(UroToday.com) The 2025 SUO Annual Meeting featured a State-of-the-Art lecture by Dr. Tudor Borza addressing how contemporary practice patterns, evidence, and diagnostic innovations have led to a dramatic reduction in the overtreatment of low-risk prostate cancer. Drawing largely from the Michigan Urological Surgery Improvement Collaborative (MUSIC) experience and national datasets, he highlighted how active surveillance (AS) has evolved into the preferred strategy for Grade Group 1 disease, supported by robust evidence and safer, more reliable diagnostic tools.¹
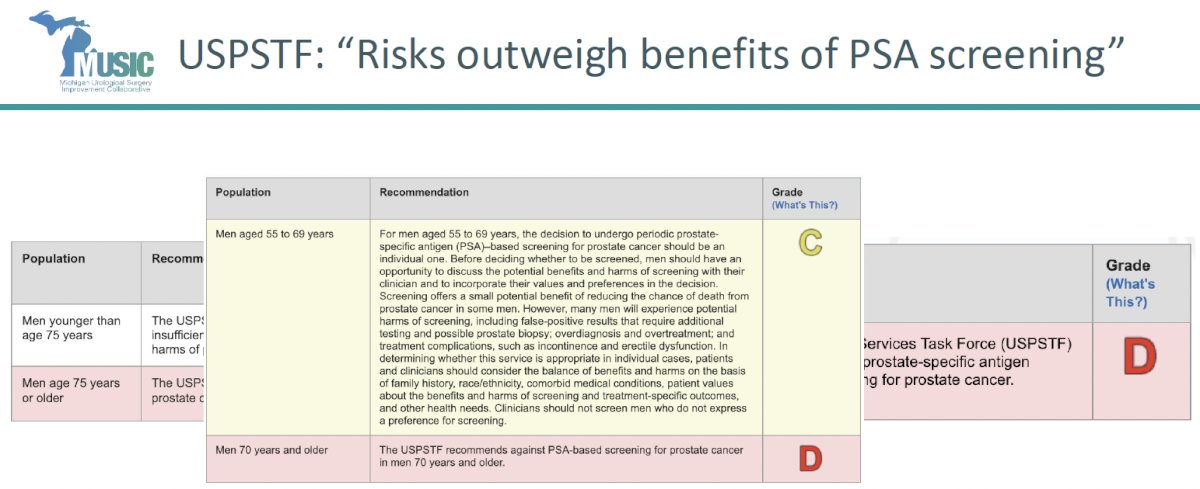
Turning Point: Addressing Overdiagnosis Without OvertreatmentHistorically, PSA screening faced criticism for detecting many indolent cancers that would never threaten life—leading to unnecessary surgery, radiation, and treatment-related morbidity. The 2012 USPSTF “D” recommendation against PSA testing crystallized the problem and temporarily reduced screening rates.² This shift emphasized the need to separate diagnosis from treatment.
Active surveillance emerged as the modern solution to this dilemma. Contemporary AS involves structured PSA monitoring, MRI, confirmatory biopsy, and predefined criteria for intervention—providing a safe means of avoiding overtreatment in appropriately selected men.
