(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting was host to a prostate cancer session. Dr. Samson Fine discussed clinically significant prostate cancer, highlighting that not all pattern 4 prostate cancer acts the same.
At the 2025 SUO Annual Meeting, the session on prostate cancer pathology featured an important State-of-the-Art lecture by Dr. Samson Fine outlining how refinements in grading—particularly the evolving role of pattern 4 and cribriform morphology—are reshaping risk assessment. The presentation emphasized the growing consensus that histo-architectural features beyond traditional Gleason patterning offer meaningful prognostic value and should be incorporated into contemporary clinical decision-making.1
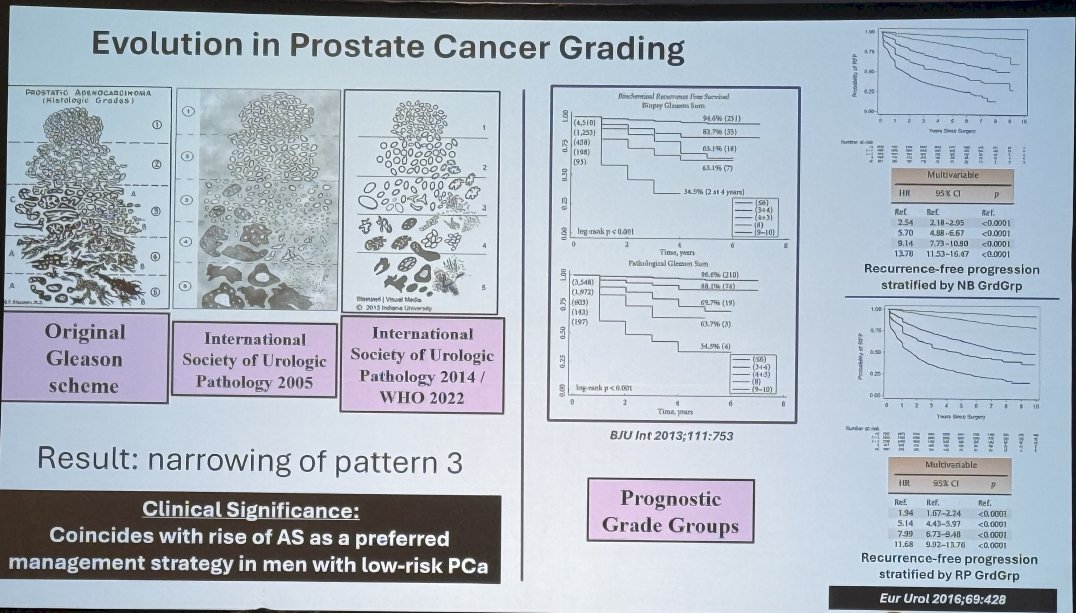
Evolution in Prostate Cancer GradingDr. Fine began by reviewing the historical evolution from the original Gleason scheme to successive updates by the International Society of Urological Pathology (ISUP), including the 2005, 2014, and 2022 refinements. Across these iterations, the most consequential shift has been the progressive narrowing of pattern 3 and reclassification of architectural features once considered low risk.2
