(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting was host to the annual European Association of Urology (EAU) lecture. Dr. Alessandro Volpe delivered a comprehensive review of the 20-year evolution of active surveillance (AS) for small renal masses (SRMs), charting how the field moved from anecdotal observations to structured, evidence-based management grounded in prospective data, refined risk stratification, and a deepened biological understanding of SRM heterogeneity. His talk underscored that active surveillance is not a passive or inferior alternative to intervention, but rather a deliberately monitored oncologic strategy tailored to the natural history of small renal tumors.
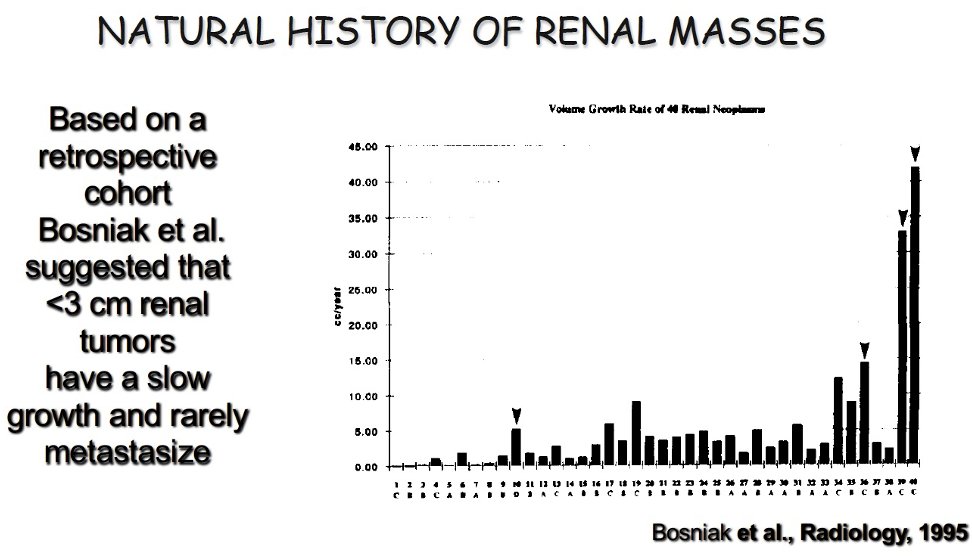
He opened by highlighting the epidemiologic shift that sparked interest in surveillance: the dramatic rise in incidentally detected renal tumors over the last 25 years, largely attributable to increased abdominal imaging. The majority of these tumors are ≤4 cm, often asymptomatic, and exhibit wide biological variability. Early radiologic and autopsy studies revealed that a substantial proportion of small renal lesions were histologically benign or indolent. Bosniak and colleagues evaluated the longitudinal behavior of small enhancing renal masses and demonstrated minimal growth over time, with many masses exhibiting growth <0.3 cm per year and exceedingly low rates of metastasis. Their observations established the initial hypothesis that tumor biology—rather than tumor presence alone—should guide management.1