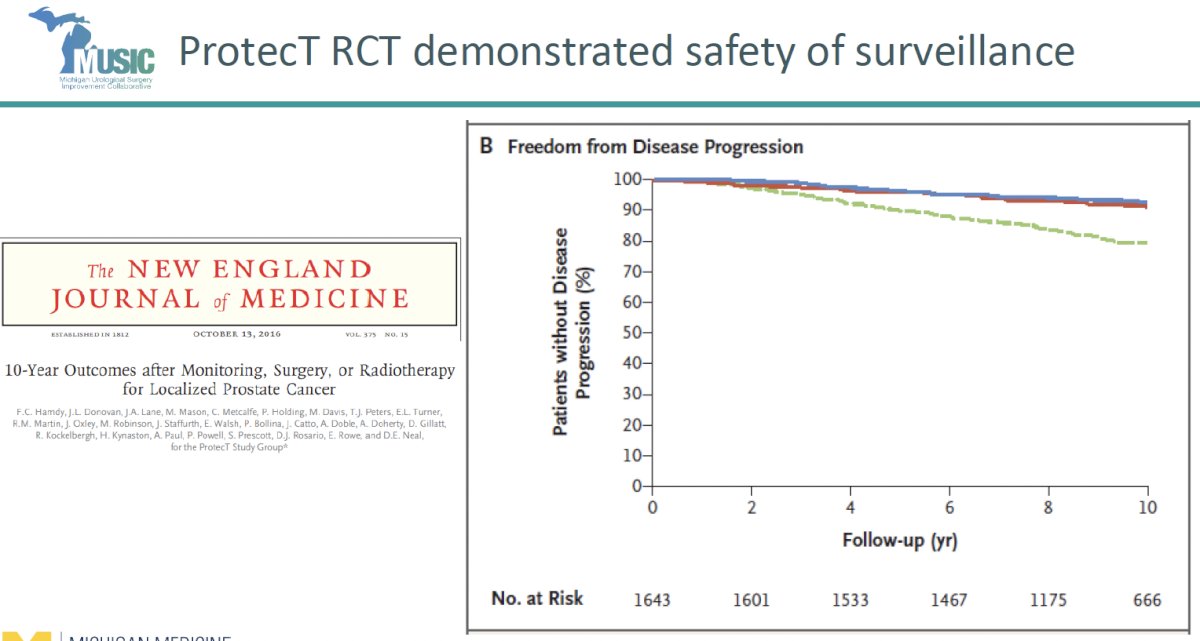
Dr. Borza reviewed data from the landmark ProtecT randomized trial, which followed men with localized prostate cancer for more than a decade.³ This trial demonstrated that:
- Prostate cancer–specific mortality at 10 years was low (≈1%) and similar across surgery, radiotherapy, and active monitoring.
- Although progression and metastases were more common with active monitoring, this did not translate into increased mortality.
- Long-term survival outcomes remain virtually superimposable across treatment arms, providing the strongest evidence base supporting AS for low-risk disease.
Active Surveillance Adoption and Safety
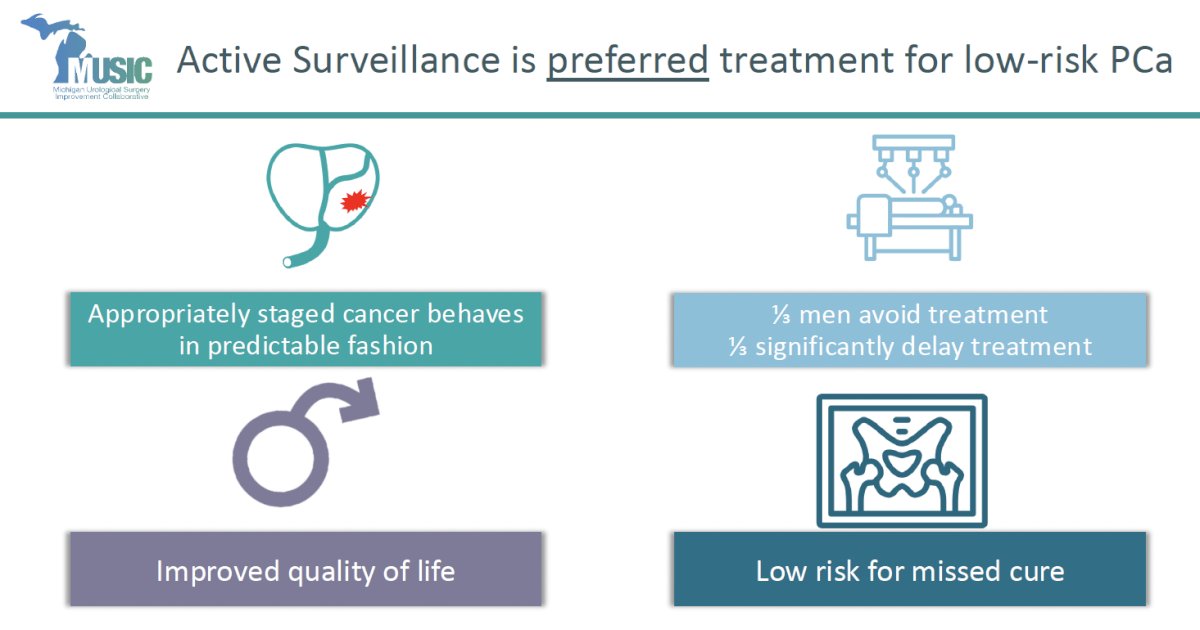
