(UroToday.com) Tuesday morning’s plenary session started with an engaging lecture from Dr. Andrew Hung about the future role of artificial intelligence (AI) in urology. In this session, he stressed that AI should be viewed as an aid to surgical performance rather than a replacement for urologists: “According to ChatGPT, surgical AI is the use of AI technologies in surgical procedures to assist and enhance what surgeons do. Notice that it didn’t say replace, thank goodness.”
Dr. Hung began by defining surgical AI as the use of computational tools to analyze and understand large amounts of data produced before, during, and after operations. He highlighted the significant amount of perioperative data that often goes unused: “Most of this data is left on the table, meaning that it’s not being used to its fullest potential. I really do see AI as an opportunity for us to use that data to better inform us before surgery, during surgery, and even afterwards.” He showed how AI can meaningfully guide each stage of the surgical pathway, from patient selection and planning to intraoperative decision-making, and postoperative care and recovery.
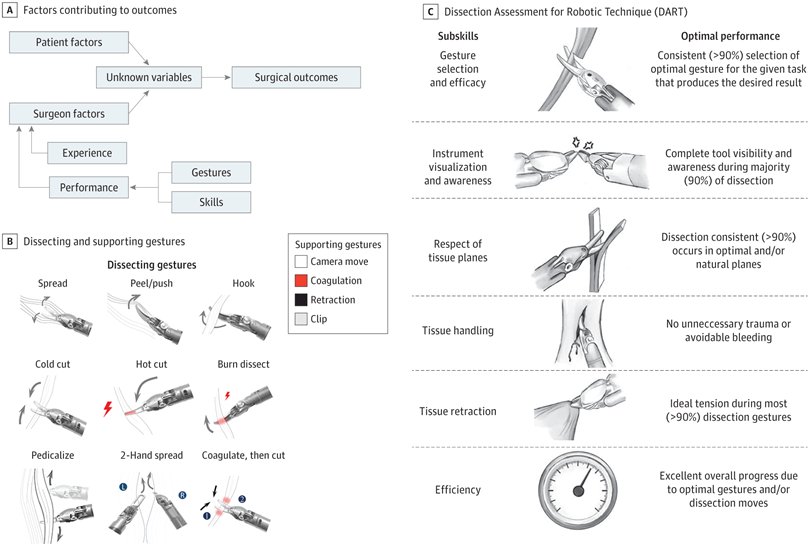
A key area of Dr. Hung’s research has been the automated classification of surgical gestures. Specific surgical maneuvers on the robotic system, such as spread, hook, peel, push, or energy use, can be treated as “letters of the surgical alphabet.” When combined, they form “words” and “sentences,” representing functional units of entire operations. AI models can be trained to decode entire operations into sequences of gestures.
