(UroToday.com) Wednesday’s plenary session featured Dr. Xu Zhang, who gave a cutting-edge lecture on his team’s two-decade progress in telesurgery development. He highlighted the latest landmark achievements, including intercontinental human robotic procedures.
In the past 20 years, minimally invasive surgery has become the standard, Dr. Zhang began. Robotics now propels us into a new age of development, with three-dimensional vision and complete freedom of movement, enabling procedures outside the limits of laparoscopy.
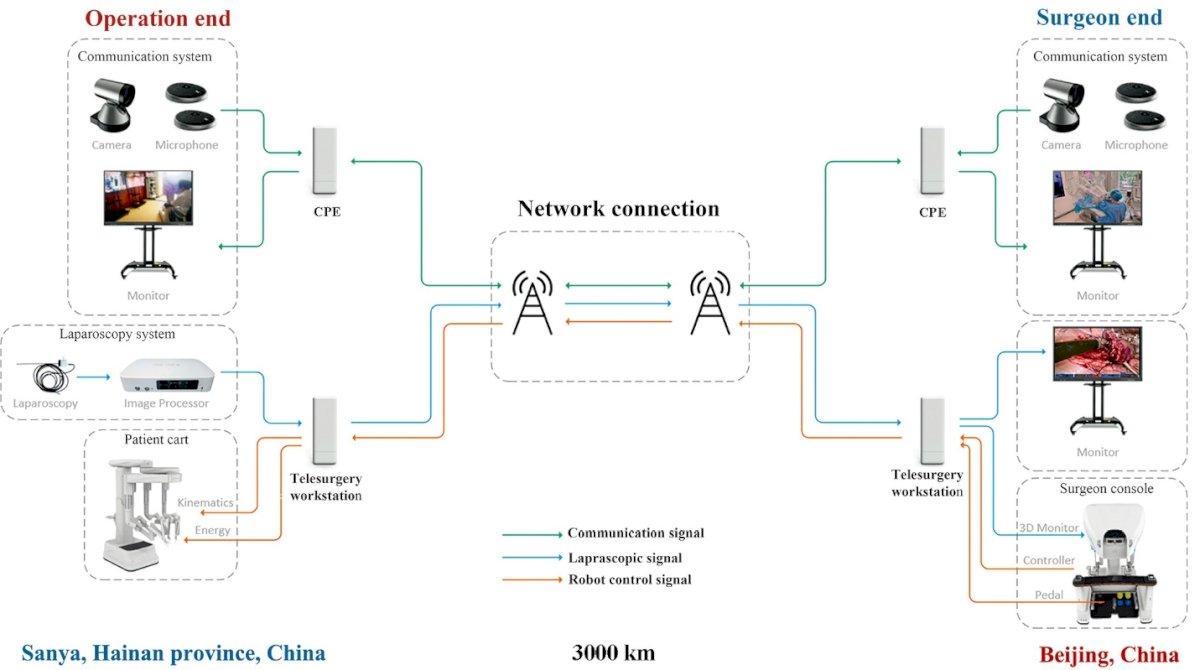
To establish a reliable platform, Dr. Zhang’s team collaborated with Chinese telecommunication partners to integrate telecommunication subsystems, including video and audio communication and high-resolution monitors, teleconference devices for synchronous communication, and robotic surgical systems that offer real-time remote operation.
The system was rigorously tested on a 3,000 km connection between Beijing, where the surgeon console was located, and Sanya, Hainan Province, the site of operation. The schematic below illustrates the dual-end setup, where cameras, microphones, and monitors input to telesurgery workstations that connect across a high-speed 5G optical fiber backbone.
