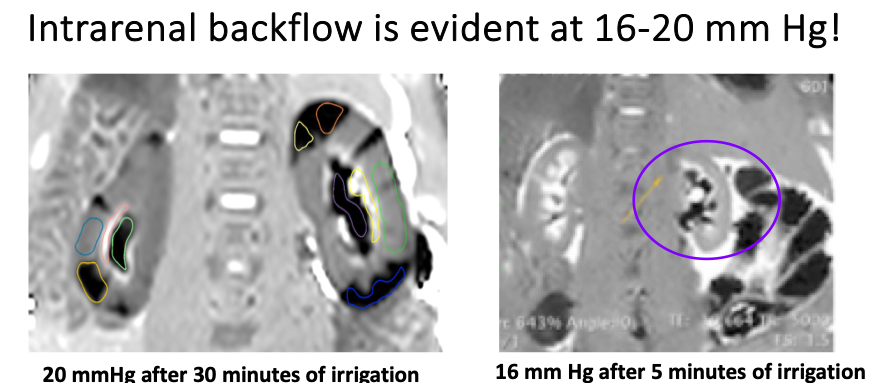 Figure 2.
Figure 2.
With the advent of modern ureteroscopes, now equipped with pressure-sensing technology and suction capability, surgeons are able to actively manage IRP in real time. Dr. Jung reflected, ‘My own experience using these tools was eye-opening; both the high-pressure peaks and the dramatic pressure drops observed with suction were striking.’ The consequences of elevated IRP extend well beyond infection. Both experimental and clinical studies have demonstrated associations with nephropathy, renal scarring, abscess formation, impaired renal function, calyceal rupture, and renal inflammation. Dr. Jung emphasized that these effects can be worse in patients with CKD, diabetes, or hypertension, especially if they undergo repeat procedures. These findings underscore that high pressure is not only a risk factor for sepsis but also a driver of long-term renal injury.
Armed with this knowledge, Dr. Jung urged the audience to reflect on the broader risks associated with ureteroscopy and how they can be mitigated. Of utmost concern are infection and sepsis. In a CROES study of 11,885 patients, 1.72% developed postoperative fever and 0.30% progressed to severe urosepsis, representing a significant number of seriously ill patients. A larger secondary study of 24,373 patients reported 3.9% with infection-related complications and 0.51% with urosepsis.4,5 These findings highlight that while the overall incidence of infectious complications is relatively low, the absolute number of affected patients worldwide is substantial. Identifying and addressing modifiable risk factors such as recent UTI, infection stones, or prolonged operative time becomes critical in reducing postoperative morbidity. High irrigation pressure has also been identified as a contributing factor.6
In a clinical study conducted by Croghan et al, patients who developed postoperative sepsis after ureteroscopy were found to have significantly higher mean intrarenal pressures compared to those without infection.7 This was the first human study to directly evaluate the relationship between elevated IRP and postoperative sepsis, providing compelling evidence that pressure control is clinically relevant (Table 1). Dr. Jung also reflected on the potential relationship between pain and elevated intrarenal pressure, though current data remain limited. This observation further illustrates that the consequences of pressure are likely multifactorial, influencing not only infectious outcomes but also patient comfort and recovery.
Table 1.

She then turned to the adverse effects of elevated IRP on renal function. Animal studies have demonstrated irreversible structural damage, including scarring and ischemia. In a clinical setting, patients undergoing URS and PCNL showed increases in five different urinary biomarkers for renal injury, underscoring that functional impact is not limited to experimental models. Dr. Jung also highlighted findings from a recent unpublished porcine study she is conducting. Even after short-term exposure to low pressure levels, investigators observed substantial medullary alterations within the renal parenchyma. She raised concern that these changes may represent the initiation of a pathophysiologic cascade once pressures rise.