Dr. Hung presented data from his lab evaluating nerve-sparing prostatectomy cases. Traditional statistical methods often failed to accurately predict which patients will recover sexual function one year after surgery. However, Dr. Hung explained, “If you plug them into specialized AI models that have memory of one gesture to the next, we can now predict with an 85% accuracy whether or not this patient will recover function.” AI can model sequences of dissection gestures during operations for patients who recovered versus those who did not regain erectile function at 12 months.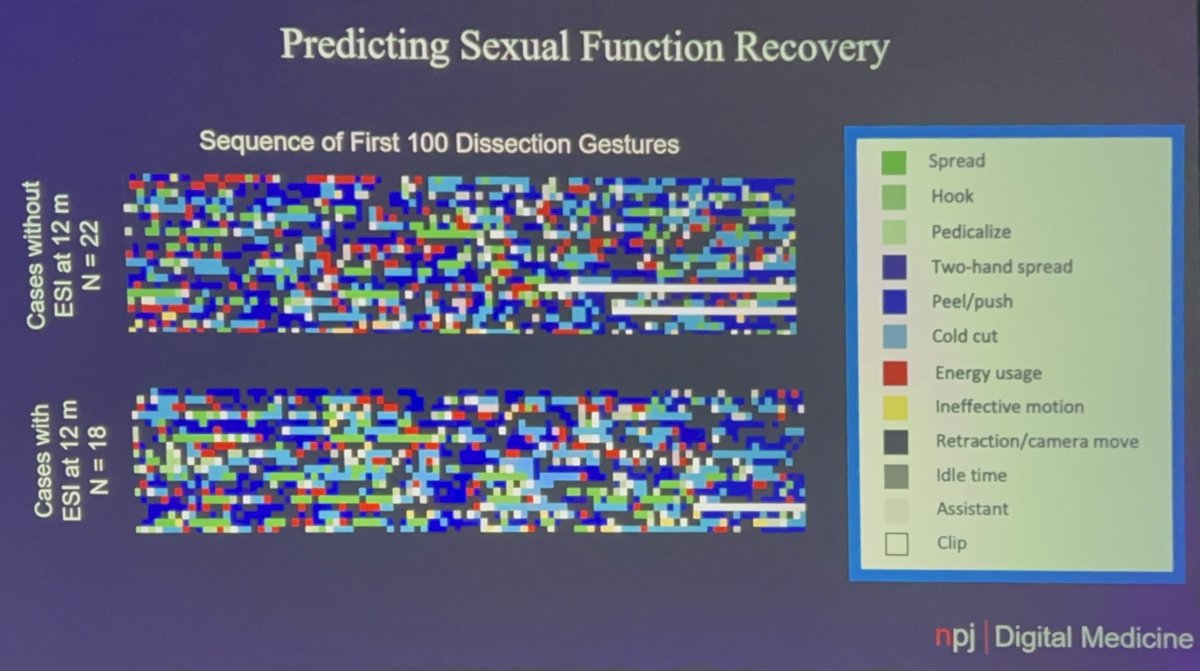
Figures from Dr. Hung’s lab show how various dissection gestures differed between patients who did and did not recover erectile function at 12 months. Quoting directly from his group’s published work: “To understand how these models make predictions, we ... ranked the important clinical features for 1-year EF prediction, which were Gleason score, age, BMI, PSA, and prostate volume. We also outputted important gesture sequences positively or negatively associated with 1-year EF recovery.”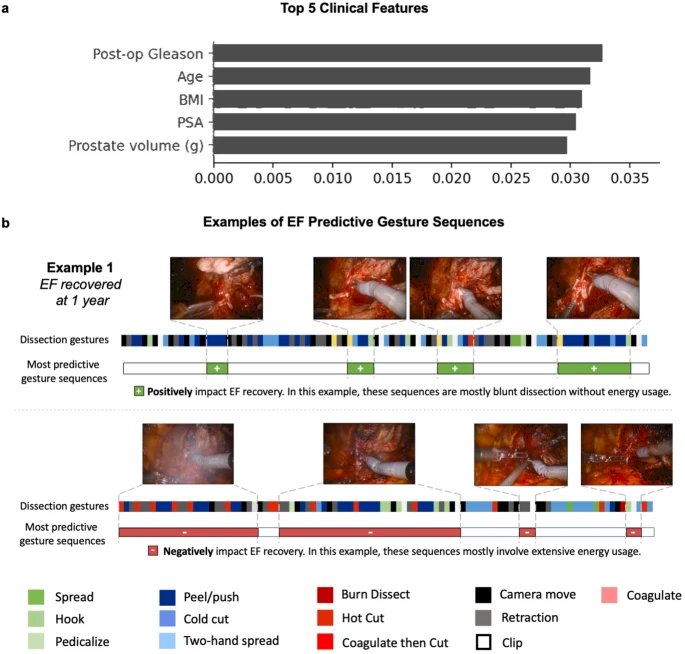
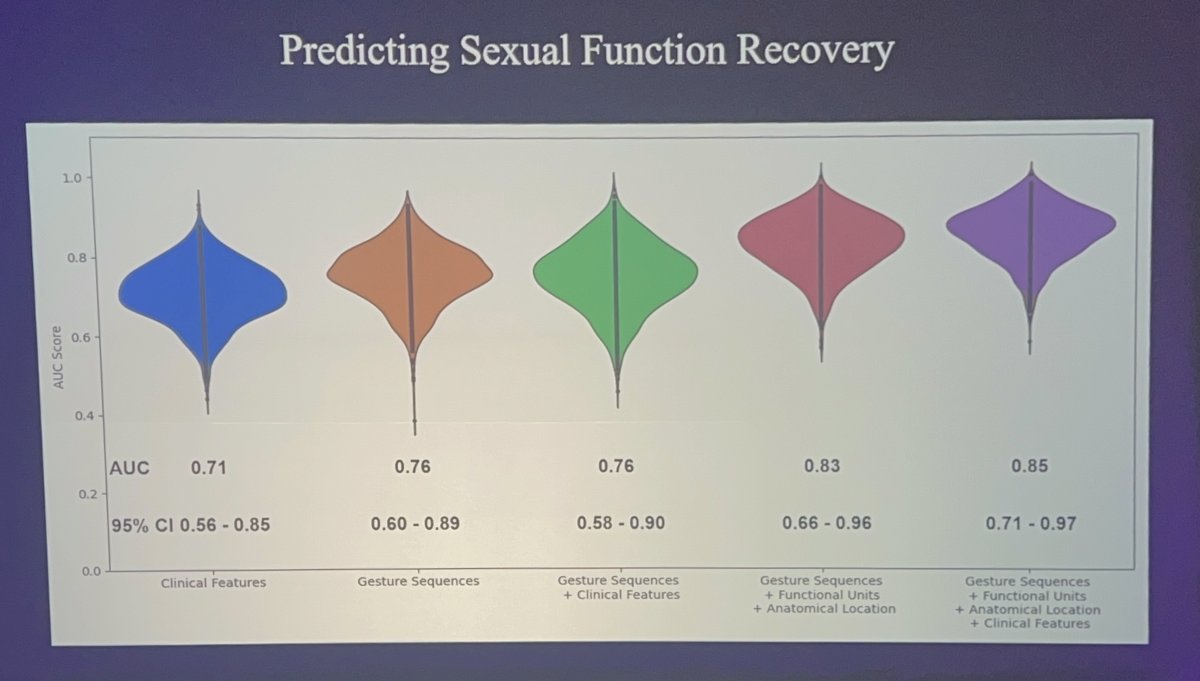
Combining gesture sequences with anatomical location and clinical features progressively improved model accuracy to an area under the curve (AUC) of 0.85.