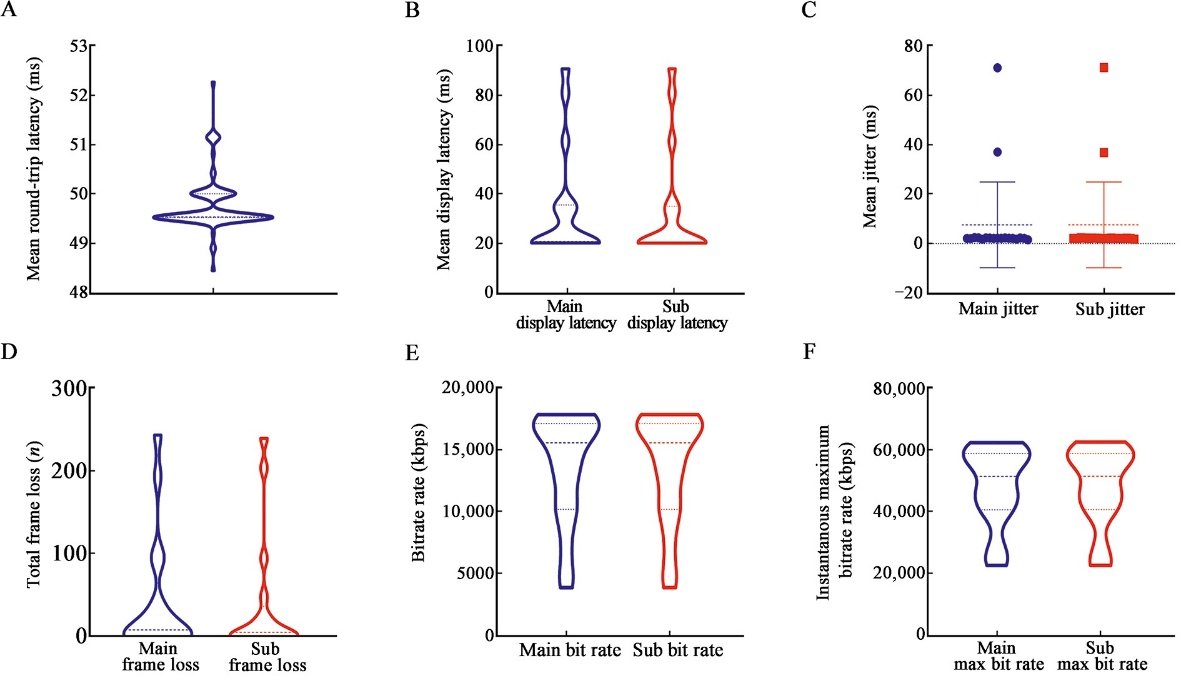
In preclinical validation studies, latency was determined to be a significant parameter in defining the success of telesurgery. Dr. Zhang explained that his team conducted over 108 laparoscopic procedures with more than 3,866 minutes of operative time in pigs. These procedures included partial nephrectomy, nephrectomy, nephroureterectomy, ureterobladder replantation, ureteral anastomosis, bladder rupture repair, prostatectomy, pelvic lymph node dissection, repair of ruptured inferior vena cava, small intestine anastomosis, repair of uterine rupture, and oophorectomy. Through these operations, the team quantified various communication metrics, including round-trip latency (approximately 50 ms, Figure A), display latency (Figure B), jitter (< 10 ms, Figure C), frame loss (< 200 frames, Figure D), and bitrate (Figures E and F). “Latency under 200 milliseconds is generally safe,” Dr. Zhang stated. “Once latency exceeds 300 milliseconds, operations become difficult to perform.”
Dr. Zhang then presented his results on bandwidth studies, which demonstrated that > 5 Mbps was sufficient for stable telesurgical performance. Nevertheless, even with low-bandwidth conditions < 5 Mbps, critical events such as simulated vascular rupture could still be managed safely, though with less efficiency. These findings were published in the Chinese Medical Journal earlier this year.
