(UroToday.com) Minimal residual disease (MRD) is an area of significant interest in urothelial carcinoma, particularly with the emergence of ctDNA-based assays capable of detecting molecular disease long before visible radiographic recurrence. In this SUO 2025 presentation, Dr. Parminder Singh reviewed the evolving definitions of MRD in metastatic urothelial carcinoma, the biologic and analytic foundations of ctDNA detection, and the rapidly expanding body of clinical evidence supporting ctDNA as a prognostic, predictive, and potentially actionable biomarker across localized and advanced disease.
MRD refers to the presence of residual cancer following definitive therapy, detected through cellular, biomarker-based, or molecular evidence that remains undetectable to standard imaging or direct visualization.1 In urothelial carcinoma, ctDNA-based MRD detection represents the most mature and clinically applicable approach. Assays fall into two broad categories:
- Tumor-informed assays: requiring prior tumor tissue sequencing to generate personalized mutation panels. These assays typically offer higher sensitivity, making them most suitable for post-operative MRD detection and surveillance.
- Tumor-uninformed (tumor-agnostic) whole-genome sequencing (WGS) assays: enabling broader mutation detection and sometimes guiding precision-medicine strategies, though often with lower sensitivity for low-burden disease.
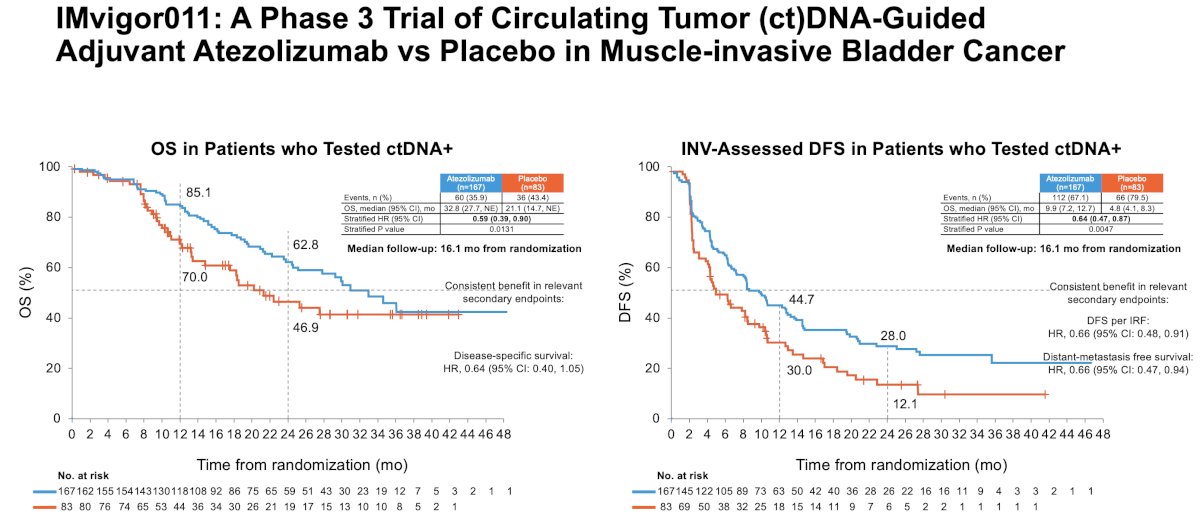
IMvigor011 is a global, randomized phase III trial that evaluated ctDNA-guided adjuvant atezolizumab versus placebo in patients with muscle-invasive urothelial carcinoma after radical surgery.3 Only patients who tested ctDNA-positive after surgery were randomized, providing the first large-scale evaluation of treatment selection based on molecular MRD status.
With a median follow-up of 16.1 months, ctDNA-positive patients treated with atezolizumab experienced significantly superior outcomes across multiple endpoints. Investigator-assessed disease-free survival curves demonstrated clear early separation, with durable benefit maintained over time (HR: 0.64, 95% CI: 0.47–0.87, p=0.0047). The OS curves similarly favored atezolizumab (median: 33 vs 21 months; HR: 0.59, 95% CI: 0.39–0.90, p=0.013). Other secondary endpoints similarly favored adjuvant atezolizumab in ctDNA+ patients:
- Distant metastasis-free survival: HR=0.66 (95% CI: 0.47–0.94)
- DFS per independent review: HR=0.66 (95% CI: 0.48–0.91)
- Disease-specific survival: HR=0.64 (95% CI: 0.40–1.05)
In contrast, ctDNA-positive patients receiving placebo had high and early recurrence rates, underscoring the prognostic significance of molecularly detectable MRD.
