(UroToday.com) The 2025 SUO annual meeting featured a prostate cancer session and a presentation by Dr. Jack Andrews discussing a secondary analysis of the RAVENS trial assessing pre-radiotherapy tumor extracellular vesicles for risk stratification in oligorecurrent prostate cancer. The role of stereotactic ablative body radiotherapy, metastasis-directed therapy for metachronous oligometastatic prostate cancer, remains uncertain. While the STOMP1 and ORIOLE2 trials suggested an oncologic benefit, a definitive survival advantage is still unclear.
Looking deeper at the data, it appears that some patients demonstrate long, durable responses, and their responses are diluted within the whole cohort. Dr. Andrews and colleagues recently published data demonstrating PSMA+ extracellular vesicles were both prognostic and predictive biomarkers of response in this setting.3 Using biomarkers to select the appropriate patients for metastasis-directed therapy may help personalize care and increase the likelihood of positive clinical trials. The RAVENS trial4 from Johns Hopkins looked at stereotactic ablative body radiotherapy versus stereotactic ablative body radiotherapy + radium-223 in metachronous oligometastatic prostate cancer. In this analysis, Dr. Andrews and colleagues obtained the plasma samples from the RAVENS trial and sought to validate the performance of PSMA+ extracellular vesicles as a prognostic biomarker.
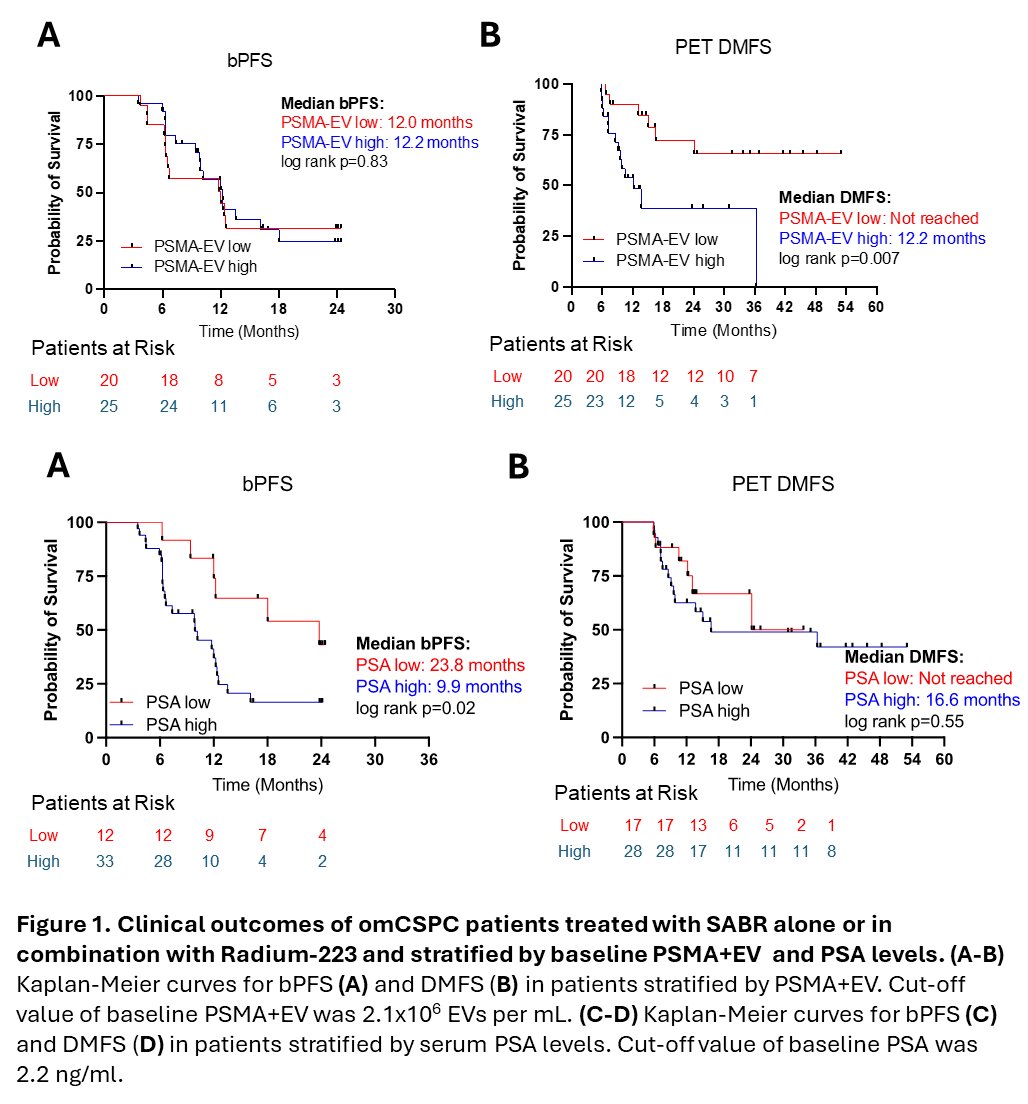
Platelet-poor plasma was obtained pre-treatment from 45 patients with oligometastatic castration-sensitive prostate cancer enrolled in the RAVENS trial. Twenty-five patients received stereotactic ablative body radiotherapy only, and 20 patients received stereotactic ablative body radiotherapy + radium-223. Biochemical progression-free survival and distant metastasis-free survival were used as clinical endpoints to determine the association of PSMA+ extracellular vesicles and serum PSA with oncological outcomes. Per RAVENS protocol, biochemical progression-free survival was defined as a ≥ 25% increase in PSA from nadir (and absolute increase to ≥ 2 ng/ml), requiring confirmation at≥ 4 weeks later. Distant metastasis-free survival was defined as new metastases visualized on molecular PET imaging and lesions needed to have a clear correlate on the CT portion (for soft tissue and nodal disease, meeting size criteria per RECIST 1.1, and for bone lesions, having a clear sclerotic/lytic component). Kaplan-Meier estimates were used to estimate survival curves.
