(UroToday.com) The 2025 Society of Urologic Oncology (SUO) annual meeting, held in Phoenix between December 2 and December 5, 2025, was host to the Poster Session. Dr. Naomi Haas presented poster #158: Five-year follow-up results from the phase 3 KEYNOTE-564 study of adjuvant pembrolizumab for the treatment of clear cell renal cell carcinoma.
Dr. Hass opened by reviewing KEYNOTE-564 (NCT03142334), the randomized, double-blind, placebo-controlled phase 3 trial that established pembrolizumab monotherapy as the first adjuvant treatment to significantly improve disease-free and overall survival after nephrectomy in patients with renal cell carcinoma at increased risk of recurrence. 1 She presented updated findings from the fourth prespecified interim analysis, now with a minimum follow-up of five years.
KEYNOTE-564 is a randomized, double-blind, placebo-controlled phase 3 trial enrolling adults with clear cell RCC at intermediate-high risk (pT2 Grade 4 or sarcomatoid features, or pT3 any Grade, N0 M0), high risk (pT4 any Grade, N0 M0, or any pT/Grade with N+ M0), or M1 with no evidence of disease following nephrectomy and/or metastasectomy. Eligible participants were required to begin treatment within 12 weeks of surgery and were randomized 1:1 to pembrolizumab 200 mg or placebo every three weeks. Therapy continued for approximately one year (17 cycles) or until recurrence, unacceptable toxicity, or physician-directed discontinuation. The trial schema is shown above.