These refinements have improved the concordance between histology and prognosis, reducing ambiguity in Grade Group assignment. This evolution coincided with the rise of active surveillance (AS) as a preferred management strategy for low-risk disease, supported by an improved identification of truly indolent cancers.3
A substantial portion of Dr. Fine’s talk focused on quantifying the extent of pattern 4, particularly in Grade Groups 2–4. Using schematic bar diagrams (see below), Dr. Fine illustrated how even small absolute quantities of pattern 4 can meaningfully shift risk classification.4
Examples included:
- GS 3+4=7 with 7% pattern 4 → 10% of total cancer
- GS 4+3=7 with 10% pattern 4 → 70% of total cancer
- GS 4+4=8 with 7% pattern 4 → 100% of total cancer
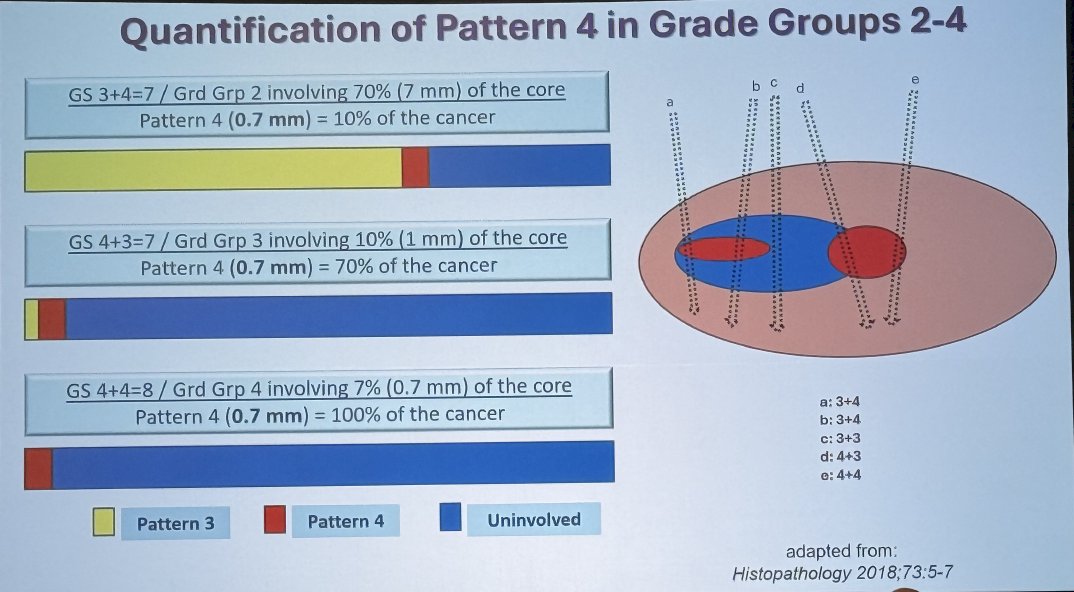
These visual examples underscore the wide biological heterogeneity within identical Grade Groups depending on the absolute burden of pattern 4, a factor increasingly recognized across EAU, NCCN, and AUA guidelines.5
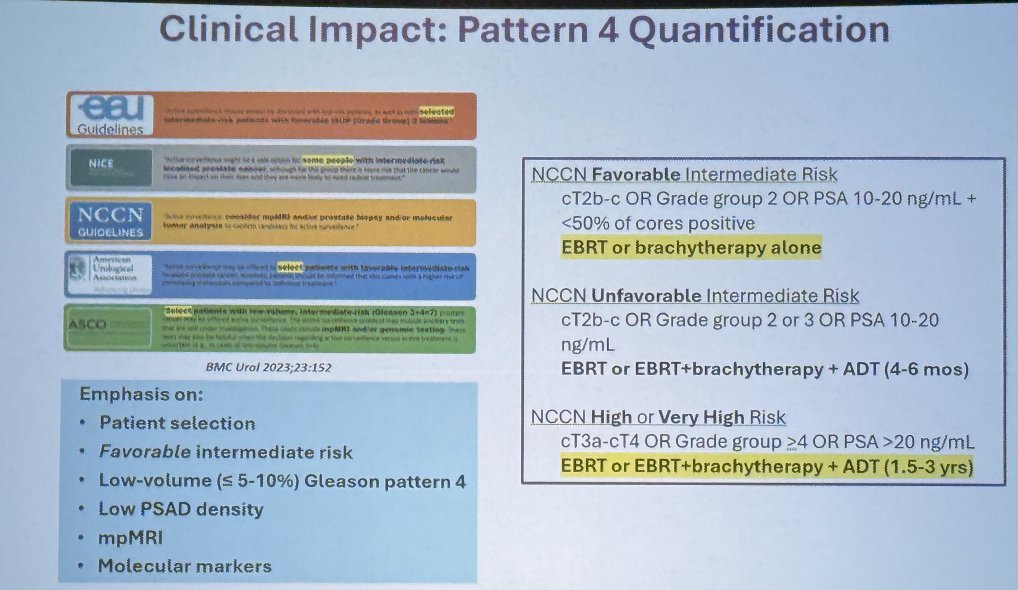
Clinical Impact and Guideline Interpretation
How have major guidelines incorporated Pattern 4 burden into risk stratification?
