(UroToday.com) The 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix between December 2 and December 5, 2025, was host to the Poster Session. Dr. Marston Linehan presented poster #172: LITESPARK-004: 5-year follow-up of the hypoxia-inducible factor-2α (HIF-2α) inhibitor belzutifan in von hippel-lindau (VHL) disease–associated neoplasms.
The HIF-2α inhibitor belzutifan is approved for the treatment of von Hippel–Lindau (VHL) disease–associated renal cell carcinoma (RCC), central nervous system (CNS) hemangioblastomas, and pancreatic neuroendocrine tumors (pNETs) that do not require immediate surgery.
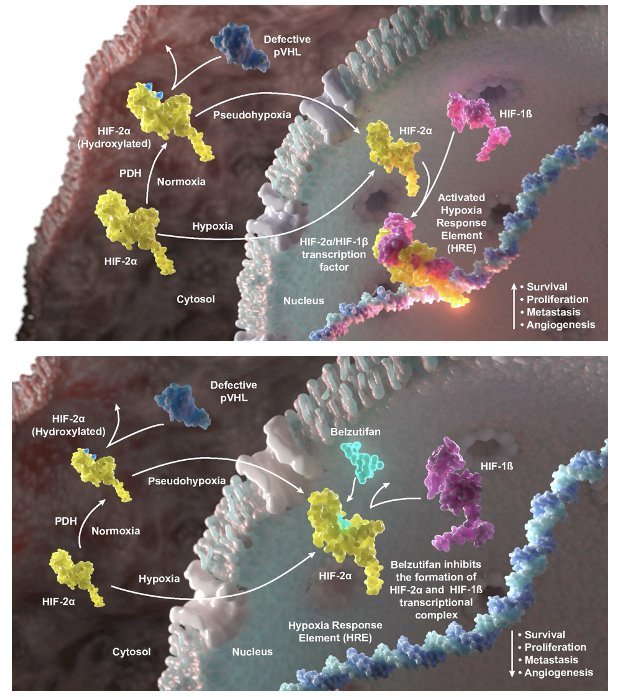
The phase 2 LITESPARK-004 study (NCT03401788) established belzutifan as an active and well-tolerated systemic therapy across these VHL-related neoplasms. Patients with VHL often undergo multiple surgeries over their lifetime to manage tumors and cysts, which can significantly affect quality of life. The mechanism of action of Belzutifan is depicted below.
At the last analysis of the LITESPARK-004 study (minimum study follow-up of 4 years) of belzutifan for VHL disease–associated neoplasms, the following results were observed:
- Objective response rate (ORR):
- RCC: 67%
- CNS hemangioblastoma: 48%
- pNETs: 91%
- The median duration of response (DoR) was not reached for all 3 tumor types
Updated results from LITESPARK-004 are now available after a minimum of 5 years of follow-up, and Dr Linehan presented those at this meeting today.
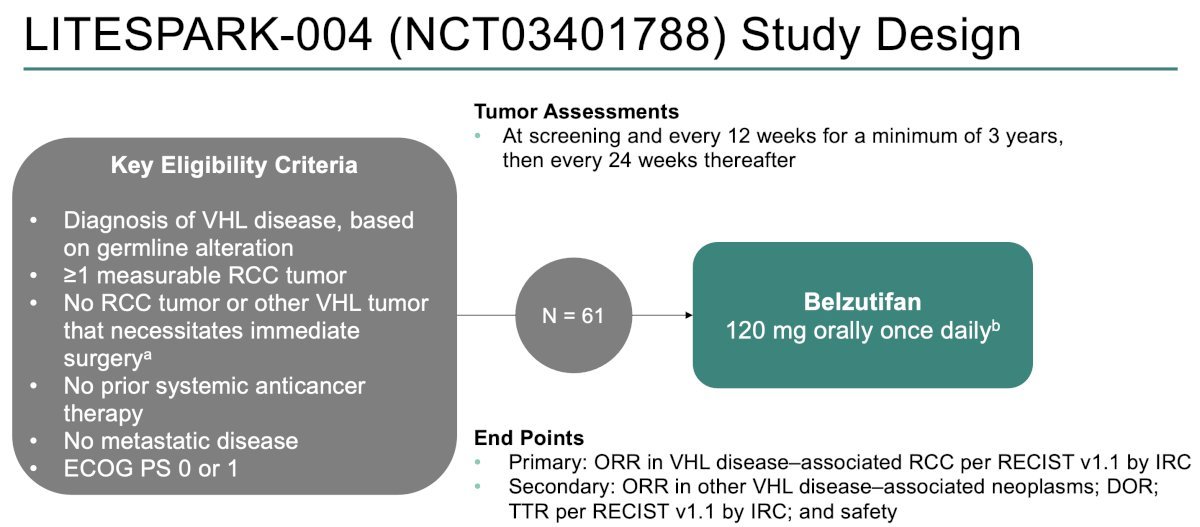
The phase II LITESPARK-004 trial enrolled patients with VHL disease who had a confirmed germline alteration and at least one measurable renal cell carcinoma tumor. Key eligibility criteria required no prior systemic anticancer therapy, absence of metastatic disease, and an ECOG performance status of 0–1.