The primary endpoint was investigator-assessed disease-free survival, with overall survival as the key secondary endpoint. Both endpoints were met at earlier analyses, so no further formal hypothesis testing was performed in this update. Adverse events were collected for 30–90 days after treatment completion based on severity, and serious treatment-related events were captured regardless of timing. The study schema is illustrated below.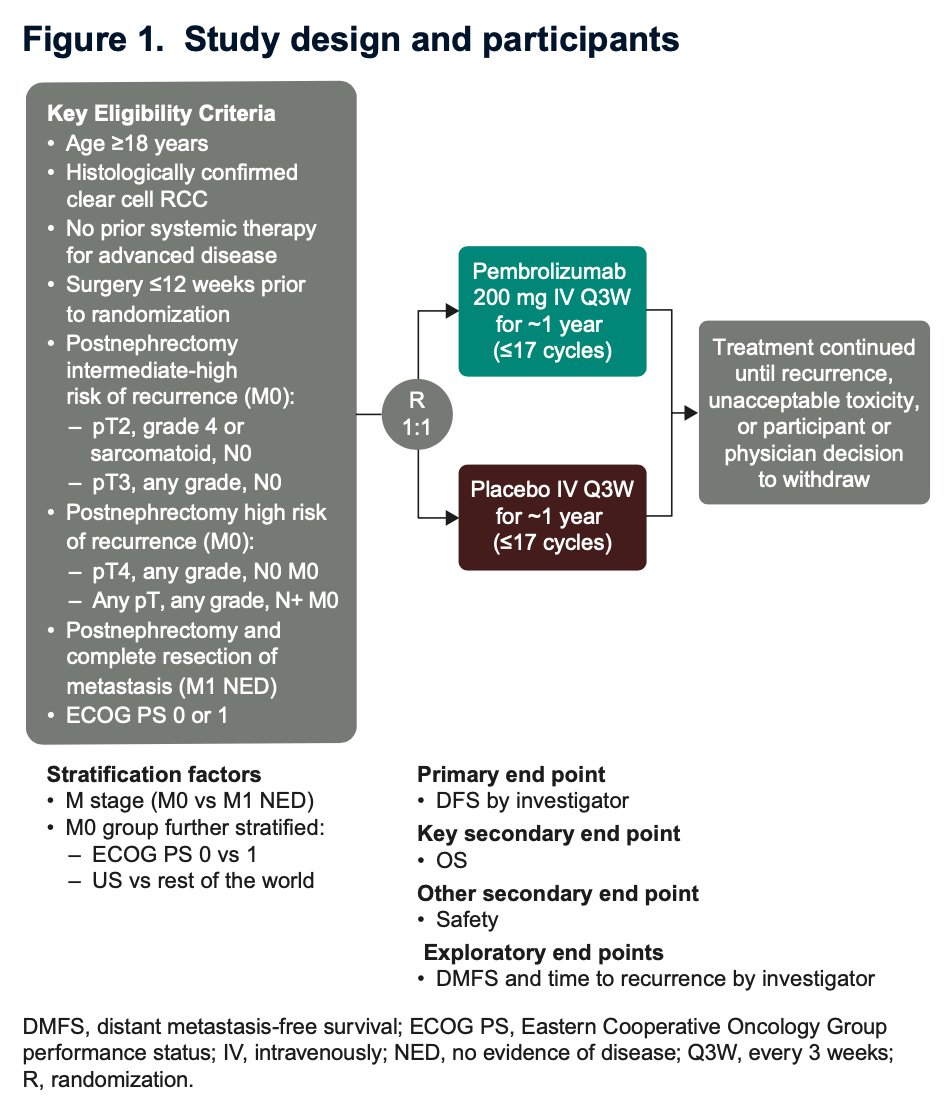
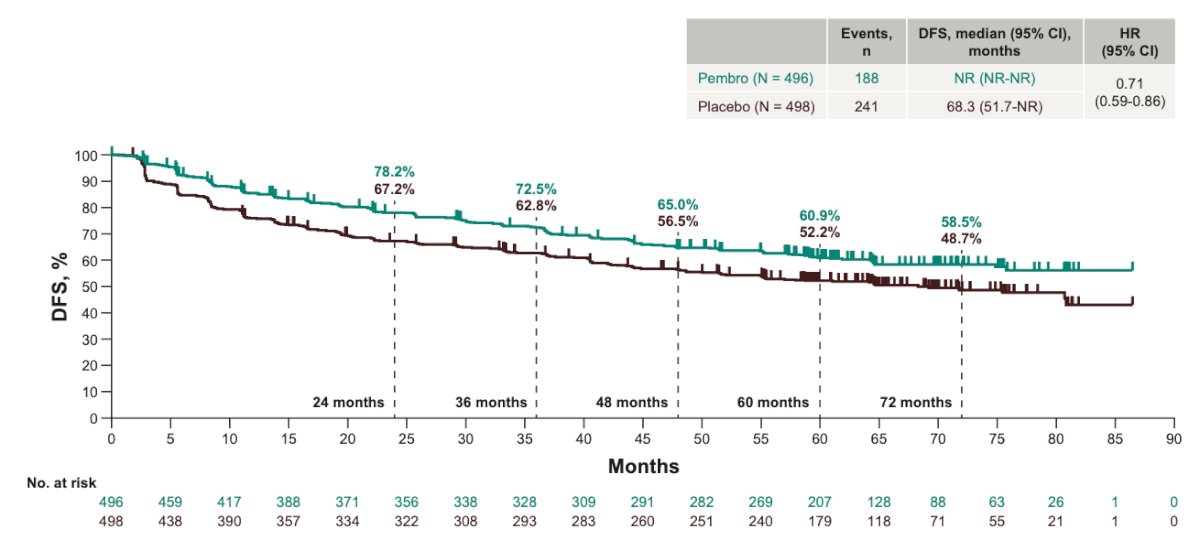
A total of 994 patients were randomized to pembrolizumab (n=496) or placebo (n=498). At the data cutoff of September 25, 2024, median follow-up was 69.5 months (range 60.2–86.9), and all participants had completed or discontinued study therapy at least three years earlier. There were 188 disease-free survival events in the pembrolizumab arm and 241 in the placebo arm. Median DFS was not reached with pembrolizumab versus 68.3 months with placebo, corresponding to an HR of 0.71 (95% CI 0.59–0.86) as shown in the Kaplan-Meier curves below. The estimated five-year DFS rates were 60.9 percent and 52.2 percent, respectively.