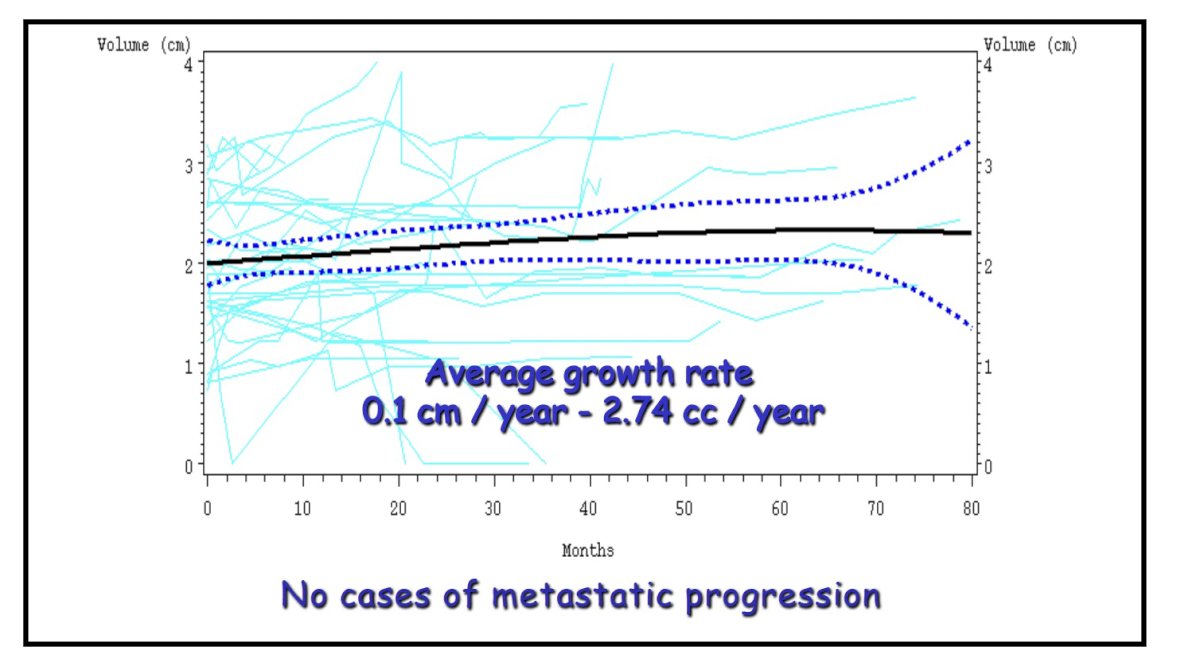
A major inflection point came with the prospective work by Volpe, Jewett, and colleagues at the University of Toronto, who enrolled 32 patients with incidentally detected SRMs and followed them closely with serial imaging.2 Median follow-up was 36 months, during which the median linear growth rate was only 0.1 cm per year, and more than one-third of tumors demonstrated zero measurable growth. This study was also the first to report volumetric growth, averaging 2.7 cm³ per year, reinforcing that changes in volume often remain clinically insignificant. Importantly, no patient developed metastases. These early findings laid the intellectual foundation for AS by demonstrating that immediate surgery was not mandatory for all SRMs.
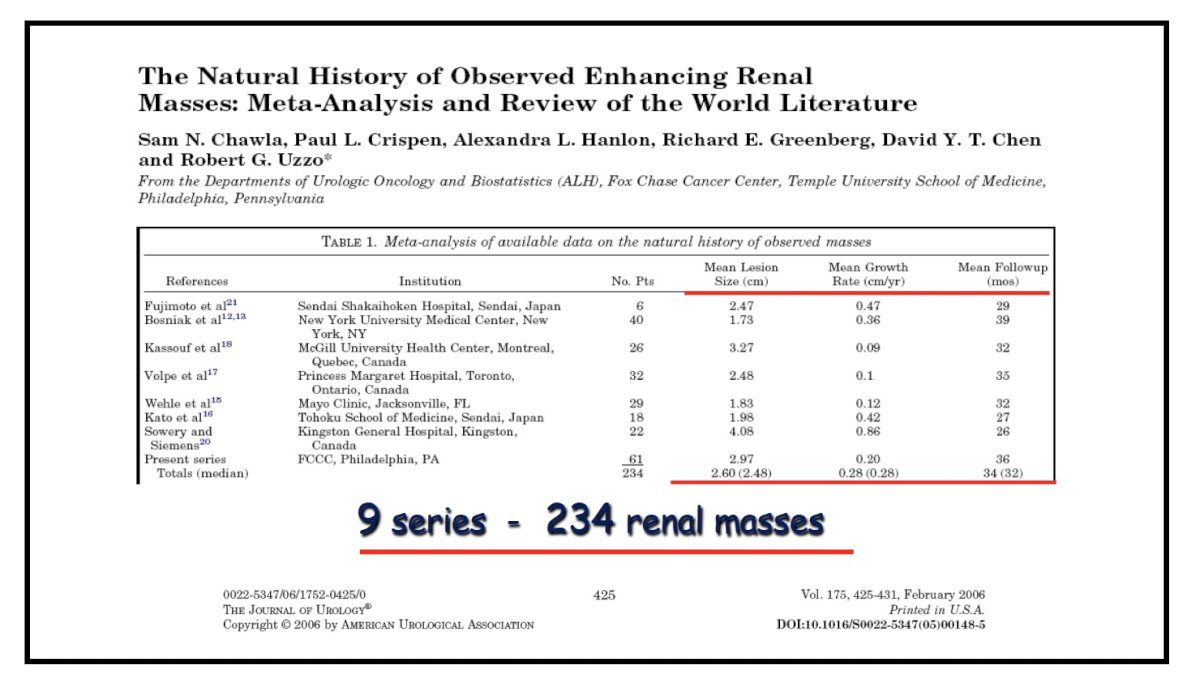
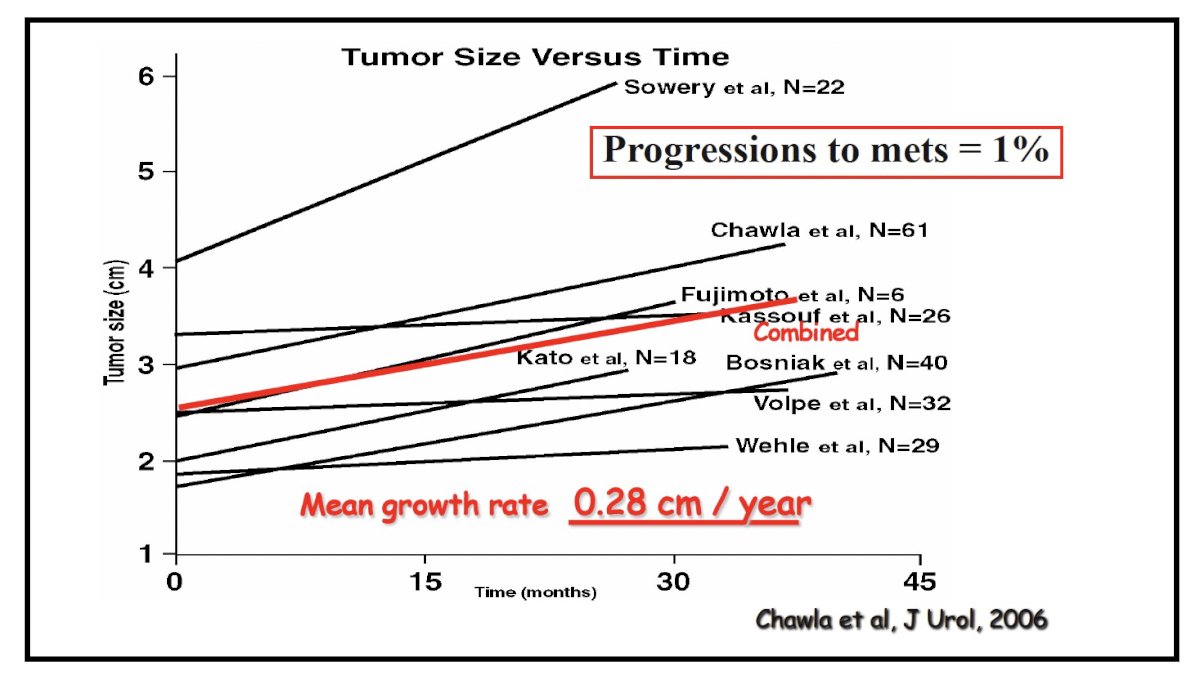
Chawla et al. expanded the evidence base with a meta-analysis of 234 SRMs drawn from nine institutional cohorts.3 Across studies, the median linear growth ranged from 0.1 to 0.7 cm per year, with a pooled estimate of 0.28 cm per year. The metastatic progression rate was remarkably low at 1%. This work powerfully reinforced that the overwhelming majority of SRMs exhibit indolent behavior and that metastatic progression during AS is rare.
Smaldone and colleagues performed one of the most granular evaluations of metastatic progressors, comparing 18 patients who developed metastasis during AS to 318 who did not.4 Progressors were significantly older (75 vs 67 years), had larger tumors at diagnosis (3.2 vs 2.3 cm), and displayed substantially faster growth kinetics (0.8 vs 0.3 cm/year). These findings introduced the concept that biologic momentum—the combination of baseline size, age, and especially growth rate—better predicts meaningful oncologic risk than static measures alone. Their work helped operationalize the modern surveillance triggers used worldwide.
To validate the feasibility of AS in broader practice settings, the Canadian multi-center prospective study enrolled 209 patients across multiple institutions.2 The baseline tumor size averaged 2.1 cm, and the median follow-up was 28 months. The mean annual growth was only 0.13 cm, consistent with earlier reports. Renal mass biopsy was performed in nearly half the cohort, with a diagnostic yield of 67 percent. Among diagnostic biopsies, 82 percent confirmed RCC. Despite this high prevalence of malignancy, no patient developed metastasis except one, underscoring that histology alone cannot reliably predict aggressiveness and must be interpreted alongside longitudinal imaging behavior. This study was pivotal in demonstrating that AS is feasible not only in specialized academic centers but also across diverse, real-world environments.

