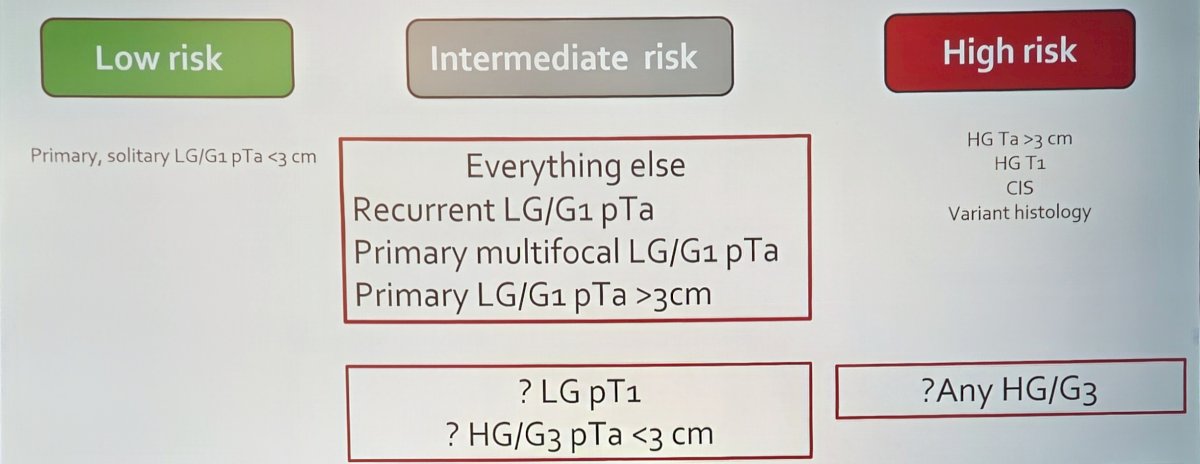
(UroToday.com) The 2025 SUO annual meeting featured a bladder cancer session and a presentation by Dr. Wei Shen Tan discussing risk stratification for intermediate risk non muscle invasive bladder cancer. Dr. Tan started his presentation by highlighting the modern framework of non muscle invasive bladder cancer subgroups—low risk, intermediate risk, and high risk—emphasizing the clinical criteria included in each category:
- Low-risk disease includes: primary, solitary LG/G1 pTa < 3 cm
- High-risk disease is defined by any of the following features:
- HG Ta > 3 cm
- HG T1
- CIS
- Variant histology
- He notes that “everything else” falls under intermediate risk, which includes:
- Recurrent LG/G1 pTa
- Primary multifocal LG/G1 pTa
- Primary LG/G1 pTa > 3 cm
- There is uncertainty regarding LG pT1 or HG/G3 pTa < 3 cm
As follows is a Venn diagram for defining intermediate risk disease, noting that NICE 2015, AUA/SUO 2020, NCCN 2021, IBCG, and EAU 2021 definitions of intermediate-risk disease all vary, which also has treatment implications:
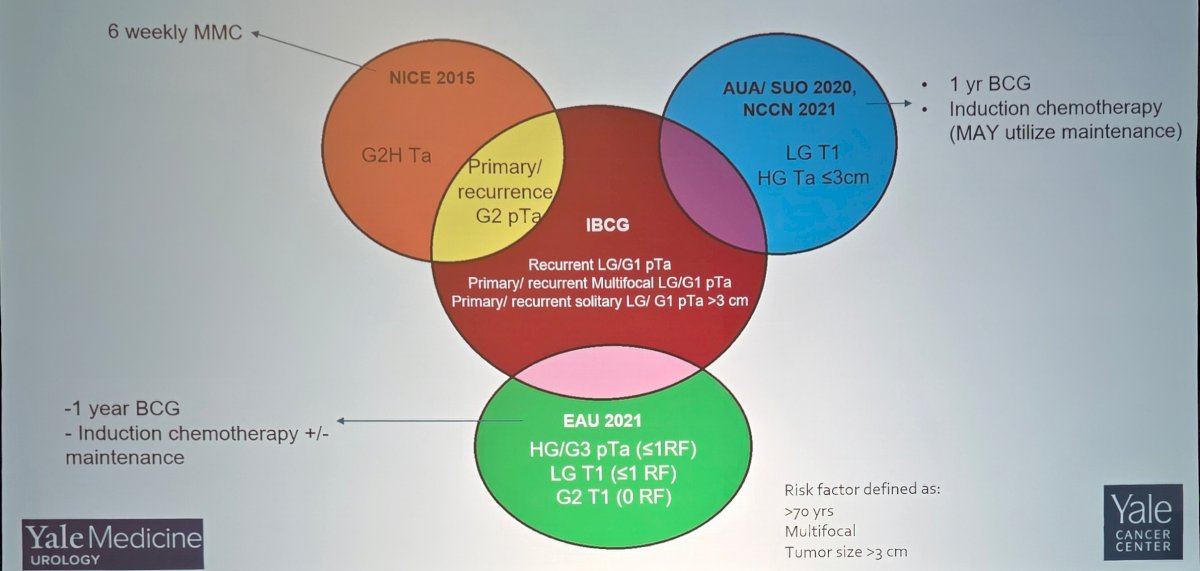
Dr. Tan emphasized how the same patient could be categorized differently depending on the guideline applied—an issue that complicates both clinical decision-making and research comparability.
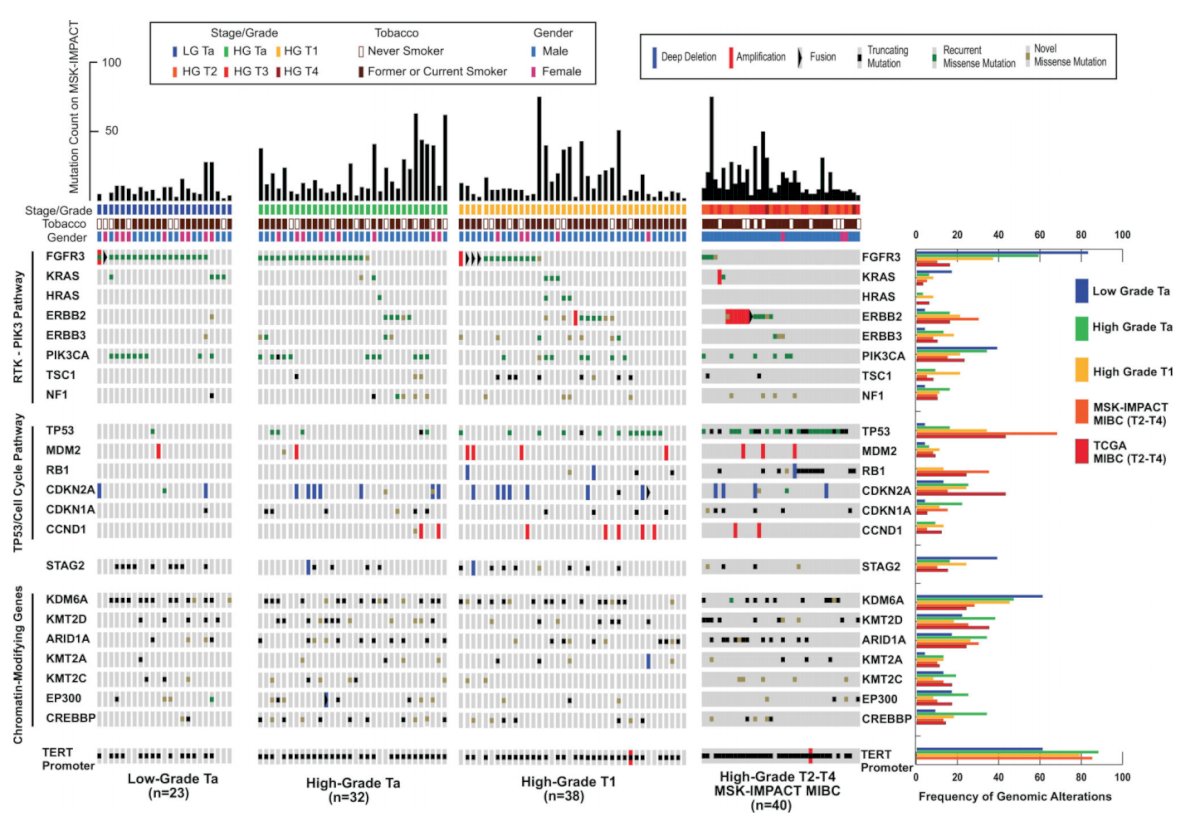