Importantly, while guidelines such as the EAU advise keeping pressure “as low as possible,” there is still no universally agreed-upon safety limit. Dr. Jung argued that instead of chasing a single threshold, urologists should focus on identifying risk factors and adopting strategies to mitigate them. Modern tools like pressure-monitoring ureteroscopes and suction access sheaths provide actionable ways to control IRP in real time.
She closed with a clear message: elevated IRP is not just a theoretical concern. It is a real, clinically relevant risk factor that can mean the difference between a routine recovery and life-threatening sepsis. “Intrarenal pressure does matter,” she stated, “and it deserves our full attention.” Dr. Jung concluded by emphasizing that urologists should shift their focus away from chasing a universal ‘safety limit’ and instead prioritize identifying risk factors. The greater aim, she stressed, is to reduce pressure whenever possible in order to protect patients.
Dr. Noah Canvasser began his counterpoint by acknowledging that intrarenal pressure does matter. However, he reframed the debate, asking not whether pressure matters, but whether measuring pressure is clinically necessary. His answer was no.
He opened with a graph illustrating the rise in publications on renal pressure over the past 25 years, noting that the majority of this growth occurred within the last five years. This, he remarked, highlights how rapidly the field’s understanding of intrarenal pressure has evolved. The ability to measure IRP in real time during ureteroscopy is, in itself, a remarkable achievement. At the same time, he cautioned that pressure-sensor guidewires can be technically challenging, dependent on proper orientation for accurate readings. Conversely, surgeons can manage pressure effectively by focusing on inflow and outflow. Inflow can be modulated with hand pumps, pressure bags, or automated irrigation systems. Outflow can be optimized with ureteral access sheaths. Higher inflow without adequate drainage raises pressure, while optimized outflow keeps it low. Hand pumps tend to generate higher pressures than pressure bags or automated systems.8 Surgeons can also tailor their approach to the case: lower settings for infectious scenarios, and higher pressures if a ureteral access sheath is present to accommodate greater outflow.
Dr. Canvasser emphasized that ureteral access sheaths are among the most effective tools for reducing intrarenal pressure. Large multicenter trials have demonstrated their ability to lower postoperative infection rates.9 He then reviewed data from Dr. Bhojani and colleagues using the LithoVue™ (LVE) ureteroscope, which incorporates intrarenal pressure monitoring. In this series, 74% of patients had pressures recorded, with a median of 28.5 mmHg and a maximum of 174 mmHg. More than 90% of cases remained below 60 mmHg, and 73% maintained pressures under 40 mmHg.10
An additional technique to manage outflow is by considering ureteroscope size. Dr. Fang and colleagues coined the term RESD (Ratio of Endoscopic Sheath Diameter), defined as the outer diameter of the endoscope divided by the inner diameter of the ureteral access sheath, as seen in Figure 3.11 When RESD values are ≤0.75, lower intrarenal pressures are typically observed. For example, a 7.5 Fr flexible ureteroscope in an 11/13 Fr sheath yields an RESD of 0.68, which correlates with low IRP. This relationship holds true for most UAS sizes, with the exception of smaller sheaths. However, most pressure studies to date have been performed with the LithoVue™ 9.5 Fr ureteroscope in an 11/13 Fr sheath, producing an RESD of 0.86. Following the RESD principle, this combination would suggest that only the largest sheaths, such as 13/15 Fr, should be used to maintain lower pressures. On the other end of the spectrum, the miniaturized 6.3 Fr ureteroscope consistently achieves RESD values ≤0.66 across all sheath sizes, supporting significantly lower intrarenal pressures (Figure 3).