IMvigor011 participants who persistently tested ctDNA-negative during serial monitoring experienced favorable outcomes, with >95% DFS and OS at ~22 months post-cystectomy. Only a small fraction (4.2%) recurred during the surveillance phase, underlining the importance of ctDNA-negative status for identifying a ‘truly low-risk’ population.
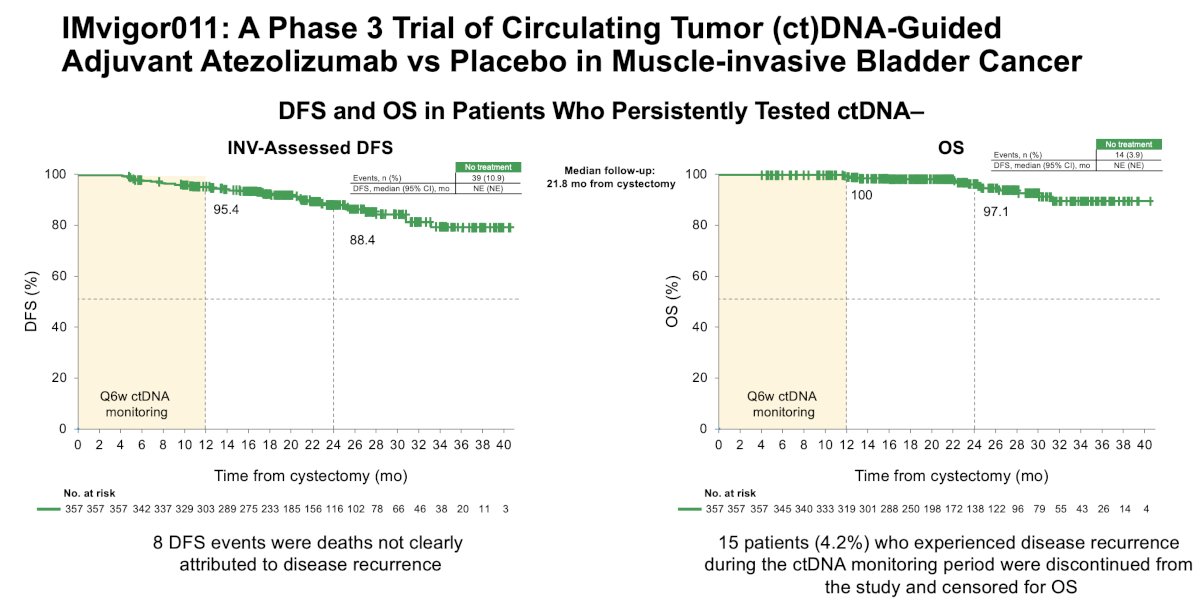
Notably, 8 DFS events in the ctDNA-negative cohort were deaths not clearly attributable to cancer recurrence, highlighting the need for careful adjudication of events in MRD-focused trials.
CheckMate 274: Post-hoc ctDNA AnalysesAdditional insight into the significance of ctDNA in the muscle-invasive urothelial carcinoma adjuvant setting comes from CheckMate 274, the landmark phase III trial of adjuvant nivolumab therapy.3 While ctDNA was evaluable in only 133 of the 709 randomized patients (19%), the findings were significant: baseline ctDNA detectability strongly correlated with worse DFS (52.1 vs 5 months; HR: 0.30, 95% CI: 0.18–0.48) and OS (not reached vs 28.2 months; HR: 0.44, 95% CI: 0.25–0.76). Patients with undetectable ctDNA had >10-fold longer median DFS than those with detectable ctDNA.
These post hoc analyses were limited by sample collection feasibility and small evaluable numbers, but they consistently reinforced the value of ctDNA as a powerful prognostic biomarker.

Dr. Singh then reviewed data from Sumiyoshi et al., which demonstrated the value of ctDNA fraction as a surrogate for tumor burden and its ability to reflect the impact of prior metastasectomy.4 ctDNA mutations showed substantial but incomplete concordance with tissue biopsies; 50.2% of mutations were shared between ctDNA and tumor tissue, while 17.6% and 32.2% were exclusive to ctDNA or tissue, respectively. These findings highlight the ability of ctDNA to capture clinically relevant mutational heterogeneity that may be missed by single-site tissue sampling.