The largest and most influential dataset in this field is the DISSRM (Delayed Intervention and Surveillance for Small Renal Masses) registry.5
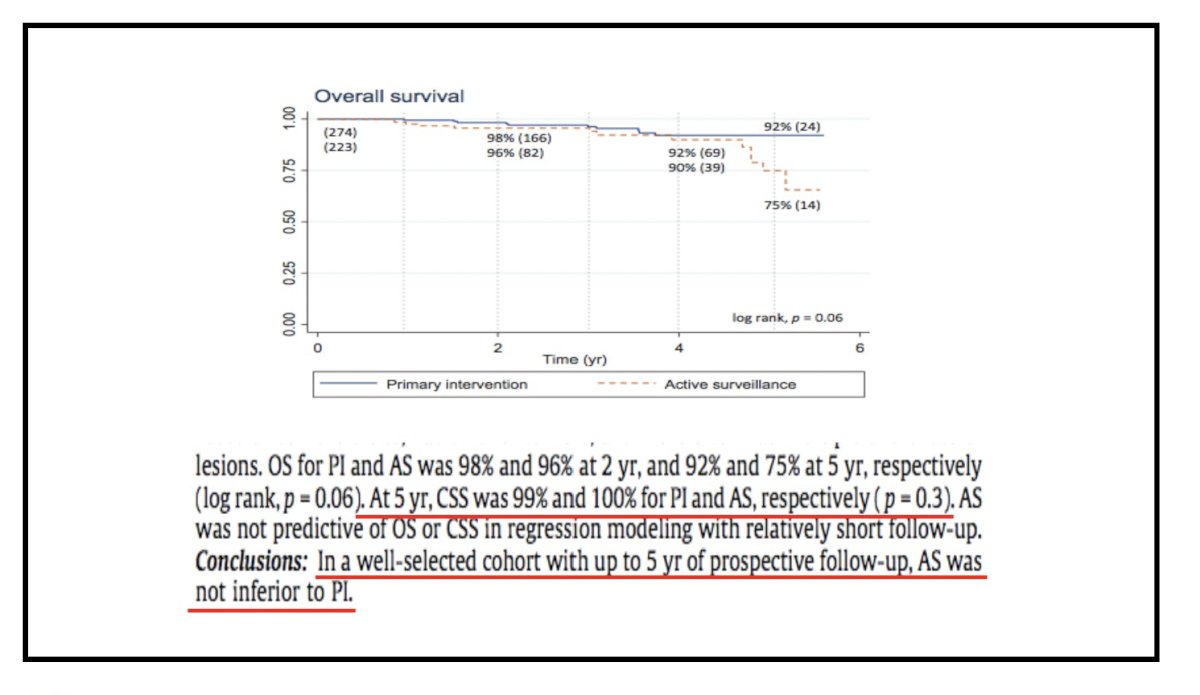
This prospective, multi-institutional cohort offered patients a choice between AS and immediate intervention, with standardized follow-up protocols. Patients choosing AS tended to be older and more comorbid, which accounts for observed differences in all-cause mortality. Cancer-specific survival, however, was excellent across both groups and nearly 100% at 5 years. Median linear growth in the AS cohort was approximately 0.1 cm per year, with 30 percent of tumors demonstrating zero growth throughout surveillance.
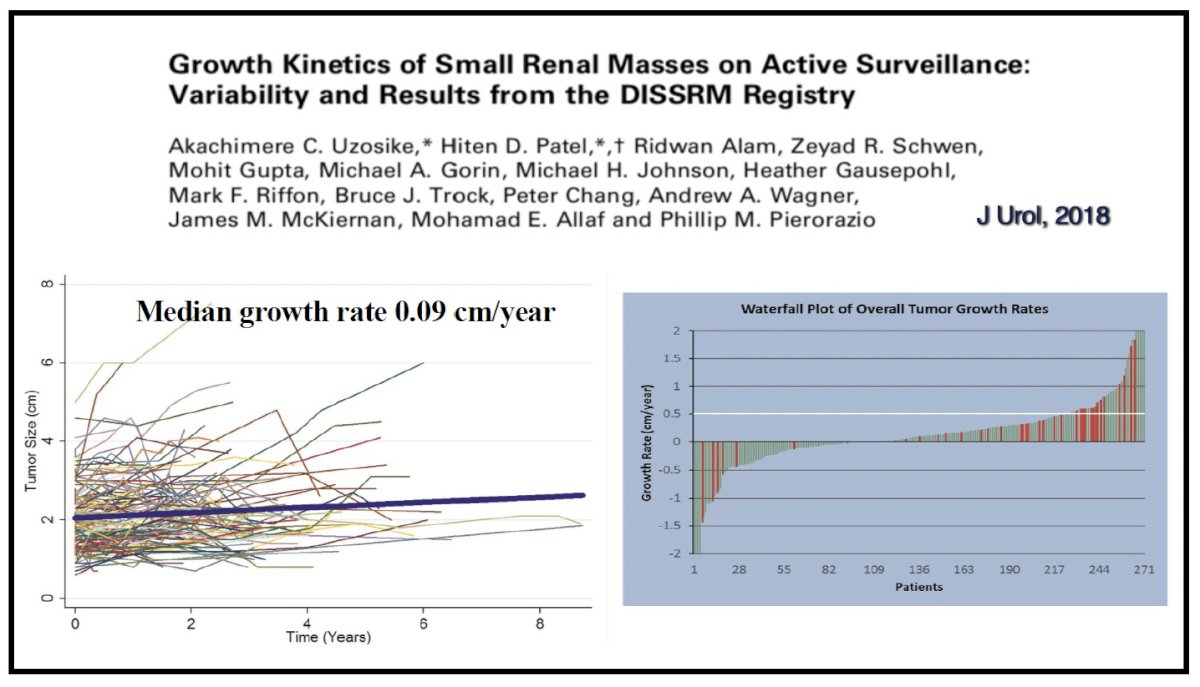
The 5-year probability of requiring delayed intervention was roughly 40 percent, yet treatment was driven far more by patient preference than by oncologic progression. Among those who remained within surveillance guidelines, no patient developed metastasis, providing perhaps the strongest evidence supporting AS as a safe initial strategy.5,6
Volpe highlighted that delayed intervention does not compromise oncologic outcomes. Multiple surgical series demonstrate that partial nephrectomy performed after a period of AS yields equivalent local control, margin rates, and cancer-specific survival compared with immediate surgery.7 Upstaging to pT3 occurs in approximately 3% of cases, a rate indistinguishable from primary