EAU & NCCN Favorable Intermediate Risk:
- Low-volume (<5–10%) pattern 4
- PSA density considerations
- Integration of mpMRI findings
- Consideration of molecular markers
NCCN Unfavorable Intermediate Risk:
- Grade Group ≥3 or >50% cores positive
- Pattern 4 of higher volume
- Treatment recommendations escalate accordingly (e.g., EBRT ± brachytherapy ± ADT)
Dr. Fine emphasized that pattern 4 quantification increasingly informs treatment intensity, distinguishing “favorable” from “unfavorable” intermediate-risk disease more reliably than Gleason sum alone.
How does discordance between MRI-targeted and systematic sampling affects oncologic outcomes? When systematic biopsy upgrades the Grade Group relative to MRI-targeted biopsy, the risk of adverse pathology increases meaningfully. Conversely, cases where MRI-targeted biopsy shows higher-grade disease may uncover clinically significant patterns (including cribriform morphology) missed by systematic sampling. Overall, when systematic and MRI-targeted biopsy findings are discordant, the risk of adverse outcomes is intermediate.6 This supports an integrated biopsy strategy, particularly for identifying pattern 4 and adverse architectural subtypes.

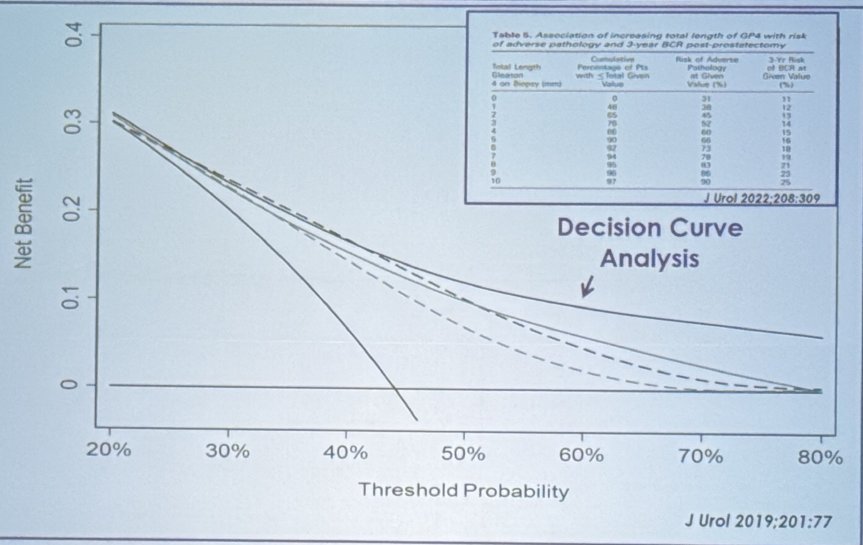
Dr. Fine presented a study of 457 Grade Group 2 (3+4=7) patients, demonstrating that multiple methods of pattern 4 quantification predict adverse pathology:
- Two definitions were used:
- Adverse Pathology Definition 1: Grade Group ≥3, extraprostatic extension (EPE), seminal vesicle invasion (SVI), or lymph node metastasis (LNM)
- Definition 2: ≥Grade Group 4, non-focal EPE, SVI, or LNM
- The key findings were as follows:
- Increased maximum %GP4 per core and overall %GP4 were both associated with higher odds of adverse pathology.