Work from Dr. Pietzak’s group previously assessed pretreatment index tumors and matched germline DNA from 105 patients with non muscle invasive bladder cancer.1 TERT promoter mutations (73%) and chromatin-modifying gene alterations (69%) were highly prevalent across grade and stage, suggesting these events occur early in tumorigenesis. Furthermore, ERBB2 or FGFR3 alterations were also present in 57% of high-grade non muscle invasive bladder cancer tumors in a mutually exclusive pattern. FGFR alterations included 60% of high-grade Ta tumors without CIS compared to 70-80% of patients with low grade Ta tumors. As follows is an overview of the genomic landscape of non muscle invasive bladder cancer by grade and stage, with a comparison to muscle-invasive bladder cancer:
Dr. Tan notes that clinicopathologic parameters are currently the best predictors of response to BCG. Historical data from previous EORTC trials (n = 2,595) suggest that a simple scoring system using the number of tumors, tumor size, prior recurrence rate, T stage, CIS, and grade is able to predict probabilities of disease recurrence and progression.2 The CUETO Scoring Model is derived from 4 trials of 1,062 patients, all treated with BCG.3 A scoring system was calculated with a score of 0 to 16 for recurrence and 0 to 14 for progression, and patients were categorized into 4 groups by score. However, there are limitations to both of these aforementioned historic risk calculators.