AS is now the preferred management strategy for GG1 prostate cancer, supported by numerous prospective and retrospective cohorts.⁴⁻⁶ These studies consistently show:
- ~1/3 of men avoid definitive treatment entirely
- Another ~1/3 significantly defer treatment
- Quality-of-life outcomes are superior compared to immediate therapy
- Risk of missing a curative window remains low
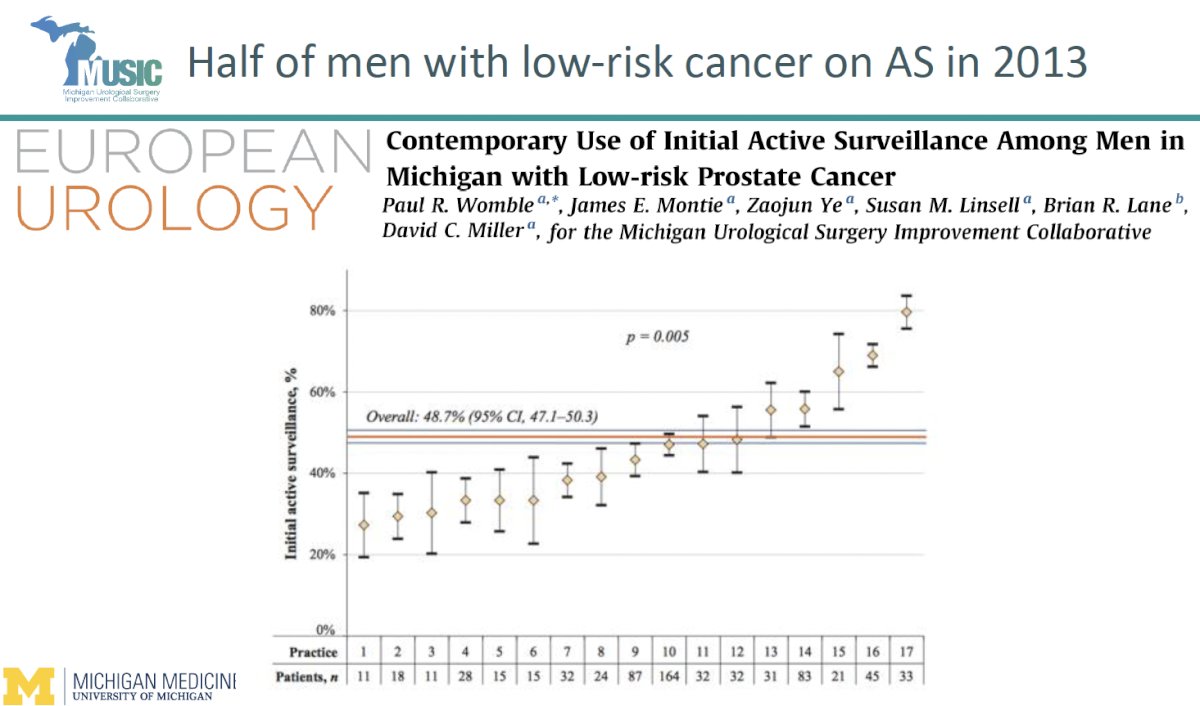
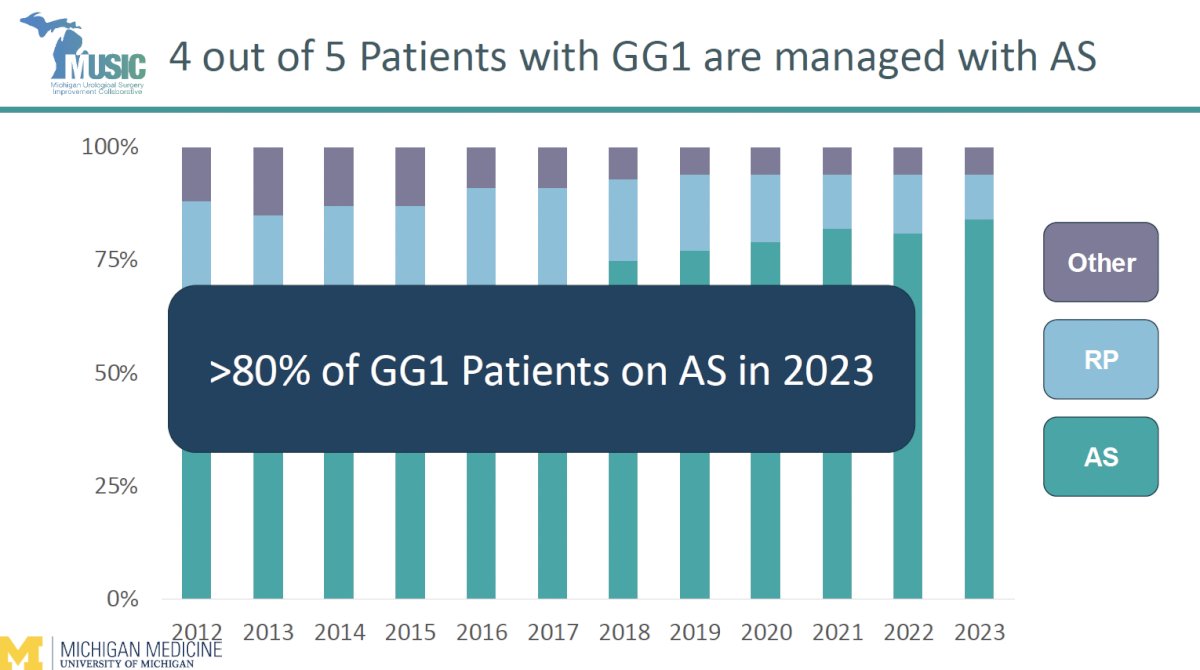
MUSIC data show that AS utilization for low-risk disease rose from ~50% in 2013 to >80% in 2023, one of the highest adoption rates worldwide.¹
National AQUA registry data demonstrate a parallel decline in surgery and radiation for GG1 disease.¹
Dr. Borza emphasized that increased AS adoption is driven not only by evidence but by improved tools for more accurate disease characterization:
- Multiparametric MRI and MRI-Targeted Biopsy
- Conventional TRUS biopsy detects cancer in ~30% of men.
- MRI-targeted biopsy increases detection of clinically significant lesions to ~60%, particularly in anterior and transition zones.⁷
- Genomic Classifiers
- Tests such as Decipher, Prolaris, and Oncotype DX provide insights into tumor biology and prognosis.
- While their impact on decision-making varies, they help reinforce confidence that a man truly has a low-risk disease.⁸
- PSMA PET
- Emerging evidence supports its utility in detecting clinically significant lesions and refining baseline staging to reduce misclassification.⁹
These tools allow clinicians to better identify men who can safely remain on AS and decrease uncertainty around underdiagnosis.
