(UroToday.com) The 2025 SUO Annual Meeting featured a prostate cancer poster session in which Dr. Jason Goodloe presented an analysis evaluating how race and community-level social vulnerability influence risk-based prostate cancer treatment patterns and metastasis-free survival in community settings.
The impact of local community vulnerability on the implementation of clinical risk-based prostate cancer care—particularly for Black men, who are disproportionately affected—remains poorly understood. This study aimed to examine whether race and social vulnerability were associated with differences in guideline-concordant treatment (GCT) and downstream metastasis-free survival (MFS).
This observational study used CaPSURE data from men diagnosed with prostate cancer between 1998 and 2022. The cohort included individuals with biopsy-proven, clinically localized prostate cancer treated in 38 community urology practices, academic centers, and VA hospitals.
The key exposures were:
- Race: Black versus non-Black
- Community-level Social Vulnerability Index (SVI): Multicomponent Census-tract metric; ≥75th percentile defined as “high”
- Guideline-concordant treatment:
- For intermediate/high-risk prostate cancer: Radical prostatectomy (RP) with radiation therapy (RT) as indicated, or Primary Radiation Therapy
- For low-risk prostate cancer: Active Surveillance / Watchful Waiting (AS/WW)
Multivariable logistic regression models assessed the associations between guideline-concordant treatment and race, SVI, and the interaction between race and SVI. Cox proportional hazards models evaluated associations between GCT and MFS among intermediate/high-risk patients. All models were adjusted for year of diagnosis, education, annual income, insurance status, comorbidities, and job status.
This study included 8,841 men with localized prostate cancer. 10% were black. 36% had low-risk disease. 12% lived in high SVI communities.
The treatment patterns were as follows:
- Overall management:
- 52% managed with radical prostatectomy
- 26% with radiation therapy
- 9% with AS/WW
- 13% with primary ADT
- Risk groups managed by primary ADT:
- 12.5% of low-risk PCa
- 12.1% of intermediate-risk PCa
- 34% of high-risk PCa
Intermediate/high-risk patients who received guideline-concordant treatment had superior MFS outcomes, as demonstrated below:
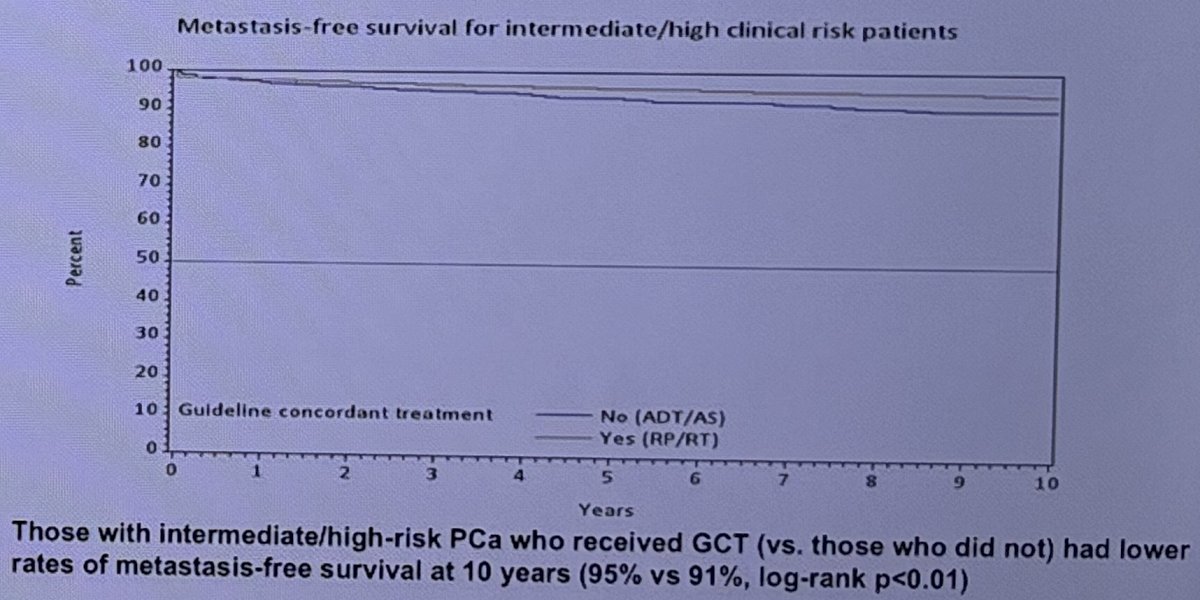
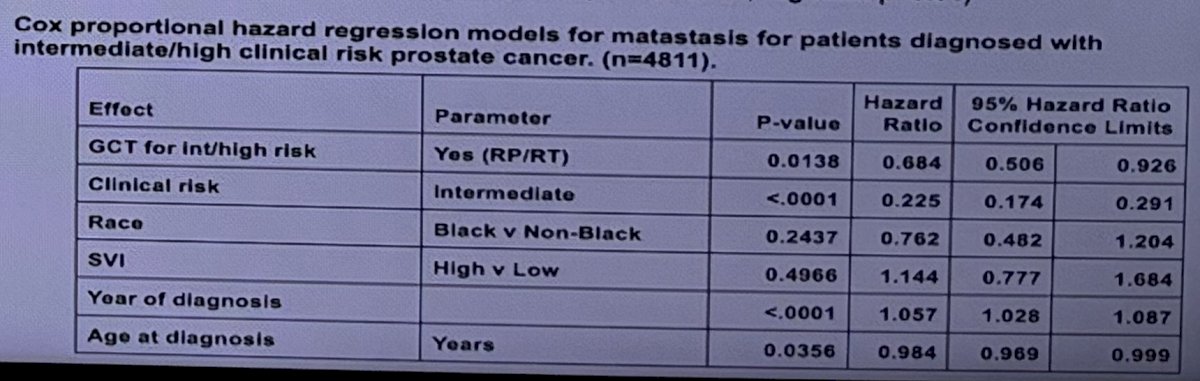
This is further demonstrated in the multivariable model below which demonstrates that intermediate/high risk patients receiving guideline-concordant treatment had a 32% lower rate of metastases (HR: 0.68, p=0.014).