- Multivariable AUC values favored models including total length of GP4, suggesting measurement that incorporates both extent and distribution may provide highest prognostic value.

Decision curve analyses supported the clinical utility of GP4 quantification across threshold probabilities relevant to treatment decisions.
Next, Dr. Fine addressed cribriform morphology.
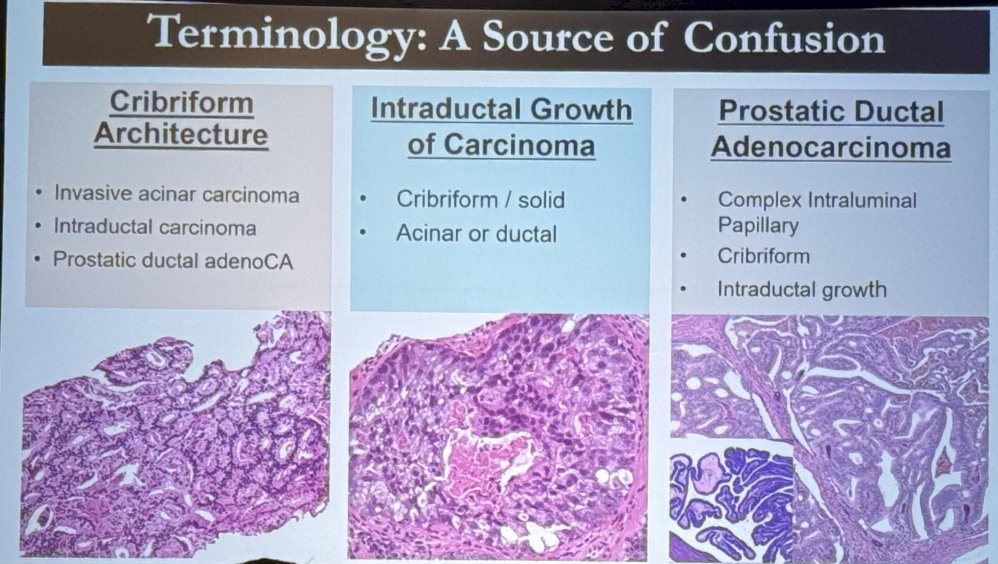
Dr. Fine reviewed three distinct but often conflated entities:7-9
- Cribriform Architecture (invasive acinar carcinoma)
- Intraductal Carcinoma of the Prostate (IDC-P)
- Prostatic Ductal Adenocarcinoma
Though morphologically related, these entities differ in prognosis and genomic instability.
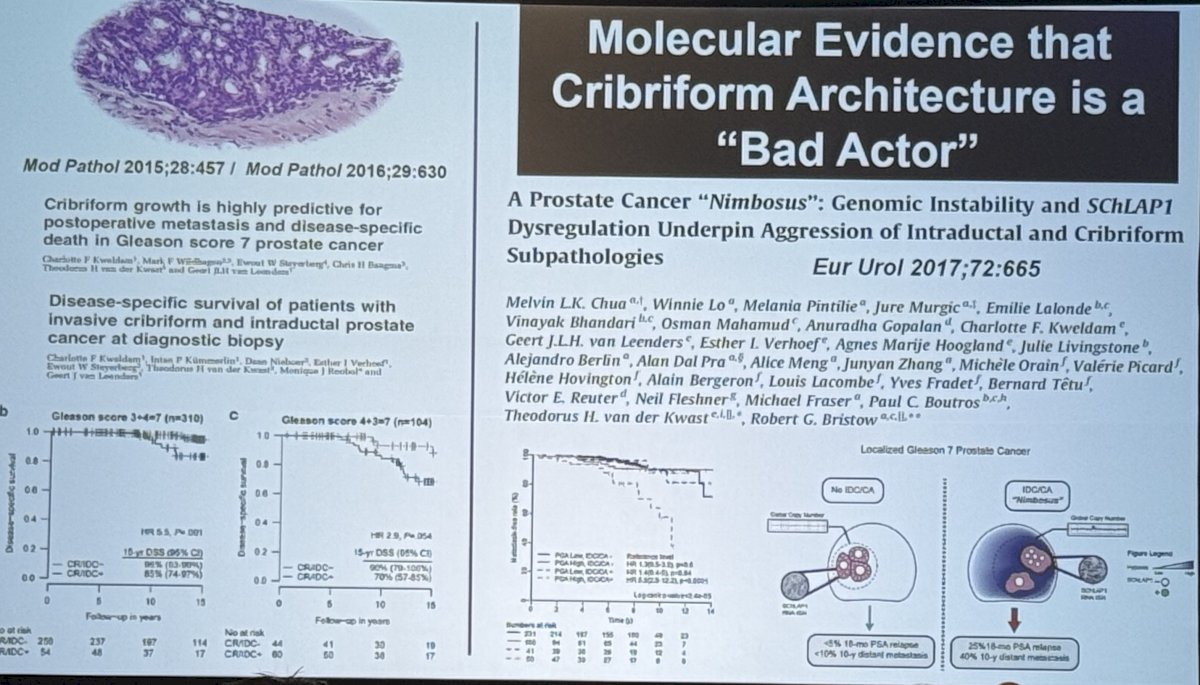