Baseline PSMA- and STEAP1-positive extracellular vesicles and PSA were quantified in 45 oligometastatic castration-sensitive prostate cancer patients receiving stereotactic ablative body radiotherapy ± radium-223. Kaplan–Meier analysis showed no PSMA-extracellular vesicles effect on biochemical progression-free survival (biochemical progression-free survival: 12.0 versus 12.2 months, p = 0.83) but a marked impact on distant metastasis-free survival (not reached versus 12.2 months, p = 0.007). High PSA shortened biochemical progression-free survival (9.9 versus 23.8 months, p = 0.02) without altering distant metastases-free survival. Cox models confirmed these patterns: PSA ≤ 2.2 ng ml-1 reduces risk of biochemical recurrence (HR 3.24, 95 % CI 1.31–9.76, p = 0.019), whereas low PSMA- extracellular vesicles (≤2.1 × 106 extracellular vesicles ml-1 HR 3.70, 1.41–10.78, p = 0.01) and STEAP1- extracellular vesicles (≤4.0 × 107 extracellular vesicles ml-1 HR 5.67, 2.01–17.21, p = 0.001) decreased risk of distant metastases:
Dr. Andrews concluded his presentation discussing a secondary analysis of the RAVENS trial assessing pre-radiotherapy tumor extracellular vesicles for risk stratification in oligorecurrent prostate cancer with the following take-home points:
- In this analysis, the previously published high/low cutpoint for PSMA+ extracellular vesicles was prognostic for PSMA PET distant metastasis-free survival; however was not predictive of biochemical progression
- PSA was prognostic for biochemical progression, but was not predictive for PSMA PET distant metastasis-free survival
- These results highlight the potential need for PSA and PSMA+ extracellular vesicles as paired biomarkers, similar to results seen in the STOMP and ORIOLE trial analysis
- There is currently an active phase 2 stereotactic ablative body radiotherapy trial with PSMA+ extracellular vesicles to further validate this biomarker
Presented by: Jack Andrews, MD, Urologic Oncologist, Senior Associate Consultant, Department of Urology, Mayo Clinic Arizona, Scottsdale, AZ
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, Wed, Dec 3 – Fri, Dec 5, 2025.
References:
- Ost P, Reynders D, Decaestecker K, et al. Surveillance of metastasis-directed therapy for oligometastatic cancer recurrence: A prospective, randomized, multicenter phase II trial. J Clin Oncol. 2018 Feb 10;36(5):446-453.
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol 2020 Mar 26;6(5):650-659.
- Andrews JR, Kim Y, Horjeti E, et al. PSMA+ extracellular vesicles are a biomarker for SABR in oligorecurrent prostate cancer: Analysis from the STOMP-like and ORIOLE trial cohorts. Clin Cancer Res. 2025 Mar 17;31(6):1142-1149.
- Wang JH, Sherry AD, Bazyar S, et al. Outcomes of Radium-223 and Stereotactic Ablative Radiotherapy versus Stereotactic Ablative Radiotherapy for Oligometastatic Prostate Cancers: The RAVENS Phase II Randomized Trial. J Clin Oncol. 2025 Jun 20;43(18):2059-2068.