Next, Dr. Tan highlighted the International Bladder Cancer Group (IBCG)’s consensus effort to better define and treat the intermediate risk population. The initial publication was in 2014,4 followed by an update in 2022,5 led by Dr. Tan. In the updated definitions and management recommendations for the treatment of intermediate risk non muscle invasive bladder cancer, among intermediate risk (low-grade tumors), the following risk factors should be assessed:
- Tumor size >3 cm
- Multiple tumors
- Early recurrence (<1 year)
- Frequent recurrence (>1/year)
- Failure of previous intravesical treatment
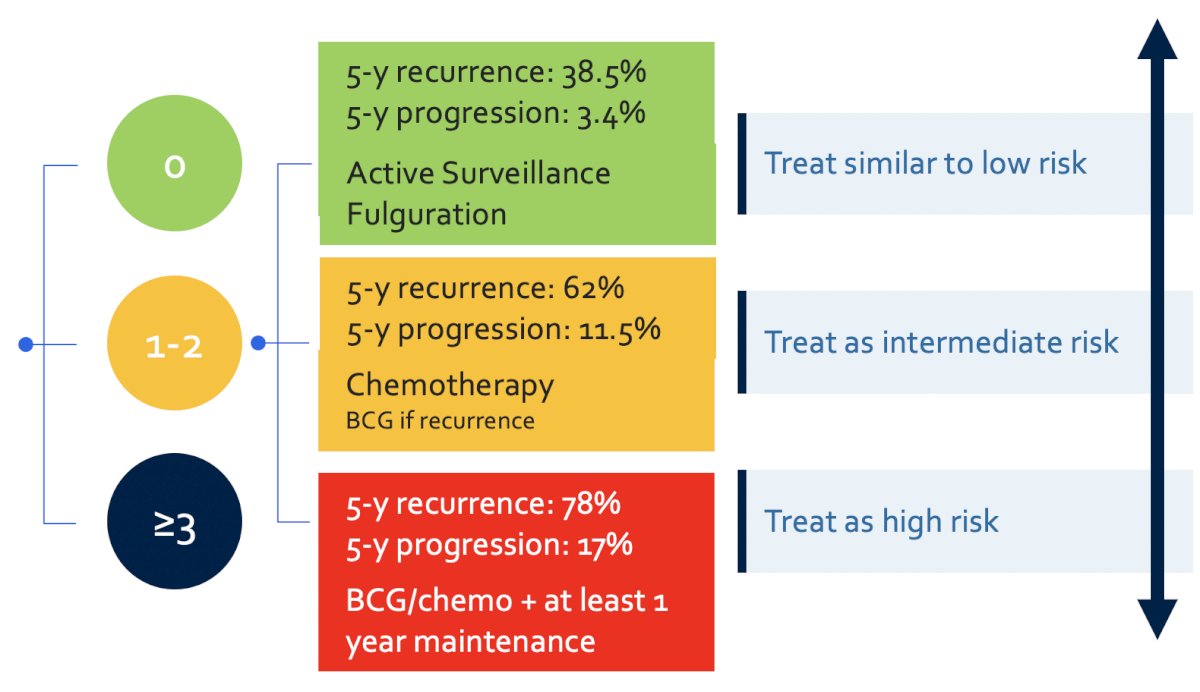
For those patients with none of the above risk factors, they should be treated similarly to those with low-risk disease (no additional treatment). For patients with 1-2 risk factors, they should be treated as intermediate risk disease and thus treated with additional adjuvant induction intravesical chemotherapy (or BCG if prior chemotherapy has been used). For patients with 3+ risk factors, they should be treated as high risk disease with BCG/chemotherapy for at least 1 year, with maintenance therapy:
In 2024, Soria and colleagues6 validated the IBCG intermediate risk grouping across 667 patients treated with adjuvant chemotherapy. Recurrence probability at 3 years varied by IBCG risk:
- IR-low: 29.5%
- IR-intermediate: 36.9%
- IR-high: 67.5%
