(UroToday.com) On the second day of the World Congress of Endourology and Uro-Technology, during the inaugural plenary session, Dr. Jeremy Teoh, MBBS, FRCSEd, FCSHK, FHKAM of The Chinese University of Hong Kong presented a State-of-the-Art lecture regarding a Transurethral Robotic Platform in the management and treatment of bladder tumors. Bladder cancer affects individuals worldwide, with nearly 550,000 patients diagnosed annually1.
Around 75% of this population will ultimately present with non-muscle-invasive bladder cancer (NMIBC). Traditional treatment for NMIBC includes transurethral resection of bladder tumor (TURBT), or standard resection (SR), allowing for the resection of all observable tumors without disruption to the bladder wall. Given high recurrence rates within 5 years (31-78%), adjunct treatments have emerged for optical oncologic outcomes, including Bacillus Calmette-Guérin (BCG) therapy and mitomycin C instillation. En bloc tumor resection (ERBT) has been proposed as an alternative technique, allowing for the complete removal of the tumor and surrounding tissue (Figure 1).
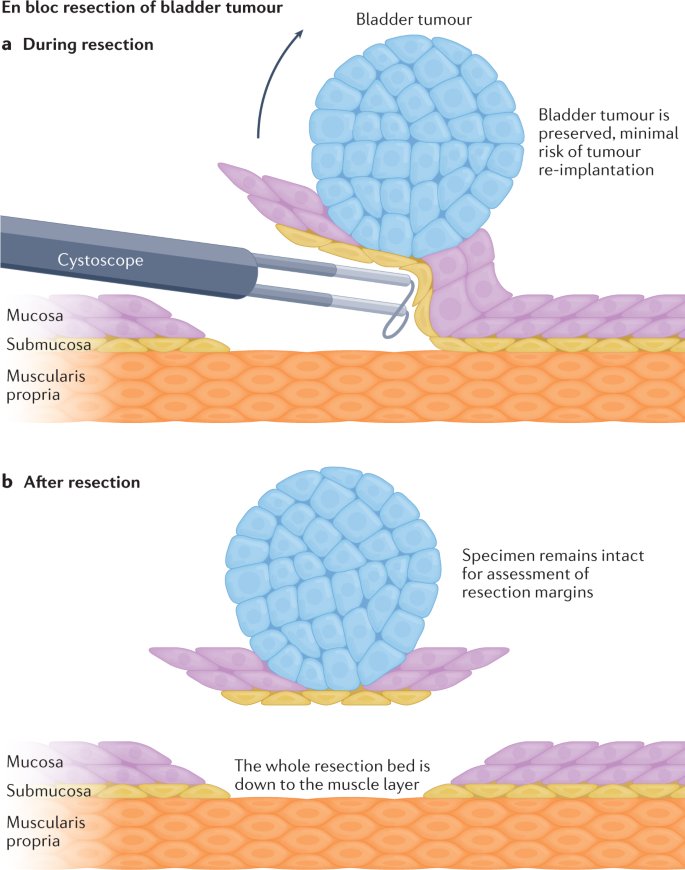
Figure 1. A) Illustrative demonstration of En bloc resection of bladder tumor. B) Resection of the detrusor muscle layer, with intact bladder tumor.
During his introduction, Dr. Teoh reaffirmed the integral role of ERBT within his surgical practice. In a 2024 randomized multicenter trial in the comparison of standard resection (SR) vs ERBT for patients with non-muscle invasive bladder cancer (NMIBC) with tumors ≤3 cm, Dr. Teoh and colleagues found recurrence rates had the potential for reduction from 38% in SR to 28% in ERBT. For patients treated with both ERBT and BCG, one-year recurrence rates were as low as 5% 2. He supported his initial remark, sharing that successful surgery in conjunction with adjuvant treatment can possibly cure patients with NMIBC.
Through his prior work, Dr. Teoh determined that ERBT may offer a promising future for the treatment of NMBIC, though he was soon met with an internal conflict: How could ERBT be implemented across institutions worldwide to ensure optimal quality of surgical techniques with current tools? After attending NARUS 2024, Dr. Teoh found his solution – The Virtuoso Surgical Endoscopic System (Virtuoso Surgical Inc., Nashville, TN). This robotic system contains two manipulators in a concentrated system that decreases the scale of robotic surgery by tenfold (Figure 2). Within the tip of a 26Fr rigid endoscope, two manipulators are dispensed, allowing for ease of manipulation and tissue cutting by surgeons. The camera is able to be fully rotated up to 180 degrees, wherein “lateral wall tumors are transformed into posterior wall-like tumors”. The console unit includes a mounted station with two joystick handles, while also allowing for the surgeon to operate in a seated or standing position. The first in-human trial was completed in May 2025 by Dr. Teoh, with 6 patients in the first phase. All patients had tumors ≤3 cm, with various locations including the lateral wall, posterolateral wall, and anterior dome. Two of these patients included more challenging tumors, with locations close to the ureteral orifice (UO).

Figure 2. Virtuoso Surgical Endoscopic System
In traditional transurethral surgery, the implementation of larger instruments presents several challenges. Bulky instrument arms may obstruct endoscopic view, restrict cross-arm maneuvering, and limit the deployment of flexible instruments in single-port surgery. The Virtuoso system addresses these limitations through its concentric tube design and smaller tube instruments. To highlight these advantages, Dr. Teoh presented intraoperative cases, including a bladder tumor near the UO (Figure 3). As his surgical video progressed, depicting precise cutting and cross-arm maneuvers, Dr. Teoh emphasized, “Suddenly it becomes a very anatomical procedure, trying to find the layers, trying to find the junction between the submucosa and also muscle layers.”