Moreover, increases in ctDNA fraction consistently correlated with poor outcomes. In pembrolizumab-treated patients, increases or lack of decline in ctDNA were associated with significantly worse PFS and OS (both p<0.001), and substantially lower objective response rates⁵. These data suggest that early ctDNA kinetics may provide a timely indicator of immunotherapy response or resistance.

Whether ctDNA dynamics vary by treatment class remains a topic of ongoing investigation. Early data suggest that immune checkpoint inhibitors produce more variable ctDNA responses than chemotherapy, potentially reflecting delayed tumor clearance or immune-related fluctuations. In an exploratory analysis of KEYNOTE-36, ctDNA profiling demonstrated its ability to serve as a tumor tissue surrogate for genomic stratification and outcome prediction under pembrolizumab-based therapy.⁶

Baseline ctDNA as a Prognostic and Predictive Marker
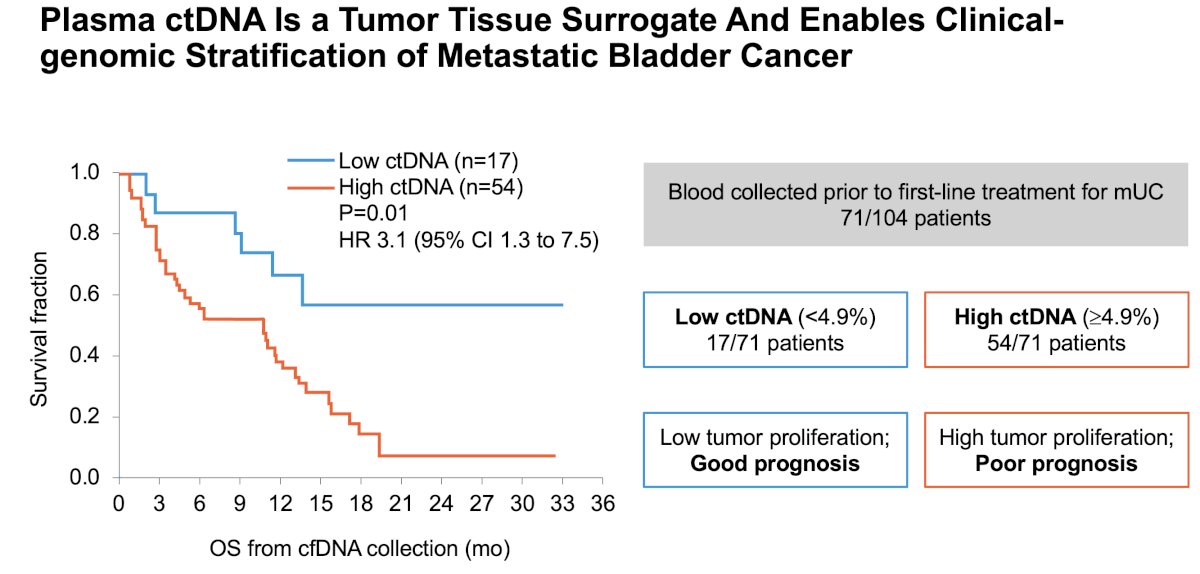
Multiple studies have shown that high baseline ctDNA levels are linked with worse outcomes in metastatic urothelial carcinoma. Vandekerkhove et al. demonstrated that patients with high ctDNA had markedly worse OS (HR 3.1; 95% CI 1.3–7.5).7
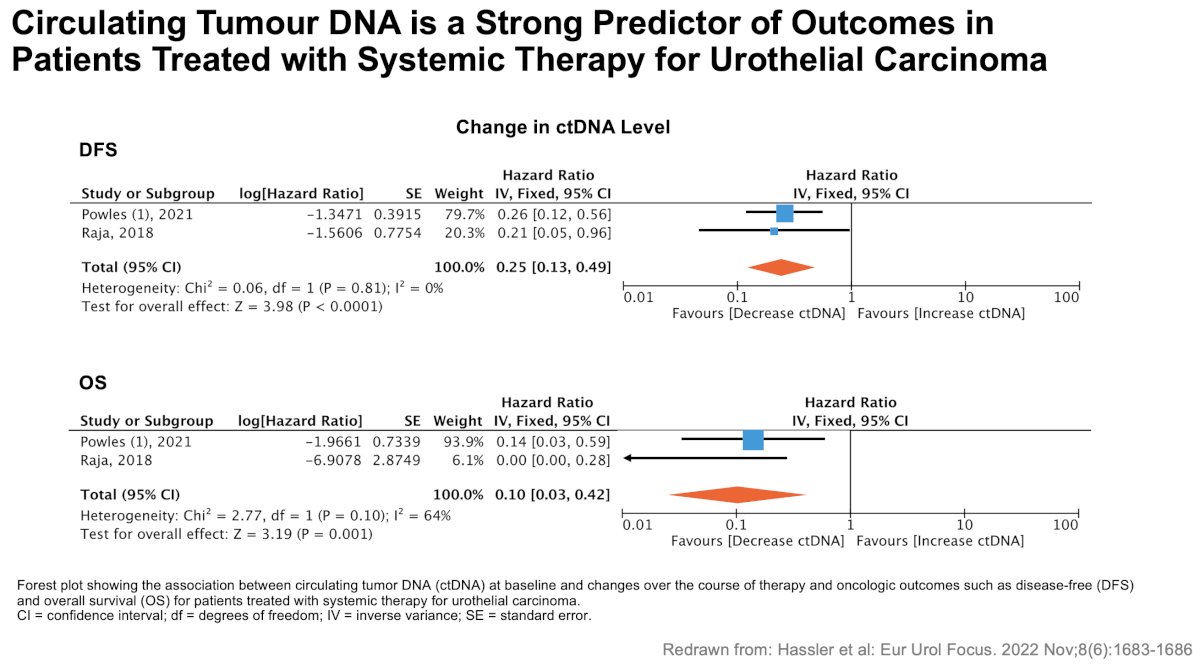
Hassler et al. further showed that both baseline ctDNA status and changes over treatment strongly correlated with DFS and OS across systemic therapies, supporting ctDNA as an independent prognostic marker.8
Dr. Singh highlighted four potential applications of ctDNA in advanced urothelial carcinoma:
- Prognosis — stratifying patients into high- and low-risk categories
- Predictive value — potentially guiding treatment selection (e.g., chemotherapy vs immunotherapy)
- Therapy escalation/de-escalation — MRD-positive patients may benefit from intensification, whereas MRD-negative patients may avoid unnecessary treatment
- Genomic evolution — ctDNA enables monitoring of emerging resistance mechanisms and identification of new therapeutic targets
