(UroToday.com) The World Congress of Endourology and Uro-Technology kicked off its first plenary session with a lively and data-rich presentation by Dr. Benjamin K. Canales (University of Florida) titled “Diabetic Medications and the Potential for Stone Prevention.” Dr. Canales opened with a sweeping heterogeneous overview of antidiabetic drug classes currently in use.
He acknowledged the overwhelming array of antidiabetic drug classes, noting that while many are essential for glucose control, only a select few show potential relevance for nephrolithiasis (Figure 1). His talk focused on three classes in particular: pioglitazone, sodium-glucose cotransporter 2 inhibitors (SGLT2i), and the weight-loss combination of phentermine with topiramate.
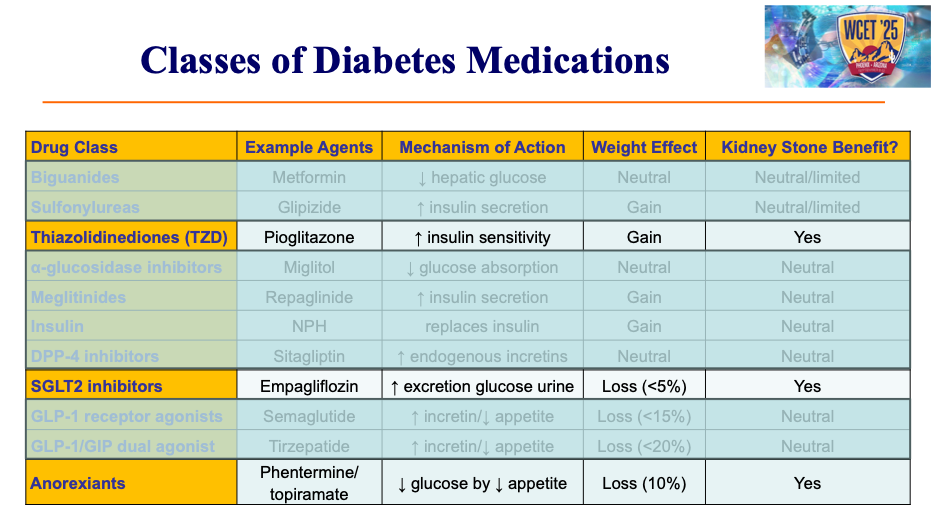
Figure 1.
Pioglitazone, a thiazolidinedione that improves insulin sensitivity in fat and muscle, has been hypothesized to exert parallel effects in the kidney. Investigators tested this concept in a randomized placebo-controlled trial of 36 uric acid stone formers for a duration of 6 months with pioglitazone 30 mg, two-thirds of whom were not diabetic. The trial demonstrated modest increases in urine pH (approximately 0.2 units) and urinary ammonium excretion, both of which would be expected to reduce uric acid stone risk. However, these benefits were offset by unwanted side effects. Participants experienced an average 2-3% increase in body weight, and urinary calcium excretion rose by nearly 20%. This raised concerns about a possible predisposition toward calcium-based stones. Dr. Canales summarized the clinical implications bluntly: although physiologically interesting, pioglitazone has not found a place in the management of uric acid stone disease.
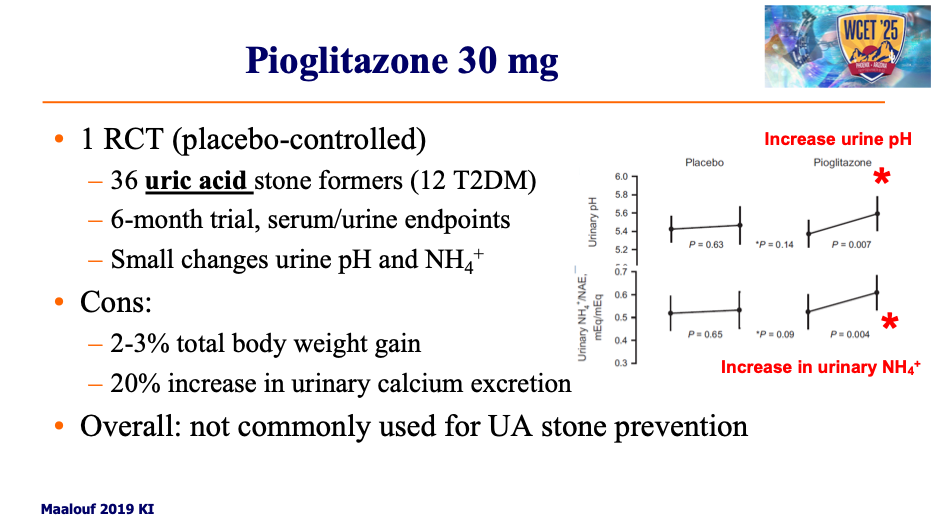
Figure 2.