Dr. Hung identified automated image segmentation as a major breakthrough in the past two years: “Image segmentation has been groundbreaking. It has changed the way that I have done my research, but also in radiology and pathology.” By isolating only relevant anatomical structures in an operation, such as the neurovascular bundle in a prostatectomy, AI systems can provide precise feedback on technical factors, including tissue traction and retraction angle, which correlate with postoperative recovery.
Dr. Hung then highlighted work from international collaborators who have advanced augmented reality for robotic surgery. He showcased the work of Dr. Jean-Christophe Bernhard from the University of Bordeaux, who trained a model on 41,000 annotated images from 170 cases. This enabled overlay of preoperative imaging onto the live kidney in real time. By merging preoperative imaging with the live surgical field, these systems can delineate tumor margins, vascular structures, and instruments with high accuracy, greatly improving intraoperative navigation.
Finally, Dr. Hung discussed advancements in autonomous robotic surgery. By using imitation learning rather than reinforcement learning, research groups have trained surgical robots to perform tasks such as tying knots, lifting flaps, and suturing with high reliability, and ultimately perform autonomous cholecystectomy. Dr. Hung explained, “This is not video editing — it knows what it’s doing. It knows where the duct is, it knows where to place two clips below and one above, and it autonomously changes its instrument. That’s miraculous.” While still in the early stages, these advances suggest that autonomous procedures may not be as far off as previously thought.
Concluding his lecture, Dr. Hung emphasized that AI has already proven value in surgical assessment, computer vision, augmented reality, and autonomous robotics, and that the next step is to demonstrate consistent benefits for patients in real-world practice. He ended with a challenge: “AI is truly here to enhance urology…my challenge to you is to think about how we can not only show it in the lab but also show it in the operating room and show value there.”
Presented By: Andrew Hung, MD, Cedars Sinai Medical Center, Los Angeles, CA
Written By: Helen Gao, Medical Student at Robert Wood Johnson Medical School, Leadership and Innovation Fellowship Training (LIFT) Scholar at Department of Urology, University of California, Irvine. @helengao295 on X during the 2025 World Congress of Endourology and Uro-Technology, September 8 – September 12, 2025, Phoenix, Arizona
References:
- Cui, Zijun, and Andrew J. Hung. "What is artificial intelligence, machine learning, and deep learning: terminologies explained." Artificial Intelligence in Urology. Academic Press, 2025. 3-17.
- Ghaffar, Umar, Heard, J., Ma, R., et al. "Surgical Gesture Utilization and Efficacy Trends Between Retractions in Surgeons Performing the Robot-Assisted Nerve-Sparing Prostatectomy." Journal of Endourology 39.5 (2025): 457-463.
- Heard JR, Ghaffar U, Ma R, et al. Surgical Performance Metrics for 1-Year Patient-Reported Outcomes After Radical Prostatectomy. JAMA surgery. 2025;160(6):674. doi:10.1001/jamasurg.2025.0931
- Hung, Andrew J. "Future directions for AI in urology." Artificial Intelligence in Urology: Present and Future (2024): 295.
- Kiyasseh, D., Ma, R., Haque, T.F. et al. A vision transformer for decoding surgeon activity from surgical videos. Nat. Biomed. Eng 7, 780–796 (2023). https://doi.org/10.1038/s41551-023-01010-8
- Ma, R., Ramaswamy, A., Xu, J. et al. Surgical gestures as a method to quantify surgical performance and predict patient outcomes. npj Digit. Med. 5, 187 (2022). https://doi.org/10.1038/s41746-022-00738-y
- Pitout A, Margue G, Rubat Baleuri F, et al. Assessing Oncologic and Functional Outcomes of 3D Image-Guided Robotic-Assisted Partial Nephrectomy (3D-IGRAPN): A Prospective Study (UroCCR-186). Cancers. 2025;17(13):2127. doi:10.3390/cancers17132127
- Saeidi, Hamed, Opfermann, J. D., Kam, M., et al. "Autonomous robotic laparoscopic surgery for intestinal anastomosis." Science robotics 7.62 (2022): eabj2908.