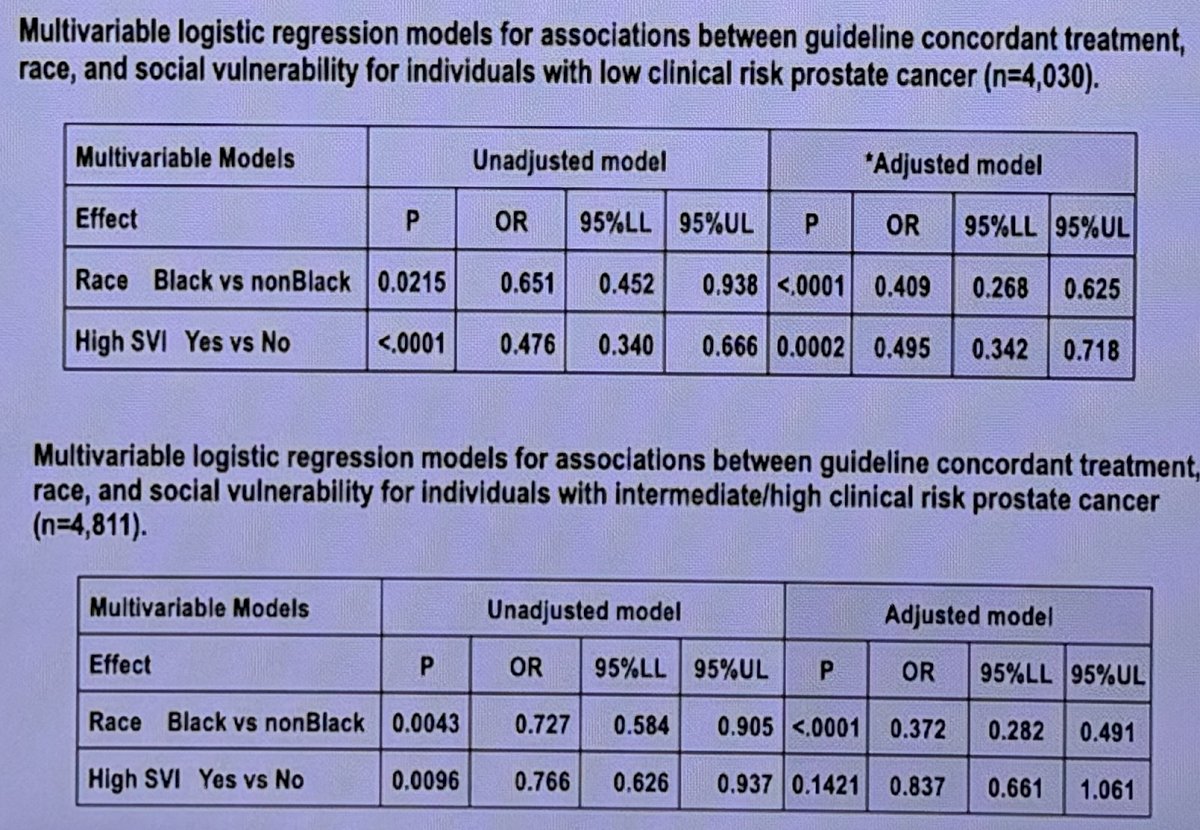
Black patients were less likely to receive guideline-concordant treatment, irrespective of disease risk (low-risk: OR=0.41, p<0.001; intermediate/high risk: OR=0.37, p<0.0001). Low-risk patients with a high SVI were less likely to receive guideline-concordant treatment (OR: 0.50, p=0.0002), but those with a high SVI and intermediate/high-risk disease were not significantly less likely to receive guideline-concordant treatment (p=0.14).
Dr. Goodloe concluded as follows:
- Black race and high SVI influenced receipt of guideline-concordant treatment, with associations that changed after accounting for disease risk.
- Guideline-concordant treatment for prostate cancer was associated with decreased metastasis risk, particularly for intermediate/high-risk patients.
- These findings highlight opportunities for improving equitable implementation of risk-based care in community settings, especially for Black men and those living in socially vulnerable communities.
Presented by: Jason L. Goodloe, MD, Clinical Research Coordinator and Researcher at University of California, San Francisco, CA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.