He then turned to the SGLT2 inhibitors, a class that includes canagliflozin, dapagliflozin, and empagliflozin. These agents act in the proximal tubule to block sodium-glucose reabsorption, leading to glycosuria and an osmotic diuresis that transiently increases urine volume, sodium, and citrate. Over time, SGLT2 inhibitors exert anti-inflammatory effects, promote weight loss, stabilize atherosclerotic plaque, and reduce fibrosis across multiple organs, including the kidney (Figure 3).
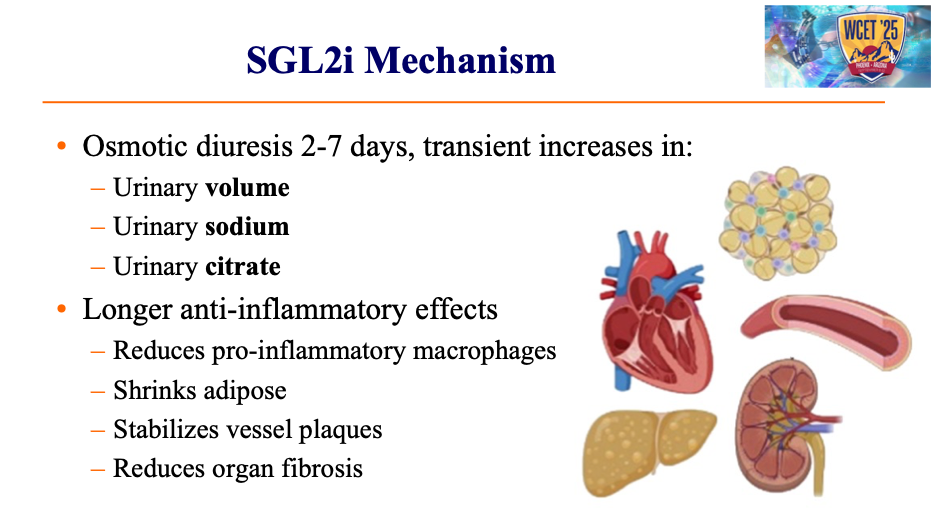
Figure 3.
Drawing on a meta-analysis of seven studies published over the last five years, including retrospective cohorts totaling more than a million adult patients, Dr. Canales showed that diabetic populations on SGLT2 inhibitors consistently experienced a small but measurable reduction in incident stone risk (Figure 4). However, the magnitude of this benefit is low, only about one to two fewer stone events per 1,000 patient-years. As Dr. Canales pointed out, primary care physicians prescribe these drugs to improve cardiovascular and renal outcomes, not for stone prevention, though any effect on nephrolithiasis is a welcomed secondary advantage. He did emphasize that data on recurrent stone prevention remain limited, and these agents should not be recommended as primary therapy for stone formers.

Figure 5.
The question of whether SGLT2 inhibitors might benefit stone formers without diabetes was addressed in the SWEETSTONE trial, a randomized crossover study published in 2024 from Switzerland (Figure 5). Approximately 20 calcium oxalate and 20 uric acid stone formers were treated with empagliflozin 25 mg or placebo for two-week intervals with 24-hour urine collections. The investigators reported a 36% reduction in calcium phosphate supersaturation and a 30% reduction in uric acid supersaturation during the active drug phase. While these results appear promising, closer inspection reveals important limitations. Both calcium phosphate values remained within the normal range, and both uric acid values remained above the abnormal threshold, casting doubt on the clinical significance of the findings. Moreover, the changes were transient, likely reflecting homeostatic adaptation, and thus insufficient to justify recommending SGLT2 inhibitors as first- or second-line stone prevention therapy. Dr. Canales concluded that while these agents may hold potential in select refractory patients, there is currently no evidence to support their use in broader stone populations.