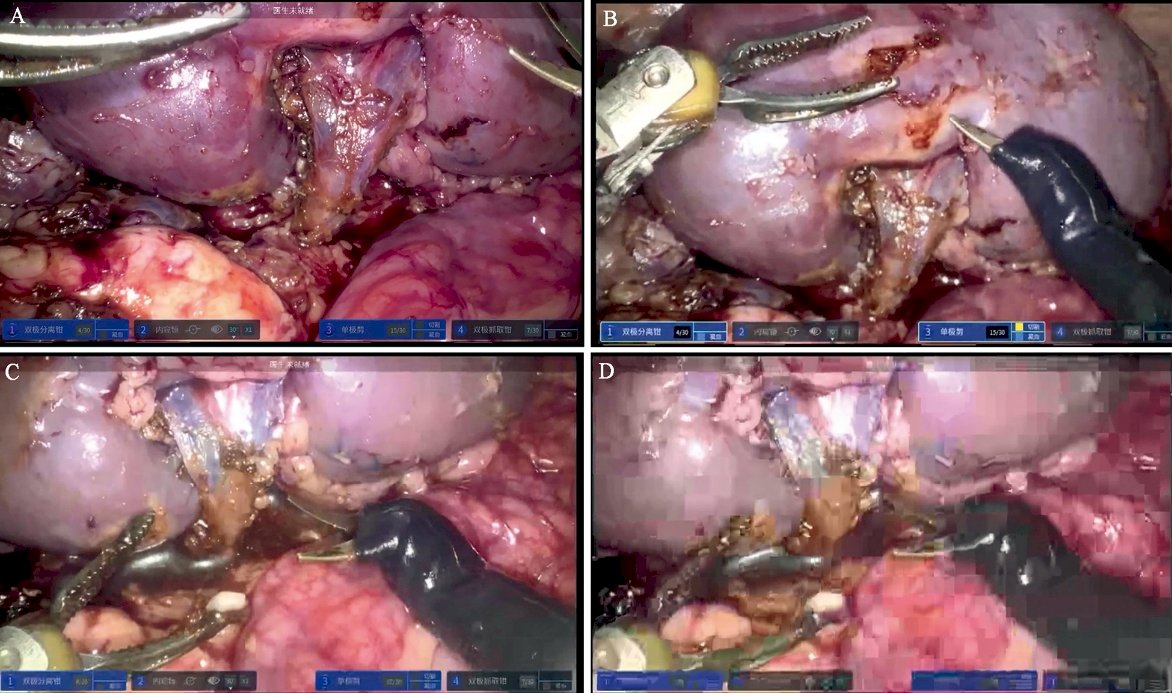
From Dr. Zhang’s publication in the Chinese Medical Journal, the above figure shows laparoscopic images under different bandwidths in partial nephrectomy. (A) 15–20 Mbps, very clear; (B) 10–15 Mbps, clear; (C) 1–5 Mbps, unclear; and (D) less than 1 Mbps, blurry.
Surgeon workload was evaluated using the NASA Task Load Index (NASA-TLX). The analysis showed minimal increases in the surgeon’s mental and physical demand, no significant increase in frustration, and stable effort and performance scores, supporting that remote operation did not impose additional burden as compared with conventional robotic surgery.