All participants received belzutifan 120 mg orally once daily. Tumor assessments were performed at screening, then every 12 weeks for a minimum of 3 years, and subsequently every 24 weeks thereafter. The primary endpoint was objective response rate (ORR) in VHL-associated RCC per RECIST v1.1, as assessed by an independent review committee. Secondary endpoints included ORR in other VHL-associated neoplasms, duration of response, time to progression, and safety as shown in the study schema below.
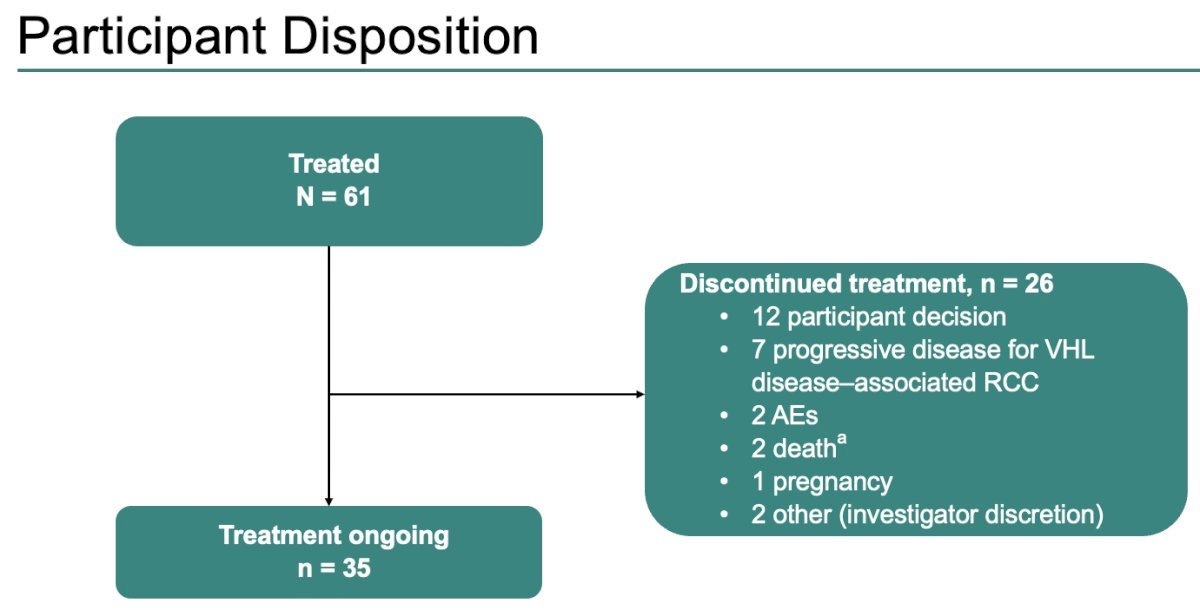
As of the data cutoff, all 61 enrolled participants had received belzutifan, and 35 remained on treatment. Median study follow-up was 61.8 months. Most treatment discontinuations occurred due to participant choice rather than disease progression or toxicity.