Figure 6.
Lastly, Dr. Canales addressed an anorexiant, Qsymia® (a combination of phentermine and topiramate). Phentermine, a sympathomimetic appetite suppressant approved in 1959, remains the most prescribed weight-loss drug in the United States. Topiramate, a carbonic anhydrase inhibitor, is known for its bicarbonate-wasting properties that can alter urinary chemistry and is also frequently prescribed off-label to blunt addictive behaviors/inhibit cravings ranging from gambling and alcohol to food and tobacco.
Recognizing both its widespread use and mechanistic potential, Dr. Canales and colleagues conducted an 18-month open-label randomized controlled trial of the combination in obese, diabetic uric acid stone formers with normal renal function. Eligible participants were adults between the ages of 18 and 75 who had recurrent uric acid stones, a body mass index greater than 30, and either pre-diabetes, type 2, or insulin-dependent diabetes, with preserved renal function defined by an eGFR above 60. Patients were excluded if they had contraindications to phentermine or topiramate or if they were already receiving anti-obesity pharmacotherapy.
The primary outcome of CT-measured stone volume demonstrated striking results: patients receiving phentermine/topiramate experienced a 52% reduction in stone volume, whereas controls, most of whom were on potassium citrate, experienced an 8% increase. This difference reached statistical significance and suggested a meaningful therapeutic effect (Figure 7).
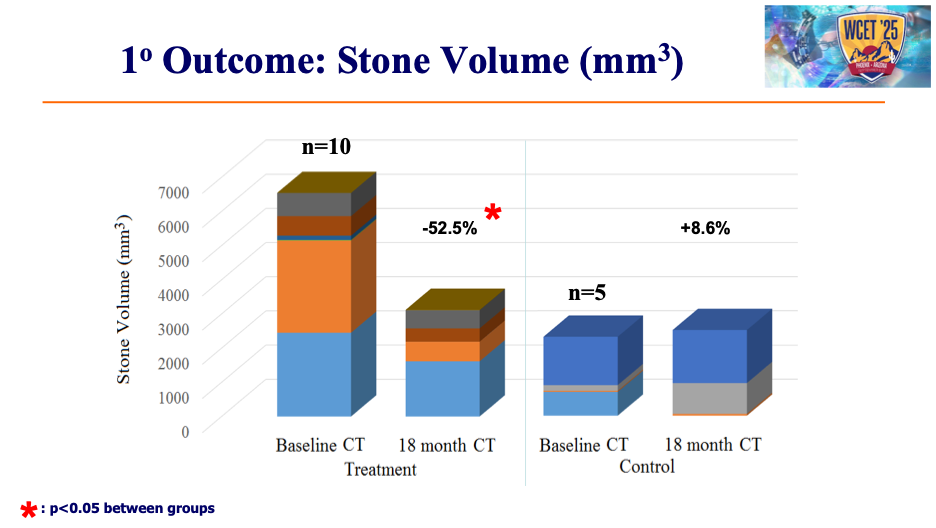
Figure 7.