As ctDNA technologies mature, prospective ctDNA-guided trials—similar to IMvigor011—will be essential to validate how MRD detection and kinetics should influence patient management in both localized and metastatic urothelial carcinoma. Further work is needed to define optimal testing intervals, thresholds for clinical action, and integration with imaging and clinical assessment.
Presented by: Parminder Singh, MD, Department of Internal Medicine, Mayo Clinic Arizona, Phoenix, AZ
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, December 2nd–5th, 2025
References:- Alvarez J, Patel VG, Singla N, et al. Minimal residual disease in urothelial carcinoma: Definitions and emerging biomarkers. Urol Oncol. 2024; 42:113-121.
- Powles T, Kann AG, Davarpanah NN, et al. IMvigor011: A phase III trial of ctDNA-guided adjuvant atezolizumab in muscle-invasive bladder cancer. ESMO 2025 Congress.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Long-term outcomes of adjuvant nivolumab in high-risk muscle-invasive urothelial carcinoma: ctDNA exploratory analyses from CheckMate 274. J Clin Oncol. 2024; 42:1105-1115.
- Sumiyoshi T, Sakamoto N, Fukumoto K, et al. Genomic heterogeneity captured through cfDNA in metastatic urothelial carcinoma. JCO Precis Oncol. 2025; 9:e2400472.
- Mehra R, Pal SK, Agarwal N, et al. ctDNA kinetics and outcomes with pembrolizumab in advanced urothelial carcinoma. Cancer. 2024; 130:2110-2120.
- Grivas P, Plimack ER, Petrylak DP, et al. KEYNOTE-361 exploratory ctDNA analyses: Genomic stratification and dynamic changes under pembrolizumab-based therapy. Nat Med. 2024; 30:2508-2516.
- Vandekerkhove G, Lavoie JM, Annala M, et al. Prognostic significance of baseline ctDNA in metastatic bladder cancer. Nat Commun. 2021; 12:184.
- Hassler MR, Hjorth L, Filipovic A, et al. ctDNA as a predictor of survival in urothelial carcinoma receiving systemic therapy. Eur Urol Focus. 2022; 8:1683-1686.