surgical cohorts. These findings reassure clinicians and patients that AS preserves curative potential when surveillance triggers—such as increasing size, aggressive biopsy histology, or accelerated growth—are appropriately acted upon.
A major advance in AS personalization is the integration of renal mass biopsy. Gorin and colleagues reported diagnostic accuracies exceeding 90 percent, with minimal complication rates and high concordance with final pathology.8 Biopsy plays a crucial role in distinguishing benign lesions, such as oncocytomas (16–20% of SRMs), and indolent chromophobe RCC, from more aggressive histologies like papillary type 2 or tumors with sarcomatoid differentiation. Its use reduces overtreatment and sharpens risk stratification. In younger patients or those with tumors approaching 3 cm, biopsy provides critical information to guide AS continuation versus intervention.
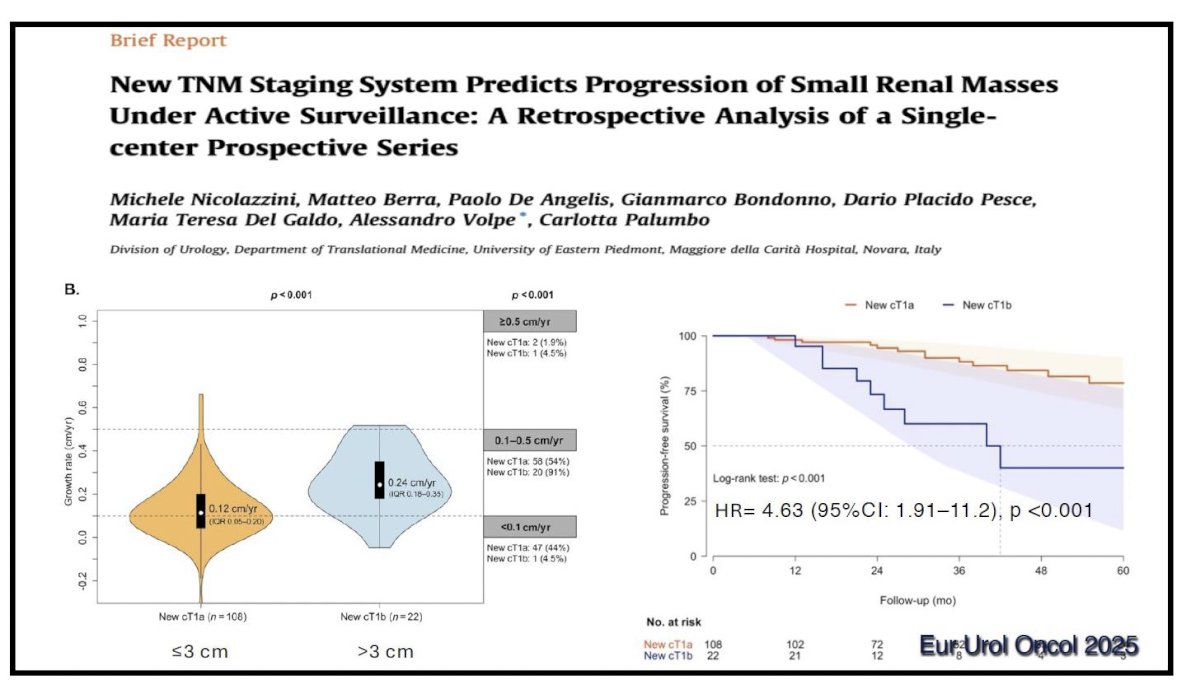
Dr. Volpe then addressed tumor size and proposed refinements to T1a staging. Emerging evidence suggests that tumors ≥3 cm behave differently during AS. Nicolai et al. demonstrated a significant association between baseline size ≥3 cm and time to progression, reporting a hazard ratio of 4.5 for progression in tumors above this threshold.9 Although size alone should not prompt automatic intervention, it supports more intensive surveillance intervals and lowers the threshold for treatment when combined with other adverse features.