At baseline, all 61 participants had RCC. Most also had additional VHL-associated neoplasms, with 50 participants (82%) presenting with at least one evaluable CNS hemangioblastoma and 20 participants (33%) having at least one pancreatic neuroendocrine tumor. Prior to initiating belzutifan, 59 participants (97%) had undergone one or more VHL disease related surgical procedures, underscoring the significant cumulative treatment burden typically experienced by this population.
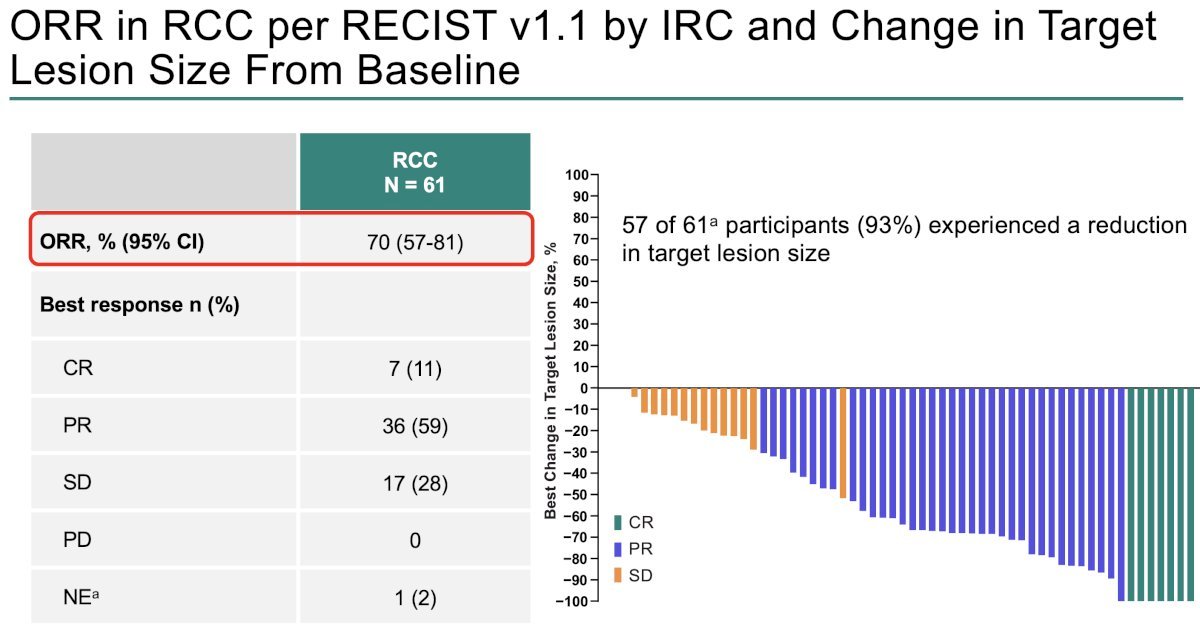
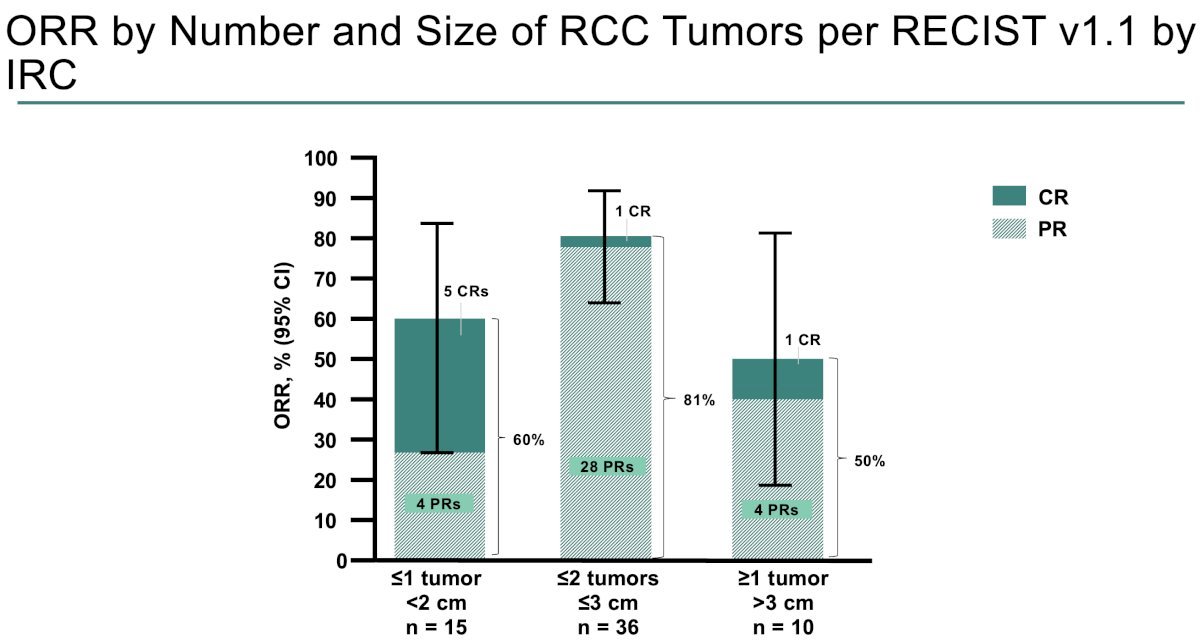
The overall ORR for RCC was 70%, including a complete response in 7 patients (11%) and a partial response in 36 patients (59%). Since the previous data cutoff (April 3, 2023), the ORR