Evidence That Cribriform Architecture Is a “Bad Actor”Several highlighted studies demonstrated:
- Cribriform growth is associated with higher rates of recurrence, metastasis, and prostate cancer–specific mortality.
- Molecular signatures (e.g., MYC, SCHLAP1 dysregulation) support the aggressive biology of cribriform and IDC-P subtypes.
- Presence of large cribriform patterns in Grade Group 2 significantly elevates risk, effectively reclassifying these men into a biologically unfavorable intermediate-risk group.
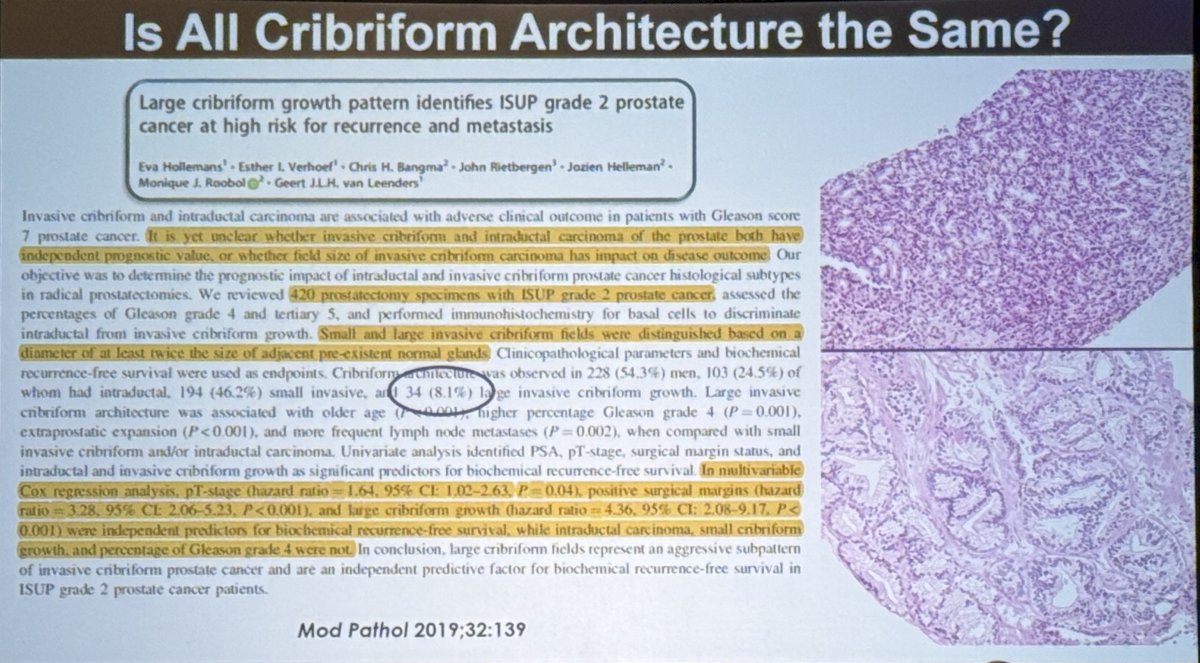
The size and extent of cribriform lesions influence prognosis:
- Large cribriform lesions (≥0.25 mm diameter) carry markedly higher metastatic potential.