What are the limitations of current clinical studies of active surveillance?
- Lack of histological diagnosis in most cases
- Lack of standardized follow-up protocols
- Lack of standardized criteria to indicate delayed intervention
- Limited information on patient’s quality of life and anxiety
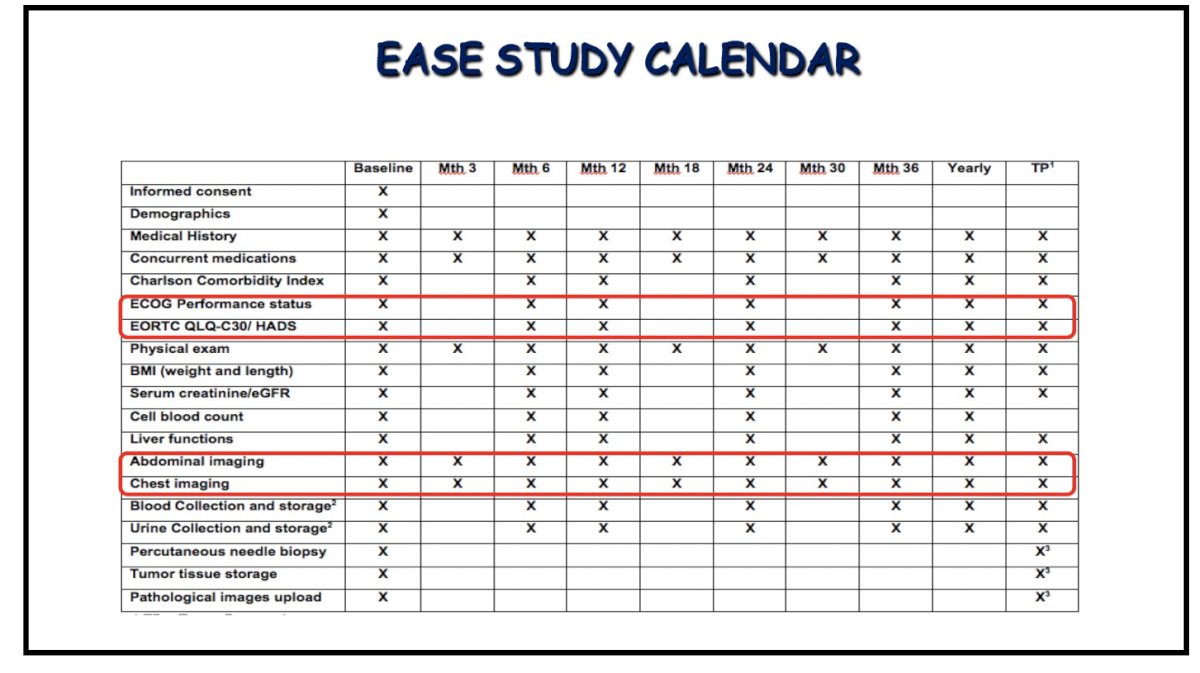
EASE (European Active SurveillancE of Renal Cell Carcinoma) is a multicenter, prospective study of AS for histologically confirmed SRMs that aims to overcome some of these limitation through standardized indications, follow-up, and well-defined criteria for progression and delayed intervention:
What is the goal of AS for SRMs?
- Avoid cancer-specific mortality
- Avoid progression of renal insufficiency to end-stage renal disease (ESRD) and dialysis
- Avoid treatment-related complications
- Allow a good quality of life
Addressing the 1st goal of avoiding cancer-specific mortality, Dr. Volpe highlighted that among elderly patients with small renal cortical tumors, postoperative mortality is driven predominantly by competing comorbidities rather than by progression or lethality of the primary renal malignancy. Even though all patients in the population-based study below underwent nephrectomy, the probability of dying from kidney cancer within five years is low, reflecting the generally indolent natural history of 2–4 cm T1a–T1b masses when appropriately treated.