increased from 67% to 70.5%, driven by two additional partial responses. Notably, 93% of participants experienced a reduction in the total sum of RCC target lesion diameters from baseline, underscoring the sustained antitumor activity of belzutifan in this VHL population.
ORRs were observed across number/size of RCC lesions. The highest CRs were observed in patients with solitary tumors <2 cm in size (5 complete; 32%).
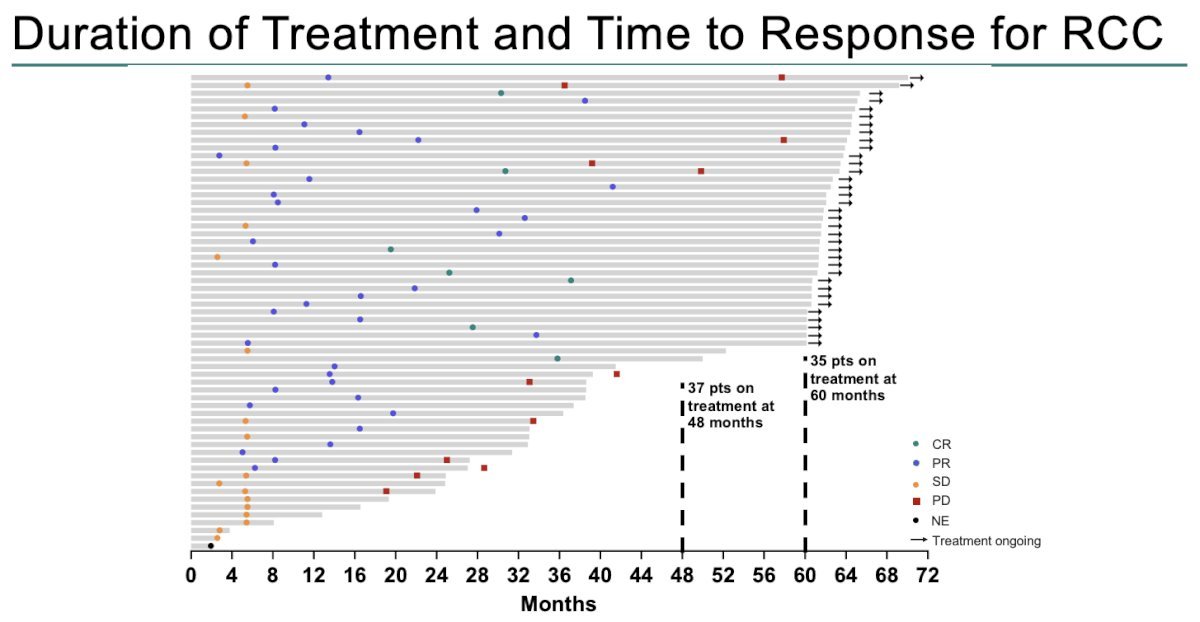
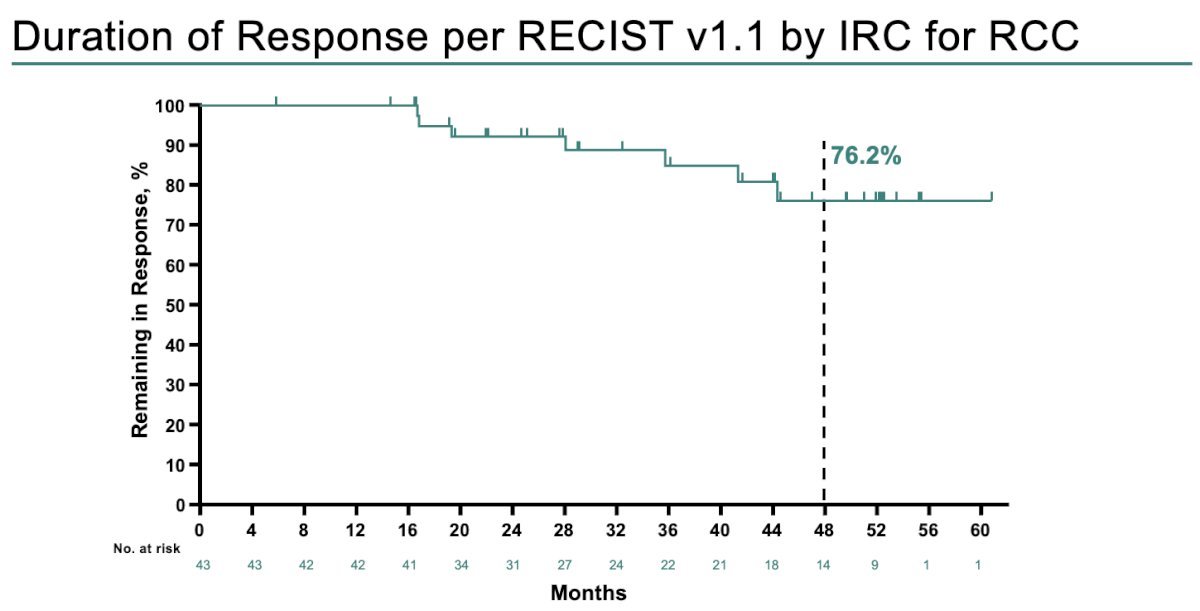
Across VHL-associated tumors, belzutifan produced durable responses with prolonged duration of therapy. In the RCC cohort, median duration of response was not reached, with a 48-month DOR rate of 76% and several patients maintaining responses beyond 60 months; the swimmer plot highlights that 37 patients remained on treatment at 48 months and 35 at 60 months. For CNS hemangioblastomas, median DOR was 60.3 months with an 82% 48-month DOR rate, while pNETs achieved a 48-month DOR rate of 94% with median DOR not yet reached.
Moreover, response durability was substantial across all tumor types. In the RCC cohort, 76.2% of participants remained in response at the 4-year landmark (figure below), highlighting the long-term activity of belzutifan. Comparable durability was observed in the CNS hemangioblastoma group, with 82% maintaining response at 4 years, and durability was even more pronounced in pNETs, where 94% of participants remained in response at the same time point.