Progression rates remained low across groups, again reinforcing the recurrence-dominant nature of intermediate risk disease.
In 2023, Dr. Tan and colleagues validated the IBCG intermediate risk scoring system in an active surveillance population,7 a growing paradigm for appropriately selected low-grade tumors. The criteria for active surveillance include:
- Low grade
- ≤5 apparent low grade tumors
- Diameter ≤1 cm
- Absence of gross hematuria
- Negative urinary cytology
In this study of 163 patients, over a median follow-up of 33 months (IQR 21-46), TURBT was performed on 109 patients. At a landmark time point of 24 months, patients with 0 risk factors were over 2-fold more likely to continue active surveillance compared to patients with ≥3 risk factors (59% versus 24%):
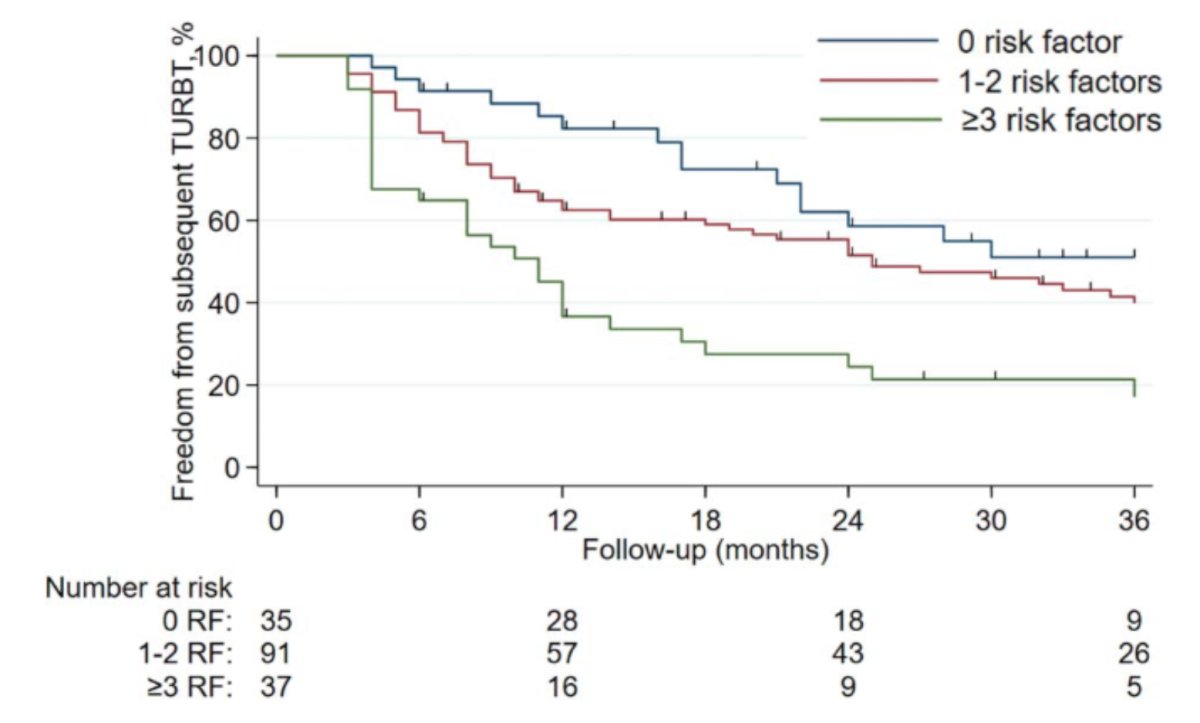
Multivariable Cox regression suggested that the IBCG intermediate risk non muscle invasive bladder cancer scoring system was associated with subsequent TURBT (1-2 risk factors [HR 1.66, 95% CI 0.96-2.90], ≥3 risk factors [HR 3.21, 95% CI: 1.70-6.09, p < 0.001]) after adjusting for age, T stage, and sex.
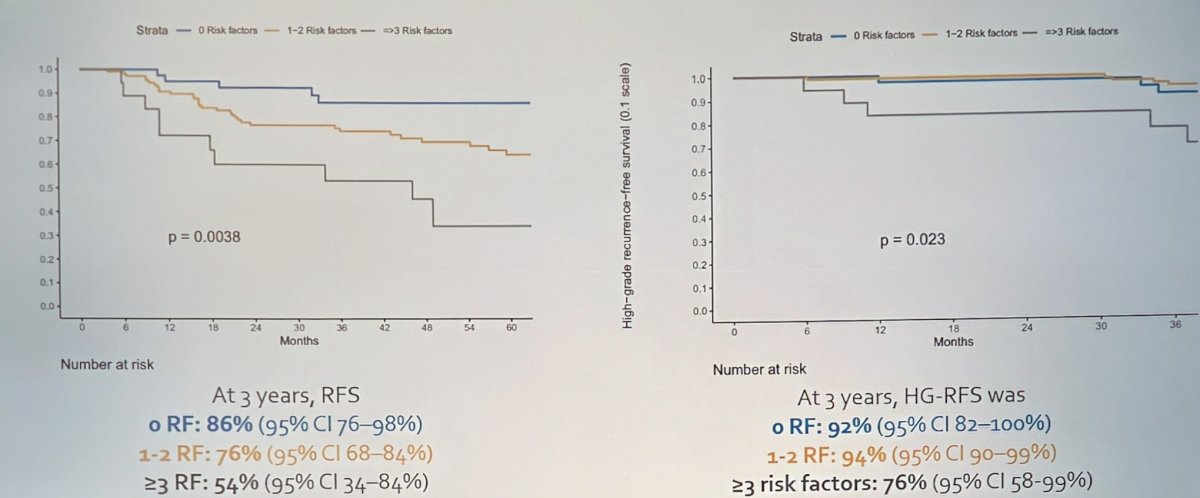
A second active surveillance validation study from Zaurito et al.8 assessed 168 LG Ta patients, over a median follow-up of 30 months, treated with adjuvant chemotherapy or BCG. The 3-year outcomes are as follows
- 3-year recurrence free survival:
- 0 risk factors: 86%