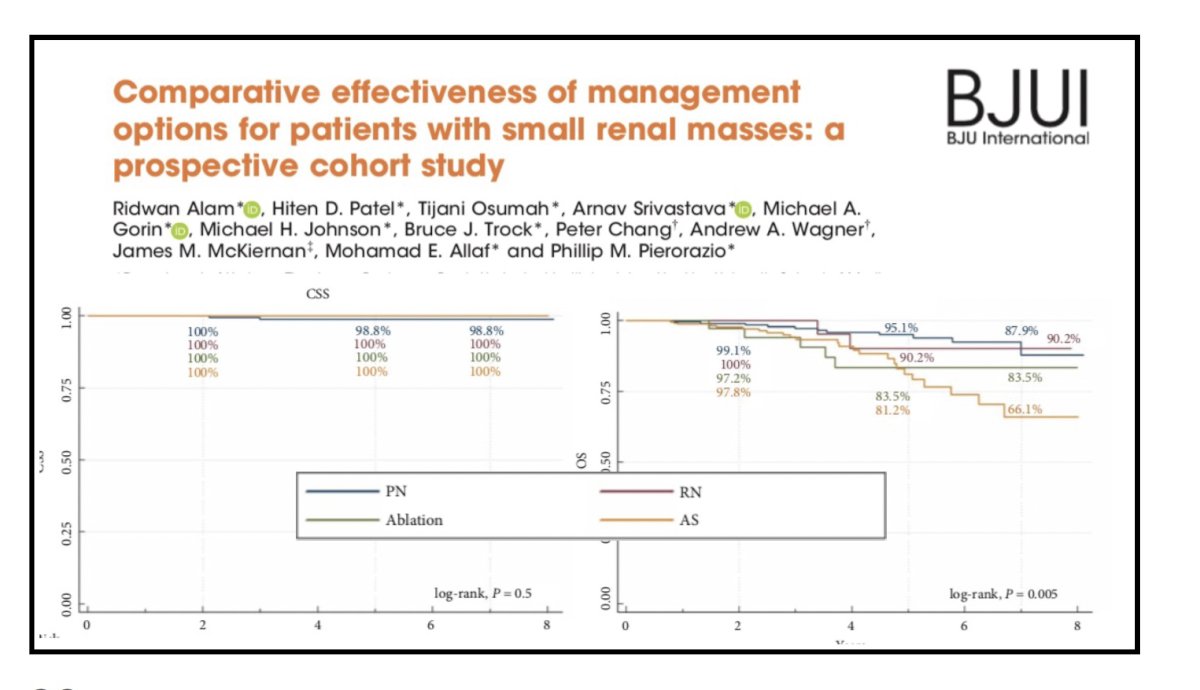
This concept is further reinforced by the study from Alam et al. that compared oncologic outcomes across partial nephrectomy, radical nephrectomy, ablation, and active surveillance for patients presenting with small renal masses. Cancer-specific survival was uniformly excellent across all management strategies, with virtually no cancer-related deaths observed during follow-up. Differences emerged in overall survival, where patients managed with partial nephrectomy and radical nephrectomy demonstrated superior long-term outcomes compared with those undergoing ablation or active surveillance. At approximately eight years, overall survival remained near 90% for partial nephrectomy and radical nephrectomy, whereas ablation and active surveillance showed more pronounced declines, reflecting underlying comorbidity rather than cancer progression. These findings highlight that while cancer-specific mortality for small renal masses is exceedingly low regardless of treatment modality, overall survival is influenced by patient selection and baseline health, underscoring the importance of individualized management balancing tumor biology with competing risks.10
With regards to avoidance of progression to ESRD and dialysis, Dr. Volpe remarked that AS is the ‘perfect nephron-sparing technique’.