Durability of Active SurveillanceUpdated MUSIC AS data illustrate excellent long-term durability:¹
- 9.3% treated at 1 year
- 16% treated at 2 years
- 24% treated at 5 years
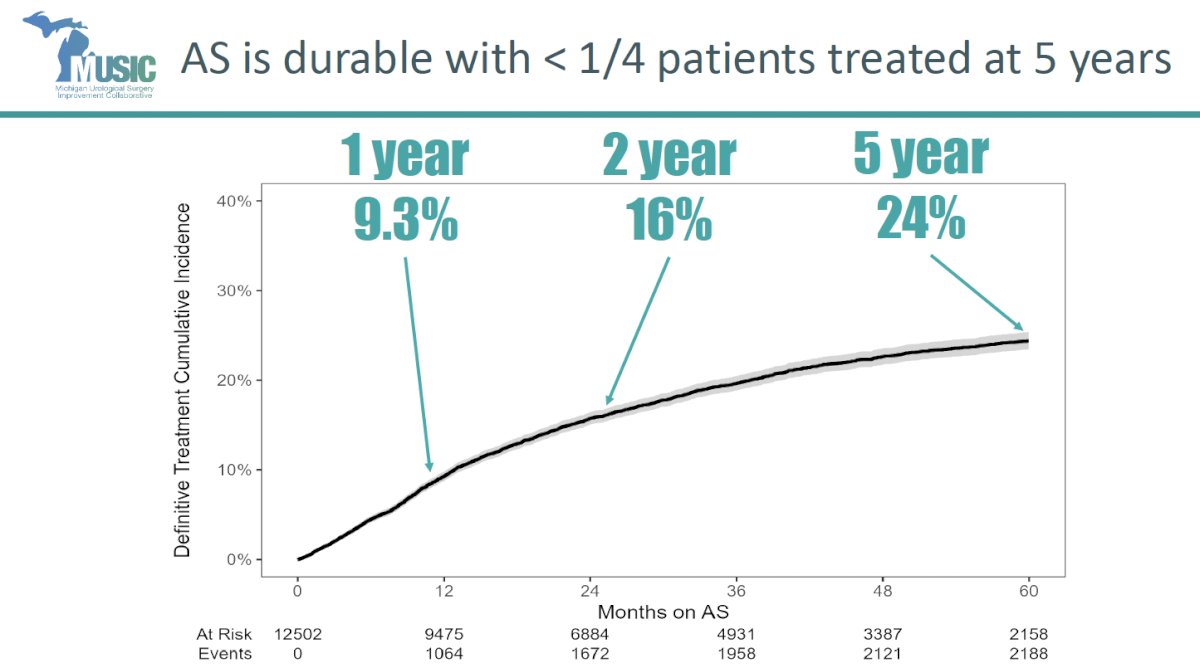
Most transitions to treatment reflect appropriate triggers (grade progression, rising PSA density, MRI changes), underscoring the safety and effectiveness of structured AS protocols.