- 1-2 risk factors: 76%
- ≥3 risk factors: 54%
- 3-year high grade recurrence free survival:
- 0 risk factors: 92%
- 1-2 risk factors: 94%
- ≥3 risk factors: 76%
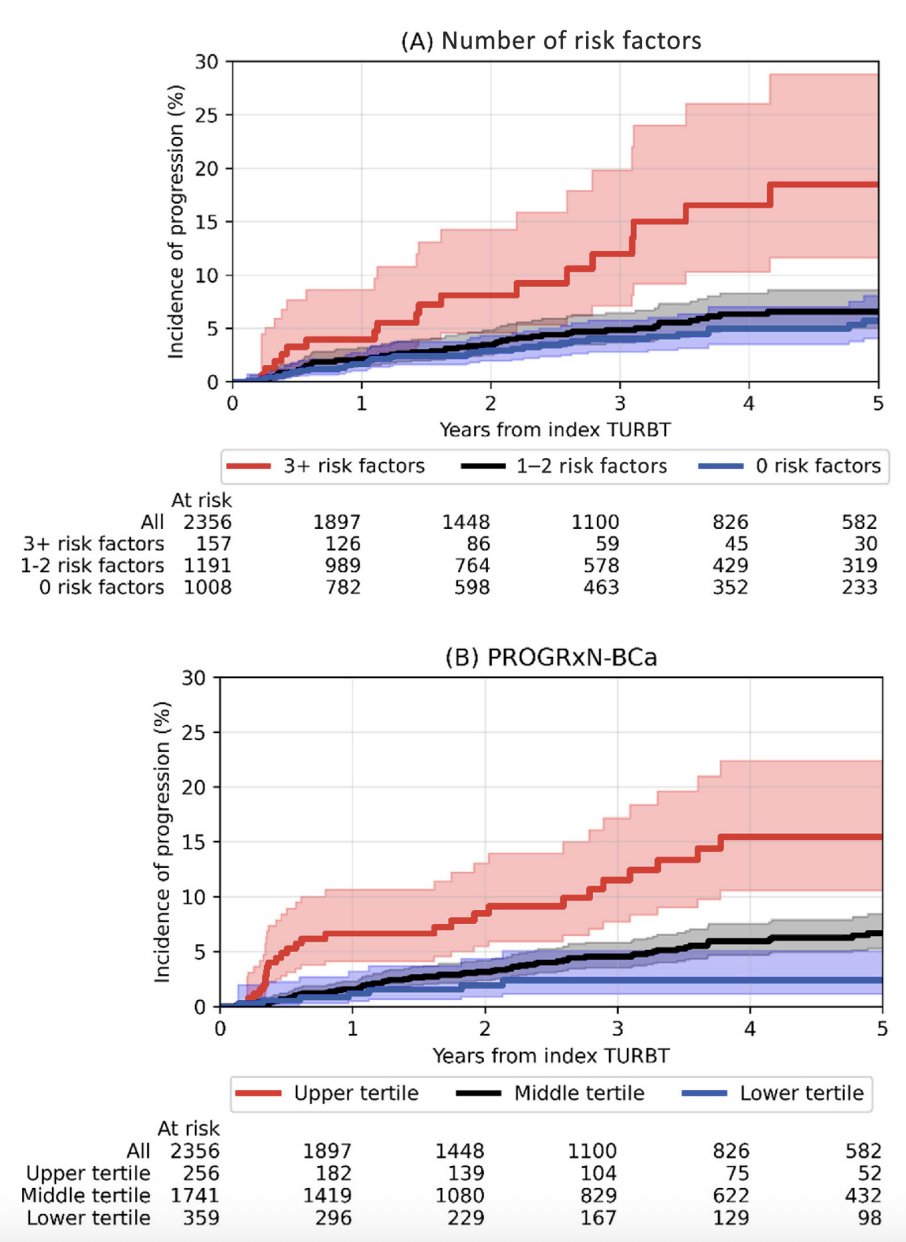
Finally, Kwong and colleagues9 recently published the PROGRxN-BCa model using the WHO 2004/2022 grading system to predict progression risk and improve substratification for non muscle invasive bladder cancer. PROGRxN-BCa was trained using 14 clinicopathological features on 3,324 non muscle invasive bladder cancer patients treated from 2005 to 2022 at four Canadian institutions. External testing was performed on 9,335 patients treated from 2005 to 2023 across 30 North American and European institutions. During a median follow-up of 3.3 years (IQR 1.6-5.8), 1,405 of 12,659 patients progressed. In the external testing cohort, PROGRxN-BCa had significantly higher c-index (0.79, 95% CI 0.77-0.80) and net benefit overall and across different subgroups compared with the EAU risk calculator (0.71, 95% CI 0.70-0.73, p < 0.001). For intermediate risk patients, the IBCG substrata could not distinguish between the groups with 0 and 1-2 risk factors, with 5-year progression risks of 6% (95% CI 4–8%) and 7% (95% CI 5–9%), respectively. However, PROGRxN-BCa separated these patients into distinct risk tertiles:
Dr. Tan concluded his presentation discussing risk stratification for intermediate risk non muscle invasive bladder cancer with the following take home points:
- There is disease heterogeneity requiring better risk stratification
- The risk of recurrence is high, but progression remains low
- We need to redefine patient-centric endpoints
- There is a balancing act between over treatment versus progression risk versus treatment cost versus quality of life
- Risk stratification allows personalized treatment:
- Active surveillance
- Office fulguration
- Adjuvant treatment (chemotherapy versus BCG versus novel therapies)
Presented by: Wei Shen Tan, MD, PhD, FRCS, Yale School of Medicine, New Haven, CT
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
References:
- Pietzak EJ, Bagrodia A, Cha EK, et al. Next-generation sequencing of nonmuscle invasive bladder cancer reveals potential biomarkers and rational therapeutic targets. Eur Urol. 2017 Dec;72(6):952-959.
- Sylvester RJ, van der Meijden APM, Oosterlinck W, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: A combine analysis of 2596 patients from seven EORTC trials. Eur Urol. 2006 Mar;49(3):466-475.
- Fernandez-Gomez J, Madero R, Solsona E, et al. Predicting nonmuscle invasive bladder cancer recurrence and progression in patients treated with bacillus Calmette-Guerin: the CUETO scoring model. J Urol. 2009 Nov;182(5):2195-2203.
- Kamat AM, Witjes JA, Brausi M, et al. Defining and treating the spectrum of intermediate risk nonmuscle invasive bladder cancer. J Urol. 2014 Aug;192(2):305-315.