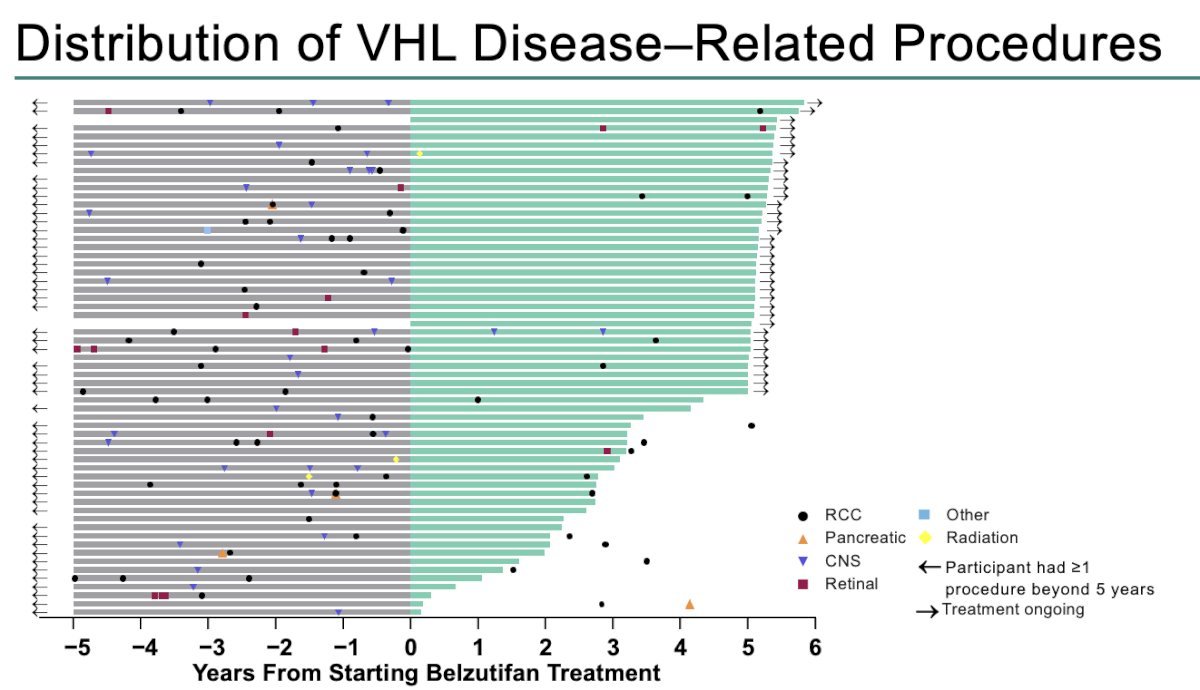
Dr Linehan highlighted that in the LITESPARK-004 study, within the 5 years before initiating belzutifan, 46 participants (75%) had undergone at least one VHL-related surgery. After starting belzutifan, 19 participants (31%) required additional VHL-related procedures. Four patients had surgery while on treatment and subsequently discontinued therapy, eight underwent surgery after stopping treatment, and seven remained on treatment at the data cutoff. Median time to first postscreening surgery has not yet been reached.
All participants experienced at least one treatment-related adverse event (TRAE), though the vast majority were low grade. Grade 3 TRAEs occurred in 11 participants (18%), and importantly, no grade 4 or 5 treatment-related events were observed.
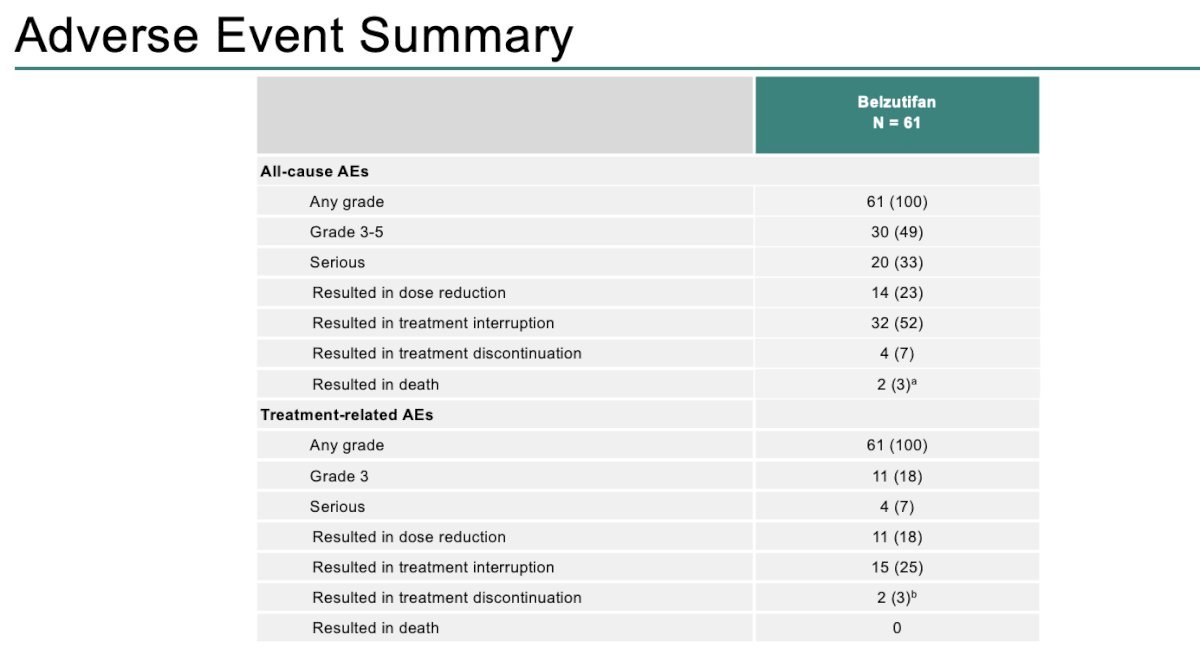
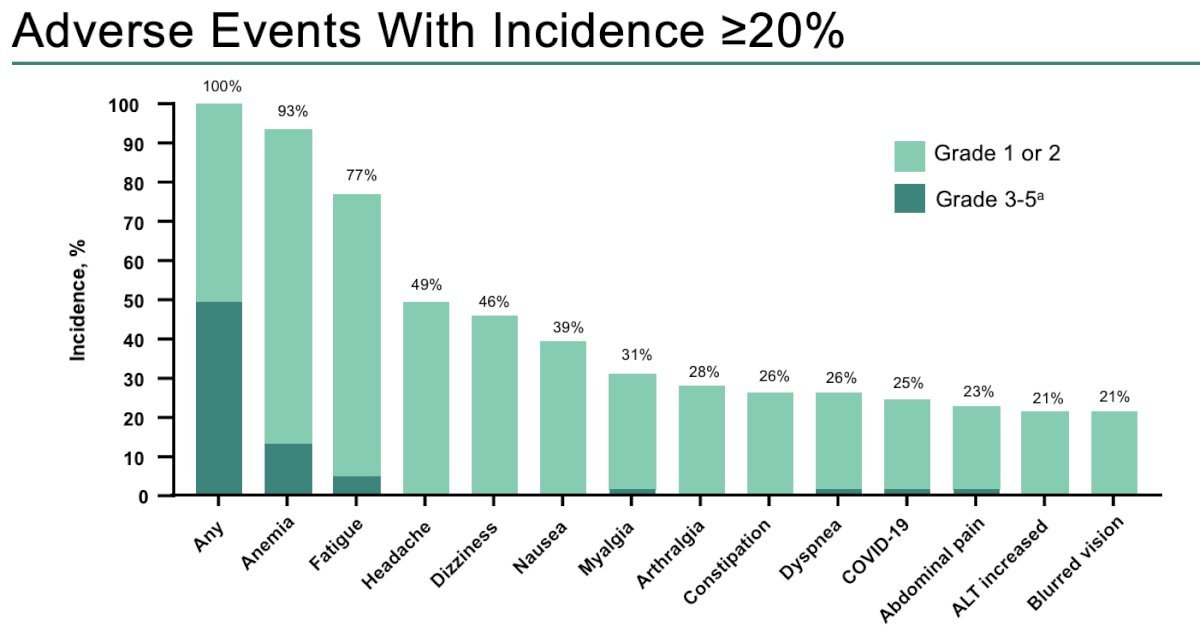
Additionally, since the most recent data cutoff on April 1, 2024, no further participants discontinued treatment or died, supporting the continued tolerability of long-term belzutifan therapy. Adverse events with an incidence ≥20% are summarized in the graph below:
Dr. Linehan concluded his presentation of the updated results from the LITESPARK-004 trial as follows:
- With a median follow-up of 61.8 months, belzutifan continues to demonstrate durable and clinically meaningful activity across VHL-associated tumors.
- ORR was 70% in RCC, 50% in CNS hemangioblastomas, and 90% in pNETs.
- Responses were durable, with most responders maintaining disease control at the 48-month assessment.
- These long-term outcomes reinforce that belzutifan may delay or, in some cases, reduce the need for repeated surgical interventions in patients with VHL disease.
- No new safety signals emerged with extended follow-up.
- Belzutifan remains the only approved systemic therapy for VHL-associated RCC, pNETs, or CNS hemangioblastomas that does not require immediate surgery.
Presented by: W. Marston Linehan, MD, National Cancer Institute, Rockville, MD, USA
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Penn State Health, @chavarriagaj on Twitter during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.