Radical Prostatectomy for GG1 Disease: Nearly EliminatedIn modern practice, overtreatment of true GG1 disease is extremely uncommon:
- In SEER, <8% of prostatectomies are performed for GG1 cancers.¹⁰
- In MUSIC, <3% of surgical pathology reveals GG1 disease.¹
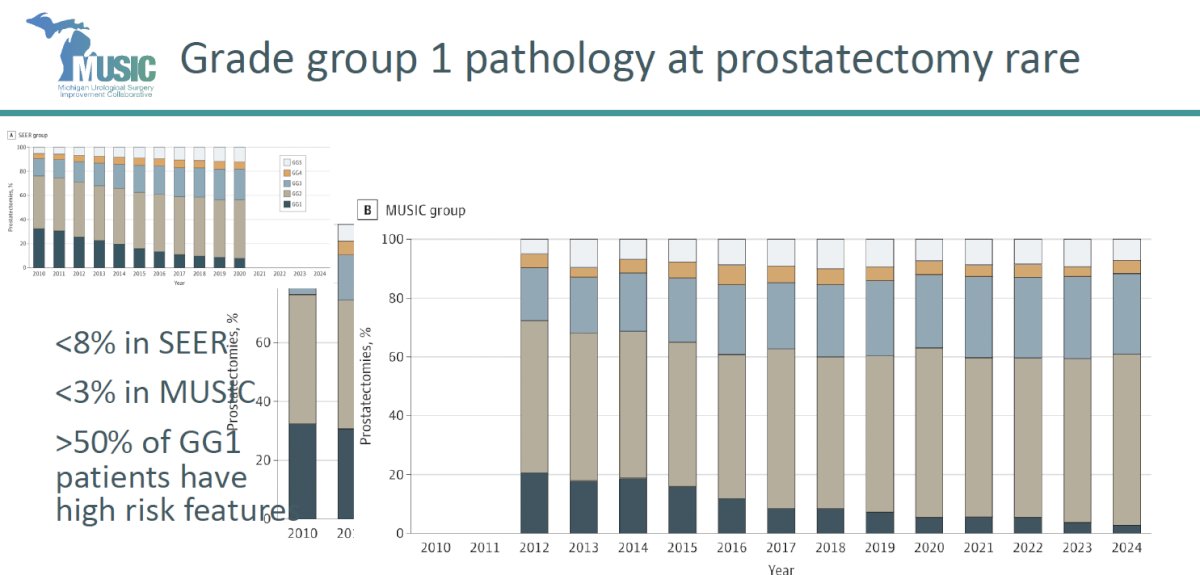
Notably, more than half of men clinically diagnosed with GG1 who undergo prostatectomy harbor higher-grade disease on final pathology, meaning truly indolent cancers seldom reach surgery at all.
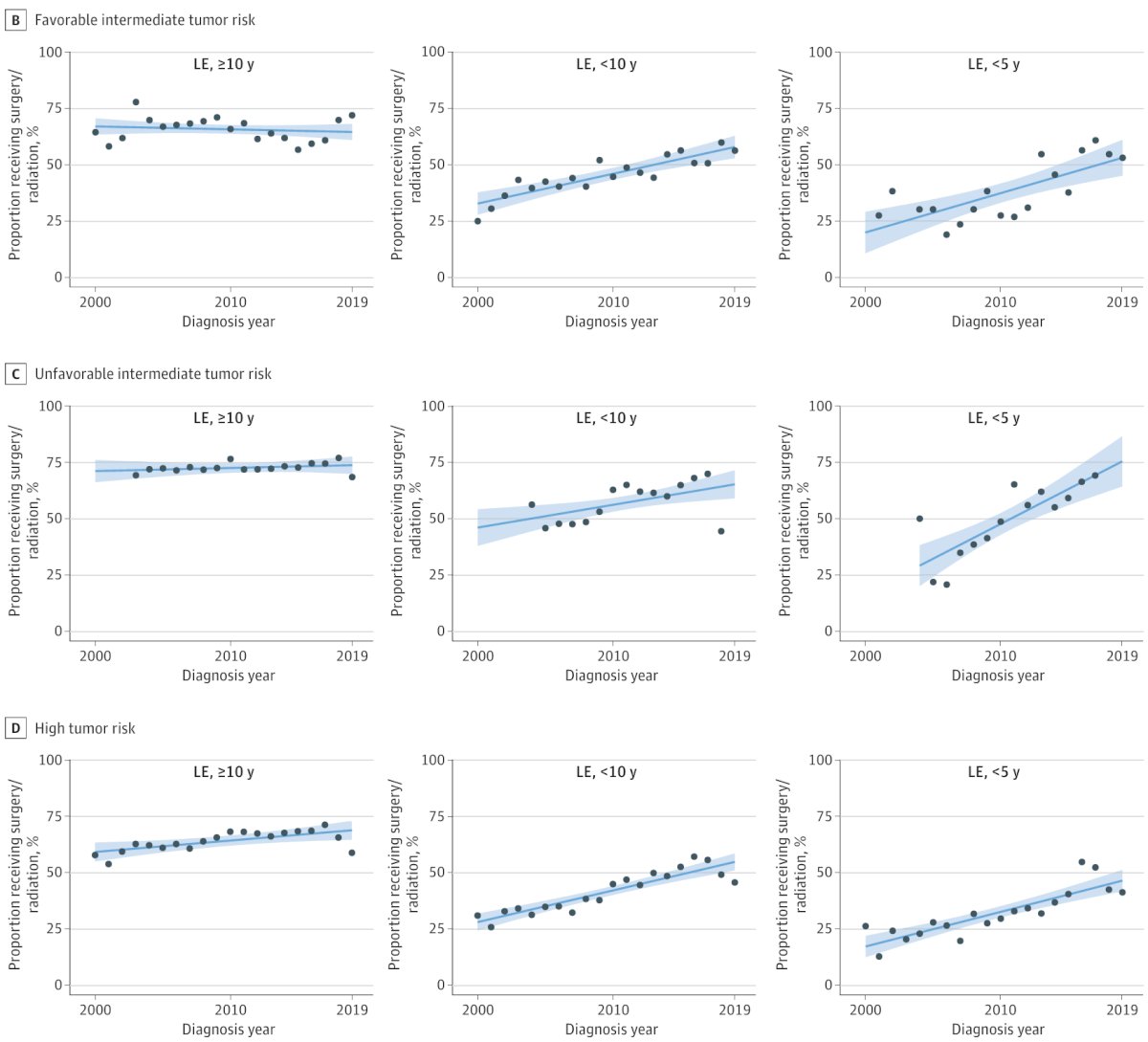
Emerging Problem: Overtreatment of Intermediate/High-Risk Disease in Men with Limited Life Expectancy
While overtreatment of low-risk disease has declined, Dr. Borza emphasized growing concern about potential overtreatment in older men with intermediate- or high-risk disease.
Data from Daskivich et al. demonstrate high rates of radiation and surgery even in men with 5-year life expectancy and 5–10-year life expectancy, where treatment benefit is uncertain, and toxicity risk is high.¹¹ This represents a major target for next-generation de-implementation efforts.
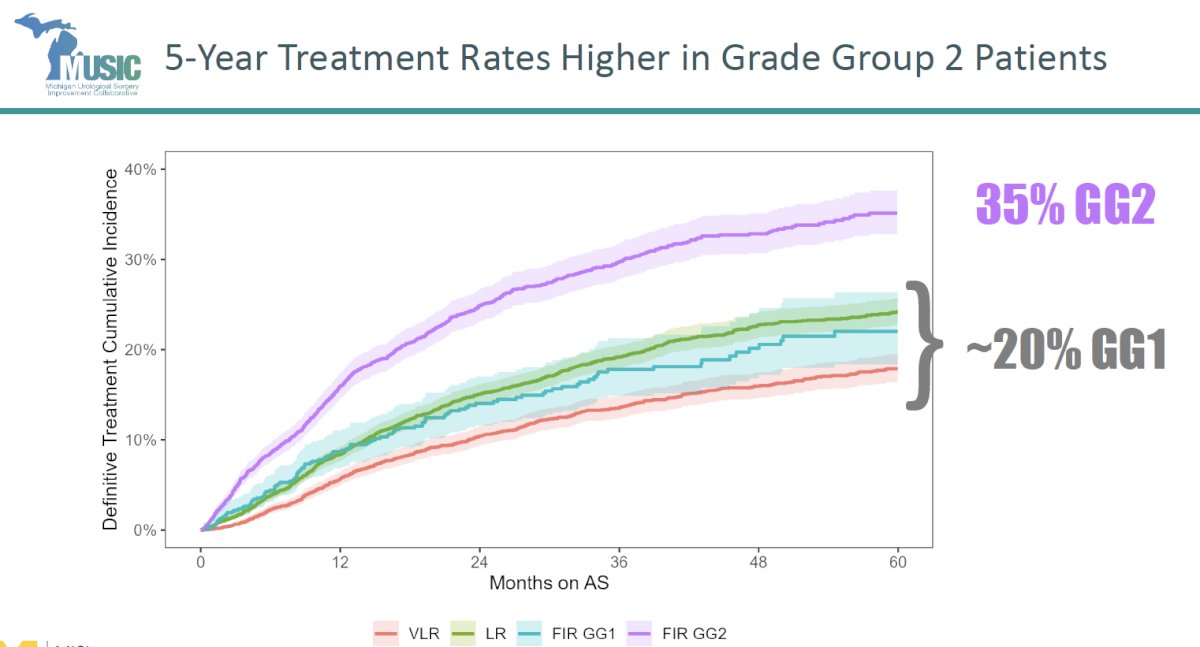
MUSIC data show that GG2 patients transition to treatment earlier and more frequently than GG1:¹
- 20% of GG1 patients treated by 5 years