- Small, focal cribriform structures confer risk, but not to the same degree.
- Studies cited showed that large cribriform morphology independently predicts metastasis and biochemical recurrence, even when controlling for Grade Group.
These findings suggest that enhancing pathology reporting to indicate cribriform size and extent may enable finer-grained risk stratification.
Dr. Fine presented an analysis of 419 patients after radical prostatectomy, which has led to a proposal of a more nuanced definition of “unfavorable histology.” The suggested components included:
- Gleason pattern 5
- Large cribriform / IDC-P
- Complex intraluminal papillary growth
- Extensive pattern 4
The performance metrics demonstrated the following:
- Biochemical recurrence
- Sensitivity 52%
- Specificity 68%
- Metastatic disease
- Sensitivity 100%
- Specificity 48%
- Prostate cancer–specific mortality
- Sensitivity 100%
- Specificity 46%
The Kaplan-Meier curves below demonstrate clear separation between “unfavorable” and “favorable” histology groups across recurrence, metastasis, and disease-specific survival endpoints.

Dr. Fine concluded with the following take home messages:
- The evolution in prostate cancer grading has narrowed pattern 3 and produced greater attention to high-grade architectural features.
- Pattern 4 quantification and cribriform morphology represent emerging markers that refine risk stratification beyond conventional Grade Groups.
- Future research should integrate advanced markers—including imaging, genomic tools, and machine learning—into the framework of enhanced pathology to improve precision in clinical decision-making.

Presented by: Samson Fine, MD, Attending Pathologist, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
References:
- Epstein JI, Zelefsky MJ, Sjoberg DD, et al. The 2014 ISUP grading system for prostate cancer. Am J Surg Pathol. 2016; 40:244-252.
- Gordetsky J, Epstein JI, Chen YB, et al. Grading of prostate cancer: past, present, and future. Hum Pathol. 2016; 48:87-99.
- Tosoian JJ, Mamawala M, Epstein JI, et al. Active surveillance for prostate cancer: long-term outcomes. J Clin Oncol. 2020; 38:356-363.
- Sauter G, Clauditz T, Krech T, et al. Quantification of pattern 4 predicts outcome in Gleason Grade Group 2. Eur Urol. 2021; 79:31-39.
- Carroll PR, Mohler JL, Beaver JA, et al. NCCN Clinical Practice Guidelines in Oncology: Prostate Cancer. Version 2024–2025.
- Kovac E, Kaffenberger SD, Li J, et al. Risk stratification by MRI-targeted vs systematic biopsy. Cancer. 2023; 129:2150-2160.
- van Leenders GJLH, van der Kwast TH, Grignon DJ, et al. Cribriform architecture and survival in prostate cancer. Mod Pathol. 2018; 31:778-785.
- Hollemans E, Verhoef EI, Bangma CH, et al. Large cribriform growth and IDC-P predict metastasis. J Pathol. 2019; 248:98-106.
- Risbridger GP, Taylor RA, Clouston D, et al. Genomic instability in cribriform and IDC-P prostate cancer. Nat Rev Urol. 2022; 19:133-150.
- Egevad L, Kristiansen G, Kweldam CF, et al. Composite histologic models for adverse pathology. Histopathology. 2024; 85:421-432.