- Tan WS, Steinberg G, Witjes JA, et al. Intermediate-risk non-muscle invasive bladder cancer: Updated Consensus Definition and Management Recommendations from the International Bladder Cancer Group. Eur Urol Onc. 2022 Oct;5(5):505-516.
- Soria F, Rosazza M, Livoti S, et al. Clinical validation of the intermediate-risk non-muscle-invasive bladder cancer scoring system and substratification model proposed by the International Bladder Cancer Group: A multicenter Young Academic Urologists Urothelial Working Group Collaboration. Eur Urol Oncol. 2024 Dec;7(6):1497-1503.
- Tan WS, Contieri R, Buffi NM, et al. International Bladder Cancer Group Intermediate-risk nonmuscle-invasive bladder cancer scoring system predicts outcomes of patients on active surveillance. J Urol. 2023 Nov;210(5):763-770.
- Zaurito P, Scilipoti P, Longoni M, et al. Identifying optimal candidates for active surveillance in low-grade intermediate-risk non-muscle invasive bladder cancer. World J Urol. 2024 Dec 30;43(1):52.
- Kwong JCC, Al-Daqqaq Z, Chelliahpillai Y, et al. Development and International Evaluation of an Artificial Intelligence-based Model (PROGRxN-BCa) Using the World Health Organization 2004/2022 Grading System to Predict Progression Risk and Improve Substratification for Non-muscle-invasive Bladder Cancer. Eur Urol. 2025 Oct 7 [Epub ahead of print].