AS can be prioritized over active treatment in the following situations:
- In the setting of a solitary kidney
- When active treatments are not feasible or indicated
- In the presence of other comorbidities (e.g., hypertension, diabetes)
- When post-treatment eGFR is likely to be <45 ml/min/1.73 m2
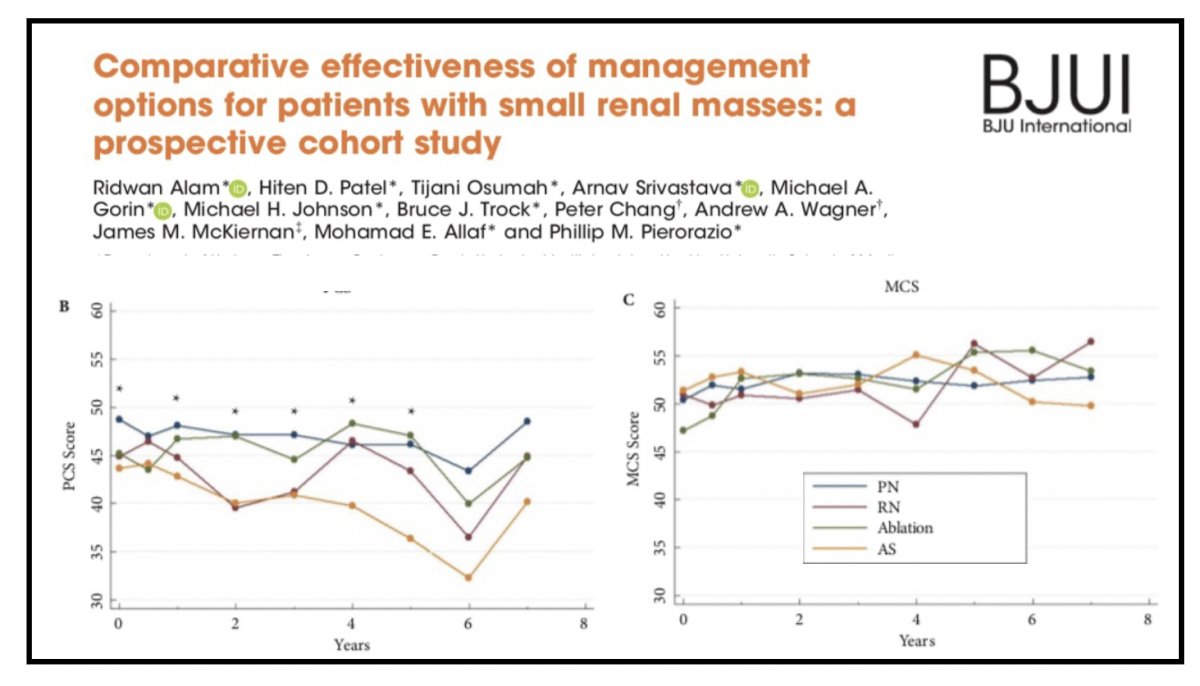
With regards to quality of life, data from Alam et al. comparing Physical Component Scores (PCS) by treatment modality demonstrate that long-term health-related quality of life remains largely comparable regardless of management strategy, supporting individualized decision-making anchored in tumor biology, patient fitness, and personal preference.10
Dr. Volpe concluded as follows:
- Active surveillance is a safe option for patients with an SRM
- Very low metastatic progression rate and cancer-related mortality
- Better preservation of renal function vs. active treatments
- Similar quality of life outcomes
- It is still underutilized in clinical practice
- Patient selection is key
- Renal mass biopsies are important to exclude tumors with aggressive histology
- Molecular and genetic characterization have the potential to become the main drivers in patient selection for AS
Presented by: Alessandro Volpe, MD, Professor, Chairman, University of Eastern Piedmont Maggiore della Carita Hospital, Novara, Italy
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, December 2nd–5th, 2025
References:
- Bosniak MA, Birnbaum BA, Krinsky GA, et al. Small renal parenchymal neoplasms: further observations on growth. Radiology. 1995;197:589-597.
- Volpe A, Panzarella T, Rendon R, et al. The natural history of incidentally detected small renal masses. Cancer. 2004;100:738-745.
- Chawla SN, Crispen PL, Hanlon AL, et al. The natural history of observed enhancing renal masses. J Urol. 2006;175:425-431.
- Smaldone MC, Kutikov A, Egleston BL, et al. Small renal masses progressing to metastases under active surveillance. J Urol. 2012;188:207-213.
- Pierorazio PM, Johnson MH, Ball MW, et al. Five-year analysis of the DISSRM registry for small renal masses. Eur Urol. 2015;68:408-415.
- Mason RJ, Patel HD, Cheaib JG, et al. Growth kinetics and outcomes of small renal masses on active surveillance. J Urol. 2018;199:641-648.
- Mir MC, Derweesh I, Porpiglia F, et al. Partial nephrectomy after active surveillance: oncologic and functional outcomes. Eur Urol. 2017;72:445-451.
- Gorin MA, Pierorazio PM, Kates M, et al. Diagnostic utility of renal mass biopsy in the era of surveillance. BJU Int. 2014;113:939-946.
- Nicolai M, Berzov M, Bruno PA, et al. Refining TNM staging for small renal masses under active surveillance. Eur Urol Oncol. 2025;5:1-10.
- Alam R, Patel HD, Osumah T, et al. Comparative effectiveness of management options for patients with small renal masses: a prospective cohort study. BJU Int. 2019; 123(1):42–50.