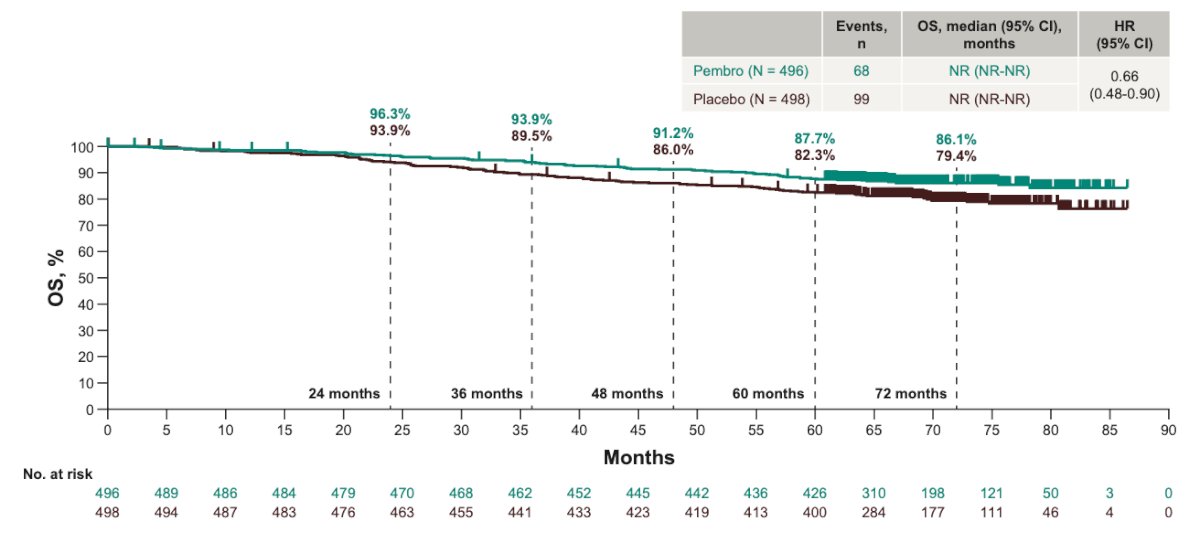
There were 68 overall survival events in the pembrolizumab arm and 99 in the placebo arm. Median OS was not reached in either group, and pembrolizumab demonstrated a sustained survival advantage with an HR of 0.66 (95 percent CI 0.48–0.90). The estimated five-year OS rate was 87.7 percent versus 82.3 percent, respectively. As shown in the prespecified subgroup analyses, the DFS and OS benefits of pembrolizumab were directionally consistent across intermediate-high-risk–risk, high-risk, and M1 NED cohorts, as well as in patients with and without sarcomatoid features. HR estimates favored pembrolizumab across nearly all strata, reinforcing the robustness of the treatment effect.
As shown in the prespecified subgroup analyses, the DFS and OS benefits of pembrolizumab were directionally consistent across intermediate-high–risk, high-risk, and M1 NED cohorts, as well as in patients with and without sarcomatoid features. HR estimates favored pembrolizumab across nearly all strata, reinforcing the robustness of the treatment effect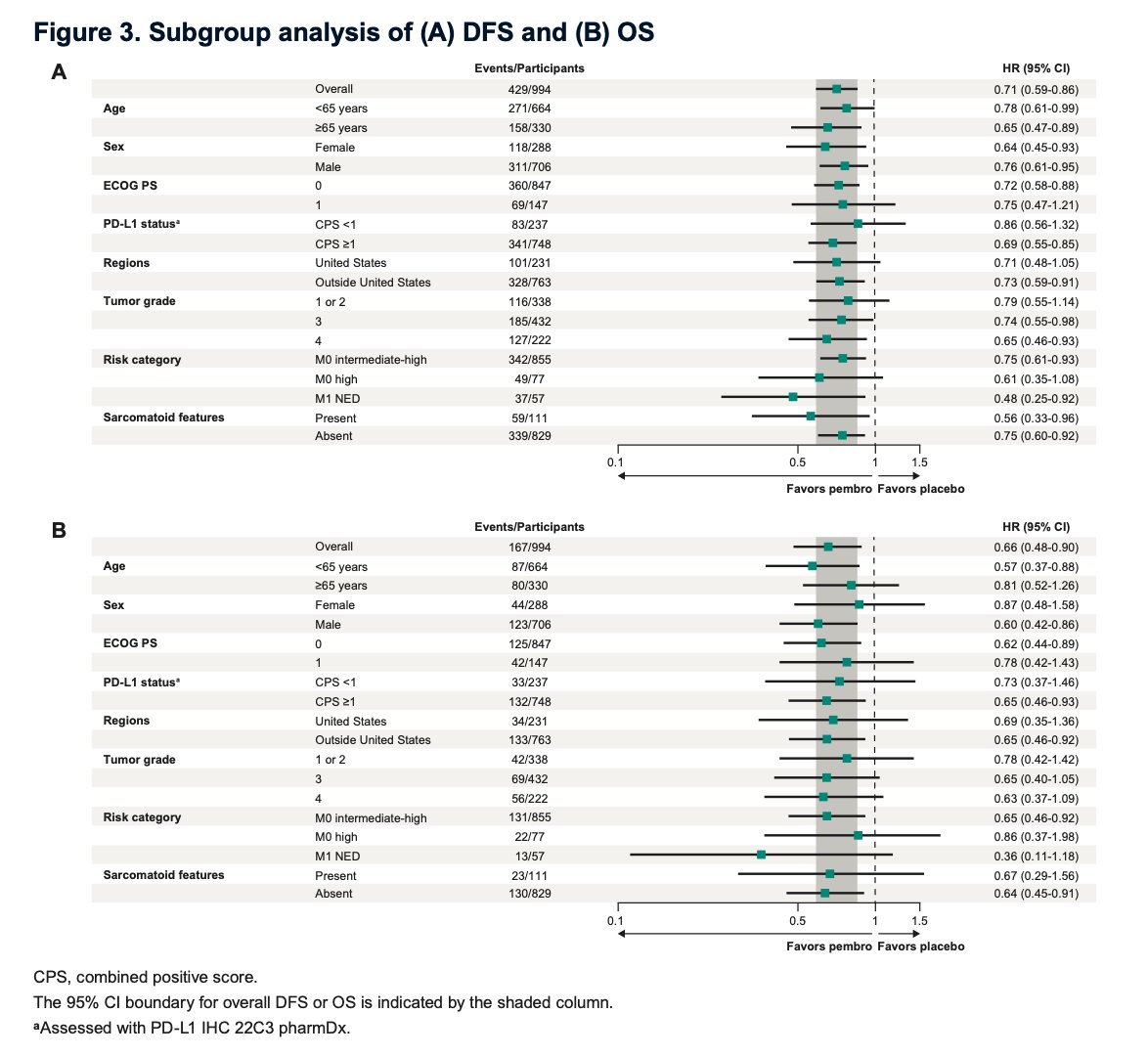