Secondary outcomes reinforced the benefit (Figure 8). Patients on phentermine/topiramate lost an average of 22 pounds, with changes evident as early as three months. Urine pH rose dramatically, reaching values of 6.2 to 6.3 compared with 5.5 to 5.6 in the control group. Uric acid supersaturation declined significantly by six months and remained low at 18 months, while hemoglobin A1c levels also improved. Despite these encouraging results, there caveats remained. By the end of the study, treated patients exhibited significant hypocitraturia, raising concerns about a shift toward calcium phosphate stone risk. Correspondingly, calcium phosphate supersaturation increased steadily from month three onward. Dr. Canales emphasized that while the drug demonstrates short- to medium-term safety and efficacy, larger trials, particularly those directly comparing phentermine/topiramate with citrate therapy, are required to define its role in stone management
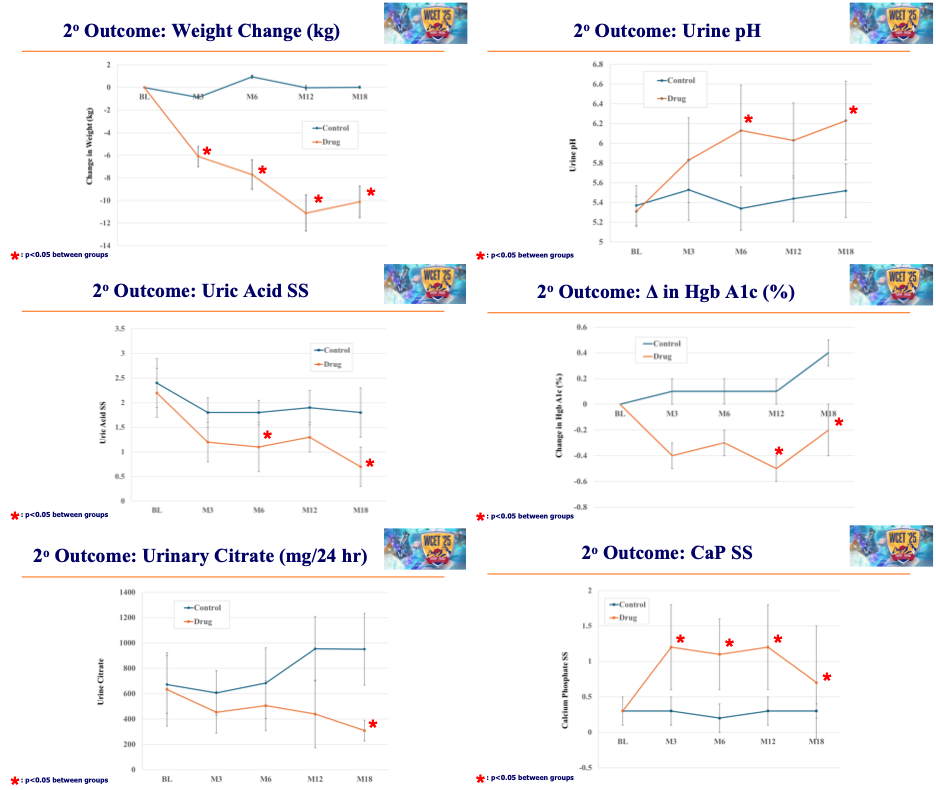
Figure 8.
In conclusion, Dr. Canales distilled his findings into a pragmatic summary. Pioglitazone offers little promise, with risks outweighing benefits. SGLT2 inhibitors appear to modestly alter the urinary environment in a favorable direction but are not supported as stone-specific therapies. Phentermine/topiramate appears to be a novel, safe, and tolerable option in the short to medium term, demonstrating meaningful reductions in stone burden and body weight, but its long-term safety remains uncertain and will require head-to-head trials against citrate therapy to be fully established. Taken together, these observations suggest that while diabetic medications are unlikely to replace established stone therapies, they may offer innovative adjunctive strategies in carefully selected patients.
Presented By: Bejamin K. Canales, MD, Associate Professor and Director of Urologic Research in the Department of Urology at the University of Florida College of Medicine, University of Florida, Gainesville, FL
Moderated by: LaMont Barlow, MD; Jaime Landman, MD; Burak Turna, MD
Plenary Chair: Norberto Osvaldo Bernardo, MD; Andreas J. Gross, MD; Li-Ming Su, MD
Written by: Seyed Amiryaghoub M. Lavasani, B.A., University of California, Irvine, @amirlavasani_ on Twitter during the 2025 World Congress of Endourology and Uro-Technology (WCET) Annual Meeting, September 08-12, 2025, Phoenix, Arizona, USA