- 35% of GG2 patients treated by 5 years
This reflects appropriate vigilance but also underscores the need for better characterization of which GG2 patients can safely remain on AS.
Dr. Borza’s take-home messages were as follows:
- Active surveillance can uncouple overdiagnosis from overtreatment
- Urologist adoption of AS continues to increase for men with low-risk PCa
- MUSIC rates >80%
- Improved risk stratification contributing to ‘durable’ use of AS
- Radical prostatectomy for Grade Group 1 prostate cancer is rare
- Overtreatment in low-risk patients is extremely rare nowadays
- Overtreatment amongst men with a limited life expectancy presents an ongoing opportunity for improvement
Presented by: Tudor Borza, MD, MS, Assistant Professor, Department of Urology, University of Michigan, Ann Arbor, MI
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, December 2nd–5th, 2025
References- Auffenberg GB, Ghani KR, Ramani S, et al. Active surveillance use among men with low-risk prostate cancer in the Michigan Urological Surgery Improvement Collaborative. J Urol. 2021;205(2):441-449.
- Moyer VA. Screening for prostate cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157(2):120-134.
- Hamdy FC, Donovan JL, Lane JA, et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer (ProtecT). N Engl J Med. 2016;375:1415-1424.
- Klotz L, Vesprini D, Sethukavalan P, et al. Long-term follow-up of active surveillance for localized prostate cancer. J Clin Oncol. 2015;33:272-277.
- Welty CJ, Cowan JE, Nguyen H, et al. Extended follow-up and risk factors for disease reclassification in active surveillance of prostate cancer. Eur Urol. 2015;68:1028-1034.
- Loeb S, Bruinsma SM, Nicholson J, et al. Active surveillance for prostate cancer: a systematic review. Eur Urol. 2015;67:619-626.
- Kasivisvanathan V, Rannikko AS, Borghi M, et al. MRI-targeted vs standard biopsy for the diagnosis of prostate cancer (PRECISION). N Engl J Med. 2018;378:1767-1777.
- Cullen J, Rosner IL, Brand TC, et al. A biopsy-based 17-gene genomic prostate score predicts metastasis and prostate cancer–specific mortality. BJU Int. 2015;116:258-267.
- Fendler WP, Calais J, Eiber M, et al. Assessment of 68Ga-PSMA PET for primary staging of prostate cancer. JAMA Oncol. 2019;5:856-863.
- Mahal BA, Butler S, Franco I, et al. Use of radical prostatectomy for low-risk prostate cancer in the United States. JAMA Surg. 2019;154:946-953.
- Daskivich TJ, Fan KH, Koyama T, et al. Effect of age, tumor risk, and comorbidity on competing risks for survival in localized prostate cancer. JAMA Intern Med. 2013;173:1318-1325.