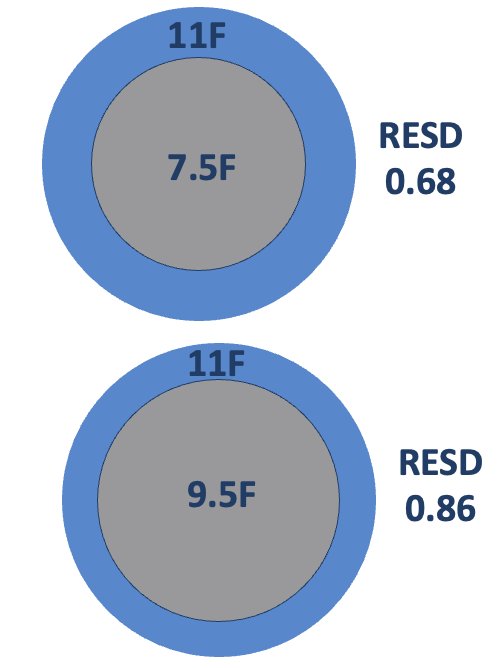
Figure 3.
Suction-enabled access sheaths have consistently demonstrated the ability to decrease intrarenal pressures. Dr. Canvasser referenced work by Fang and colleagues, who used a 3D-printed model to show that suction allowed for higher RESD values while still maintaining low pressures. He then highlighted a study by Ostergar and colleagues from Washington University,12 which evaluated suction in vivo. Using a 9.5 Fr ureteroscope, passive baseline suction showed no significant difference compared to standard non-suction sheaths. However, once suction was actively engaged, intrarenal pressures dropped by 18 mmHg, a meaningful and statistically significant reduction. These findings reinforced his argument that suction sheaths, especially when combined with sheath sizing strategies, offer a practical way to keep intrarenal pressures low without the need for routine measurement.
In the first series of 25 patients treated with suction-enabled UAS and LithoVue™, most had 11/13 Fr sheaths (65%), while the remainder used 12/14 Fr (35%). Irrigation was delivered with pressure bags at 250 mmHg and suction set at 200 mmHg. The median intrarenal pressure was 22 mmHg, compared to 28.5 mmHg in prior non-suction studies. Impressively, as shown in Figure 4, 76% of procedures were maintained below 40 mmHg.13 A closer look at the data revealed that the 12/14 Fr sheath group achieved a median IRP of 14 mmHg, which significantly lowered the overall series median.

Figure 4.
These findings were echoed by a larger multicenter FANS study of nearly 400 patients. In this cohort, procedures using ureteroscope tips ≥8 Fr reported no cases of urosepsis, and only three patients developed postoperative fever, all highly reassuring results.14
In his conclusion, Dr. Canvasser reiterated that while pressure is an important consideration, measuring it is not necessary in daily clinical practice. The combination of access sheaths, suction technology, ureteroscope size selected using RESD parameters, and tailored irrigation allows surgeons to optimize inflow and outflow safely. ‘Pressure is key,’ he noted, ‘but measuring pressure is not required. What matters is optimizing the tools and techniques we already have.’
The moderator thanked both debaters for their thoughtful presentations, and the audience was then invited to cast their votes. When the poll closed, the results were clear: 67% of the audience voted “Yes, renal pressure matters,” while 33% voted “No, it does not.” The outcome reflected the strong arguments presented on both sides, but ultimately suggested that most attendees felt intrarenal pressure deserves deliberate attention in endourologic practice.