Moreover, subgroup analyses showed that pembrolizumab consistently improved overall survival across all risk categories. Benefits were evident in M0 intermediate-high and M0 high-risk patients, with durable separation of the OS curves despite low event rates. The strongest relative benefit was observed in the M1 NED subgroup (HR 0.36), highlighting pembrolizumab’s robust and sustained survival advantage even in patients at the highest risk for recurrence.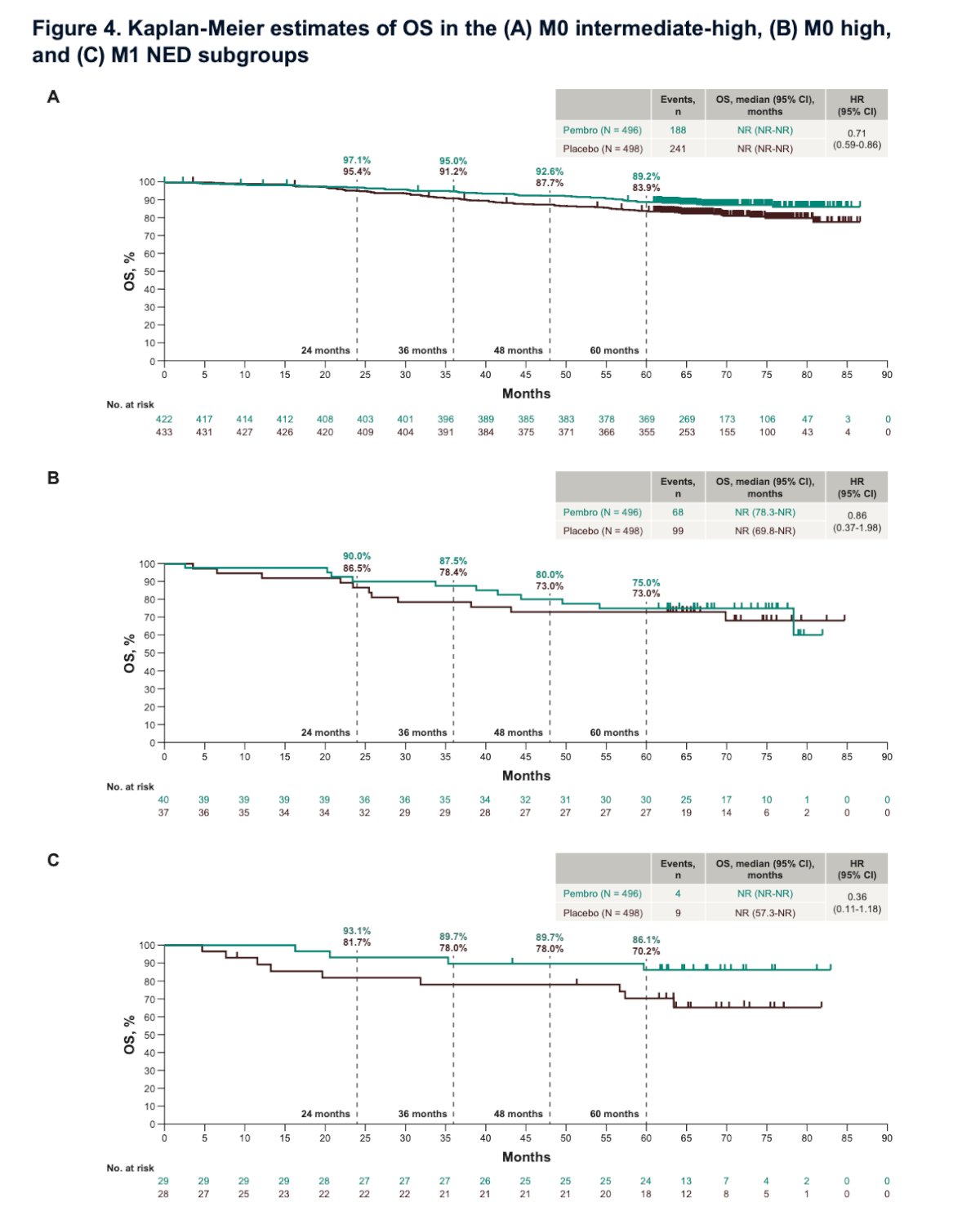
Dr. Haas highlighted that distant metastasis–free survival (DMFS) and time-to-recurrence outcomes further supported the benefit of adjuvant pembrolizumab. DMFS events occurred in 174 patients on pembrolizumab versus 220 on placebo, with median DMFS not reached compared to 80.7 months, respectively (HR 0.73, 95% CI 0.60–0.89). The 5-year DMFS rate was 63.3% versus 55.3%. Similarly, time-to-recurrence events were fewer with pembrolizumab (171 vs 226), with median time to recurrence not reached versus 80.9 months (HR 0.69, 95% CI 0.57–0.84). The estimated 5-year recurrence-free rate was 63.3% versus 54.5%.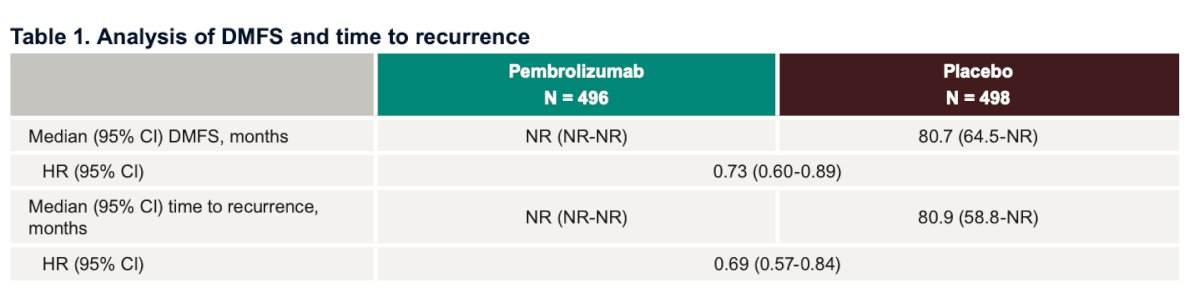