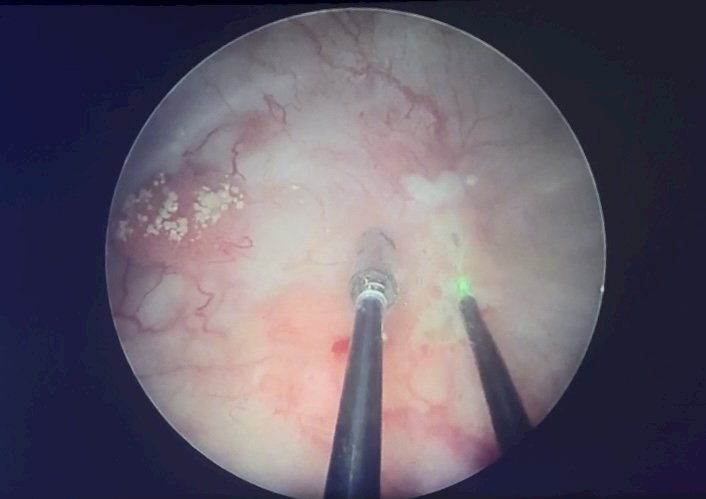
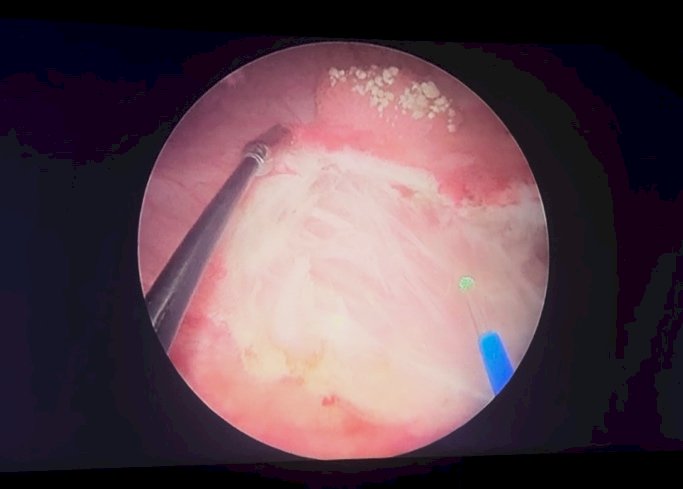
Figure 3. Intraoperative screen capture of video demonstration for the Virtuoso Surgical Endoscopic System. A). Identification of bladder tumor. B). Surgical resection of bladder tumor via En Bloc technique.
Dr. Teoh’s second operative case presented a greater degree of difficulty, involving a bladder dome tumor. The maneuverability and flexibility of the Virtuoso camera permitted a 180° rotation, effectively transforming the lesion into a “posterior” tumor without reciprocal instrument movement issues. This facilitated excision in a standard manner, though several challenges inherent to en bloc resection were emphasized. Tumors located deep within the bladder require instruments capable of sufficient reach. Dome tumors necessitate precise angulation and careful docking of the robotic system. In the context of bladder neck tumors, surgeons must remain cautious of excessive depth to avoid perforation. Throughout his presentation, Dr. Teoh stressed adherence to oncologic principles and highlighted the importance of avoiding overly deep dissection to preserve bladder integrity.
Across six procedures performed over two days, the Virtuoso system demonstrated strong feasibility and safety outcomes. The mean procedure time was 50.8 minutes, with a mean laser time of 25 minutes. Technical success was achieved in 100% of cases, as all specimens contained detrusor muscle, the study’s primary endpoint. On pathology, five patients were found to have Ta disease; all en bloc specimens demonstrated clear resection margins, and all tumor base samples were negative. One patient was found to have T2 disease with focal deep margin involvement; however, the second-look TURBT was negative, supporting a bladder-sparing approach. No grade ≥3 complications were observed. Results have been submitted to the FDA, and as of September 5, the Virtuoso system has advanced into the FDA Breakthrough Device designation program, with an anticipated accelerated review and development timeline toward 2026 approval.
In addition to en bloc tumor resection, the Virtuoso robotic platform demonstrates potential for a wide range of urologic applications, including transurethral partial cystectomy, transurethral ureteric reimplantation, transurethral diverticulectomy, and transurethral bladder cuff excision. These possibilities underscore the disruptive potential of this system to expand the field of minimally invasive urologic surgery.
Dr. Teoh concluded his presentation with the following take-home messages:
- Urologists have historically led innovation in robotic surgery, progressing from multi-port to single-port platforms.
- The transurethral robotic platform represents the next breakthrough in robotic surgery.
- True innovation requires disruption combined with real, clinical value, a principle urologists must continue to embrace.
Presented by: Jeremy Teoh, MD, Associate Professor, The Chinese University of Hong Kong, Urology
Written by: Mariah Hernandez, Research Specialist, Department of Urology, University of California, Irvine, @mariahch00 on Twitter during the 2025 World Congress of Endourology and Uro-Technology (WCET) Annual Meeting, September 8 – September 12, Phoenix, Arizona
References:
- Teoh JY, Kamat AM, Black PC, Grivas P, Shariat SF, Babjuk M. Recurrence mechanisms of non-muscle-invasive bladder cancer - a clinical perspective. Nat Rev Urol. 2022;19(5):280-294. doi:10.1038/s41585-022-00578-1
- Teoh JY, Cheng CH, Tsang CF, et al. Transurethral En Bloc Resection Versus Standard Resection of Bladder Tumour: A Randomised, Multicentre, Phase 3 Trial. Eur Urol. 2024;86(2):103-111. doi:10.1016/j.eururo.2024.04.015