Presented by:
- Moderator: Naeem Bhojani, MD, Professor of Urology, University of Montreal
- Helene Jung, MD, PhD, Department of Urology, Hospital Lillebaelt, Denmark
- Noah Canvasser, MD, University of California, Davis, USA
Written by: Mariah Hernandez, Research Specialist, Department of Urology, University of California Irvine, @mariahch00 on Twitter during the 2025 World Congress of Endourology and Uro-Technology (WCET) Annual Meeting, September 8 – September 12, Phoenix, Arizona
References:- Bhojani N, Miller LE, Bhattacharyya S, Cutone B, Chew BH. Risk Factors for Urosepsis After Ureteroscopy for Stone Disease: A Systematic Review with Meta-Analysis. J Endourol. 2021;35(7):991-1000. doi:10.1089/end.2020.1133
- Jung H, Osther PJ. Intraluminal pressure profiles during flexible ureterorenoscopy. Springerplus. 2015;4:373. Published 2015 Jul 24. doi:10.1186/s40064-015-1114-4
- Lildal SK, Hansen ESS, Laustsen C, et al. Gadolinium-enhanced MRI visualizing backflow at increasing intra-renal pressure in a porcine model. PLoS One. 2023;18(2):e0281676. Published 2023 Feb 16. doi:10.1371/journal.pone.0281676
- Somani BK, Giusti G, Sun Y, et al. Complications associated with ureterorenoscopy (URS) related to treatment of urolithiasis: the Clinical Research Office of Endourological Society URS Global study. World J Urol. 2017;35(4):675-681. doi:10.1007/s00345-016-1909-0
- Chugh S, Pietropaolo A, Montanari E, Sarica K, Somani BK. Predictors of Urinary Infections and Urosepsis After Ureteroscopy for Stone Disease: a Systematic Review from EAU Section of Urolithiasis (EULIS). Curr Urol Rep. 2020;21(4):16. Published 2020 Mar 24. doi:10.1007/s11934-020-0969-2
- Corrales M, Sierra A, Doizi S, Traxer O. Risk of Sepsis in Retrograde Intrarenal Surgery: A Systematic Review of the Literature. Eur Urol Open Sci. 2022;44:84-91. Published 2022 Aug 30. doi:10.1016/j.euros.2022.08.008
- Croghan SM, Cunnane EM, O'Meara S, et al. In vivo ureteroscopic intrarenal pressures and clinical outcomes: a multi-institutional analysis of 120 consecutive patients. BJU Int. 2023;132(5):531-540. doi:10.1111/bju.16169
- Croghan SM, O'Meara S, Cunnane EM, et al. Intrarenal pressure with hand-pump or pressurized-bag irrigation: randomized clinical trial at retrograde intrarenal surgery. Br J Surg. 2024;111(6):znae137. doi:10.1093/bjs/znae137
- Traxer O, Wendt-Nordahl G, Sodha H, et al. Differences in renal stone treatment and outcomes for patients treated either with or without the support of a ureteral access sheath: The Clinical Research Office of the Endourological Society Ureteroscopy Global Study. World J Urol. 2015;33(12):2137-2144. doi:10.1007/s00345-015-1582-8
- Bhojani N, Koo KC, Bensaadi K, Halawani A, Wong VK, Chew BH. Retrospective first-in-human use of the LithoVue™ Elite ureteroscope to measure intrarenal pressure. BJU Int. 2023;132(6):678-685. doi:10.1111/bju.16173
- Fang L, Xie G, Zheng Z, et al. The Effect of Ratio of Endoscope-Sheath Diameter on Intrapelvic Pressure During Flexible Ureteroscopic Lasertripsy. J Endourol. 2019;33(2):132-139. doi:10.1089/end.2018.0774
- Ostergar A, Wong D, Shiang A, et al. Intrarenal Pressure with Vacuum-Assisted Ureteral Access Sheaths Using an In Situ Cadaveric Porcine Model. J Endourol. 2023;37(3):353-357. doi:10.1089/end.2022.0573
- Chen KW, Koo KC, Zhong T, et al. Real time monitoring of intrarenal pressures while using the flexible and navigable suction ureteral access sheath. World J Urol. 2025;43(1):76. Published 2025 Jan 17. doi:10.1007/s00345-025-05444-4
- Gauhar V, Traxer O, Castellani D, et al. Could Use of a Flexible and Navigable Suction Ureteral Access Sheath Be a Potential Game-changer in Retrograde Intrarenal Surgery? Outcomes at 30 Days from a Large, Prospective, Multicenter, Real-world Study by the European Association of Urology Urolithiasis Section. Eur Urol Focus. 2024;10(6):975-982. doi:10.1016/j.euf.2024.05.010