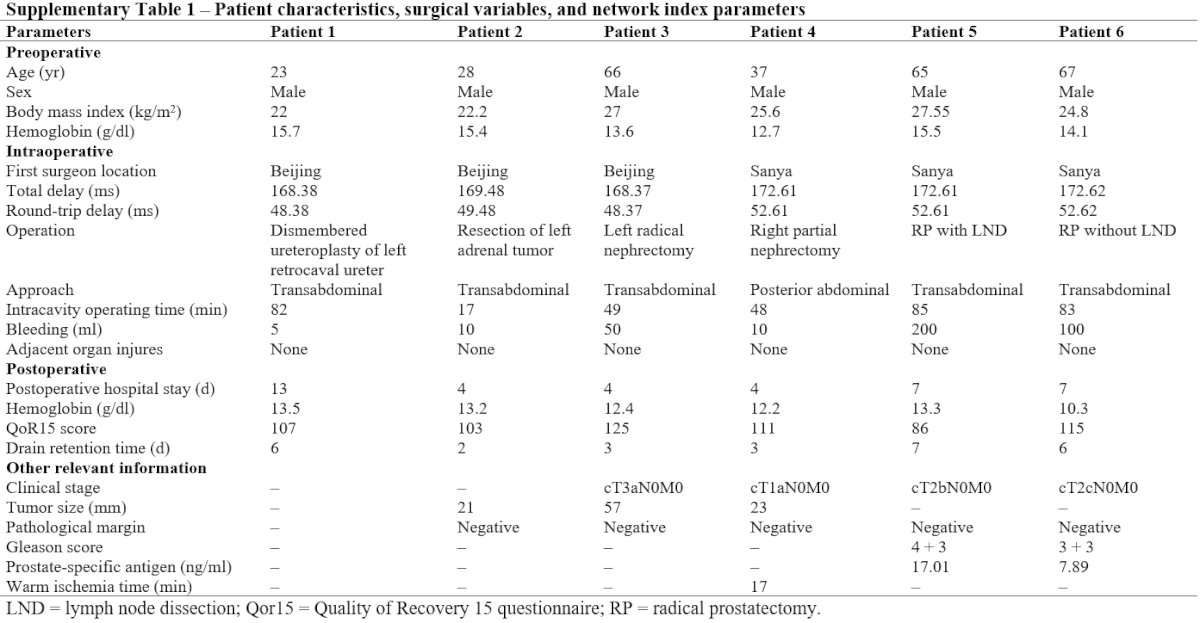
Following preclinical validation experiments, Dr. Zhang’s group conducted an ethics-approved exploratory clinical trial in Beijing. Six urological cases were performed with telesurgery, including one retrocaval ureteral reconstruction surgery, one adrenal tumor resection, one radical nephrectomy, one partial nephrectomy (retroperitoneal approach), and two radical prostatectomies. In this study, the real-time round-trip network latency ranged from 48.37 to 52.20 ms, with jitter of <1 ms. The latency for video encoding and decoding remained stable at about 20 ms. No significant differences were observed in outcomes compared to conventional robotic surgery. Two-week follow-ups demonstrated no complications.
Dr. Zhang then described expanding his work internationally, performing telesurgery across 20,000 kilometers, linking Beijing to Rome. “It felt as if the tissue was right at hand, under complete control,” he recalled. “Even with such long distances, latency was acceptable and did not affect performance.” He performed a total of 4 cases, marking the first reported cases of intercontinental telesurgery in humans. This research is soon to be published in a journal.
Concluding his talk, Dr. Zhang emphasized that telesurgery, combined with advances in AI, high-speed communication, and supercomputing, will revolutionize current surgical practice.
Presented by: Xu Zhang, MD, PhD, Chinese PLA General Hospital, Beijing, China
Written by: Helen Gao, Medical Student at Robert Wood Johnson Medical School, Leadership and Innovation Fellowship Training (LIFT) Scholar at Department of Urology, University of California, Irvine. @helengao295 on X during the 2025 World Congress of Endourology and Uro-Technology (WCET) Annual Meeting: September 8 – September 12, 2025, Phoenix, ArizonaReferences:
- Wang Y, Ai Q, Zhao W, et al. Safety and Reliability of a Robot-assisted Laparoscopic Telesurgery System: Expanding Indications in Urological Surgery. Eur Urol. 2024;85(5):506-507. doi:10.1016/j.eururo.2023.11.002
- Wang Y, Ai Q, Shi T, et al. Influence of network latency and bandwidth on robot-assisted laparoscopic telesurgery: A pre-clinical experiment. Chinese medical journal. 2025;138(3):325-331. doi:10.1097/CM9.0000000000003257