Notably, subsequent therapies were administered at similar rates in participants with documented recurrence, 64.3% in the pembrolizumab arm vs 68.1% in the placebo arm, underscoring the robustness of the KEYNOTE-564 survival benefit despite comparable post-recurrence treatment exposure.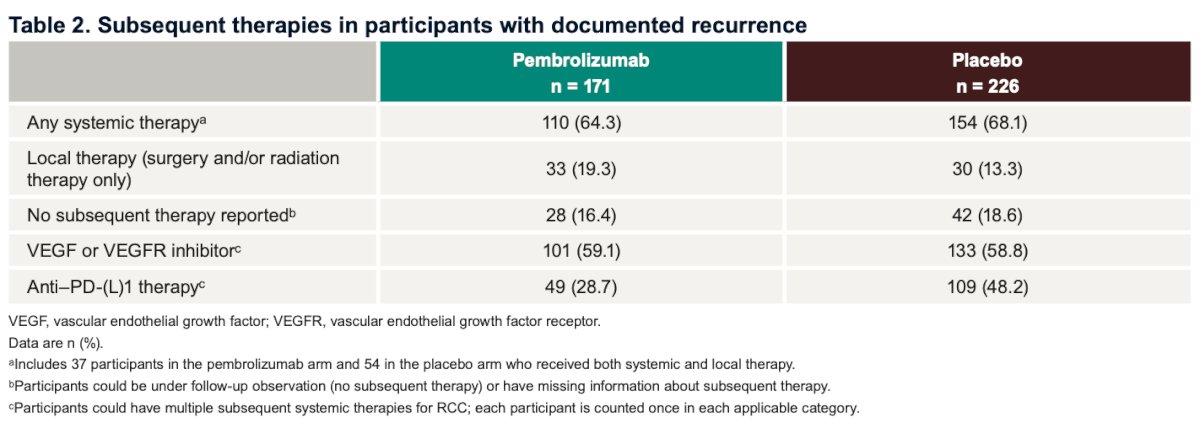
Lastly, no new serious treatment-related adverse events (TRAEs) have been reported in more than three years, supporting the long-term safety of pembrolizumab. The median treatment duration was 11.1 months, and grade 3–4 TRAEs occurred in 18.6% of pembrolizumab-treated patients versus 1.2% with placebo, with no grade 5 events in either arm. Immune-mediated grade 3–4 events remained rare (<10%), and overall, discontinuations due to toxicity were infrequent.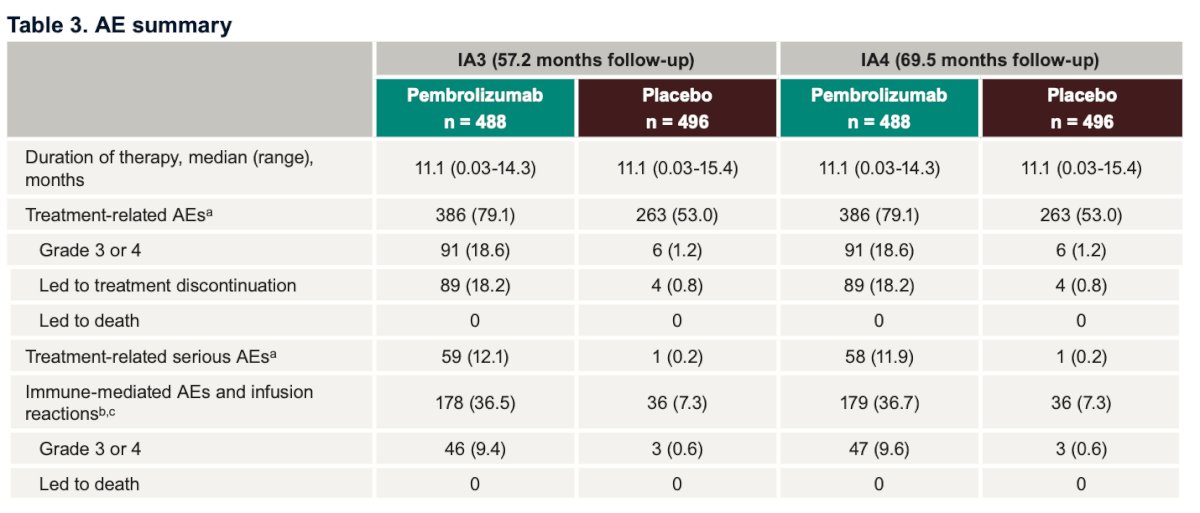
Dr. Haas concluded her presentation with the following take-home messages:
- With a minimum of five years of follow-up, adjuvant pembrolizumab continued to improve disease-free and overall survival compared with placebo in patients with clear cell RCC at increased risk of recurrence.
- DFS and OS benefits remained consistent in the overall study population and across all prespecified subgroups.
- Pembrolizumab also improved DMFS and time to recurrence compared with placebo
- Patterns of subsequent therapy included both local treatments, such as surgery or radiation, and systemic agents.
- No new serious treatment-related adverse events have been reported for more than three years.
- Pembrolizumab remains the only adjuvant therapy in RCC to demonstrate an overall survival benefit, reinforcing its role as the standard of care for appropriate high-risk patients.
Presented by: Naomi Haas, MD, Medical Oncologist, Professor of Medicine (Hematology-Oncology) at the Hospital of the University of Pennsylvania, PA, United States of America.
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Penn State Health, @chavarriagaj on Twitter during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
Reference: