(UroToday.com) The 2025 SUO annual meeting featured a bladder cancer session and a presentation by Dr. Vignesh Packiam discussing trial updates in intermediate risk non muscle invasive bladder cancer. The American Urological Association defines intermediate risk disease as the following:
- Recurrence within 1 year, low grade Ta
- Solitary low grade Ta > 3cm
- Low grade Ta, multifocal
- High grade Ta, <= 3cm
- Low grade T1
From a practical standpoing, Dr. Packiam notes that this is mostly LG Ta (unless < 3 cm, unifocal, non-recurrent), LG T1 (rare), and favorable HG Ta (< 3 cm, unifocal, non-recurrent). The AUA guidelines suggest that in an intermediate risk patient, a clinician should consider administration of a six week course of induction intravesical chemotherapy (Moderate Recommendation; Evidence Strength: Grade B). However, during the BCG shortage, the SUO suggested that intravesical chemotherapy should be used as the first-line option for these patients. Importantly, the literature suggests that mitomycin C is not as efficacious as BCG, with 2 year recurrence free survival rates of ~60% and up to 11% of patients discontinuing treatment.
In 2025, UGN-102 (Zusduri) was FDA approved on the basis of data from ATLAS1 and ENVISION.2 ENVISION is an ongoing, multinational, single-arm, phase III trial in patients with a biopsy-proven recurrence of untreated low grade intermediate risk non muscle invasive bladder cancer. Eligible patients received 6 weekly intravesical instillations of UGN-102 and were evaluated at 3 months. Of 240 patients enrolled, the 3-month complete response rate was 79.2%, with an 82.3% (95% CI 74–86%) probability of a maintained response at 12 months. The UTOPIA trial is a phase 3, single arm study of UGN-103 (a shorter manufacturing process and a simplified reconstitution procedure compared to UGN-102), for treatment of low grade intermediate risk non muscle invasive bladder cancer. This study was designed to evaluate the efficacy and safety of UGN-103 as a primary chemoablative therapy in a global study of approximately 55 sites in the United States and Europe. Enrolment is complete (n = 99), with a primary endpoint of complete response rate, and a key secondary endpoint of durability of response. Based on a November 6, 2025 press release, the 3 month complete response rate was 77.8%, in line with that seen in ENVISION.
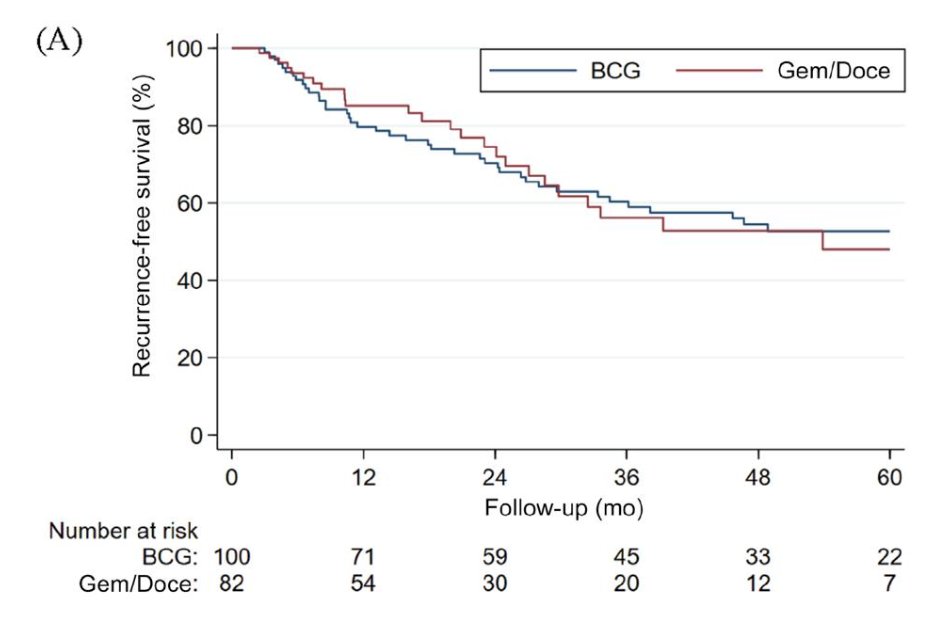
In a multicenter assessment of gemcitabine + docetaxel in intermediate risk disease, Tan et al. evaluated oncological outcomes for 182 patients treated with BCG (n = 100) or intravesical sequential gemcitabine and docetaxel (n = 82).3 Notably, recurrence rates were similar in the two treatment groups (HR 1.06, 95% CI 0.65-1.73; p = 0.8). The 2 year recurrence free survival rate for BCG was 70% versus 75% for gemcitabine + docetaxel:
The NDV-001 trial is evaluating the safety and efficacy of intravesical sustained release gemcitabine docetaxel combination (NDV-01) in high risk non muscle invasive bladder cancer. This study is an open-label, single-arm, single center study in high risk non muscle invasive bladder cancer, including patients with high grade disease with CIS, Ta, or T1 tumors, and could be either BCG naïve, BCG unresponsive, intolerant, or experienced patients. There will be 70 patients receiving intravesical NDV-01 with 6 bi-weekly instillations, and maintenance of monthly instillations. Follow-up will include urine cytology, cystoscopy, upper tract imaging, and TURBT if necessary. The oncological outcomes include:
- High grade recurrence free survival
- Progression free survival
- Cystectomy free survival
- Metastasis free survival
- Cancer specific survival
- Overall survival

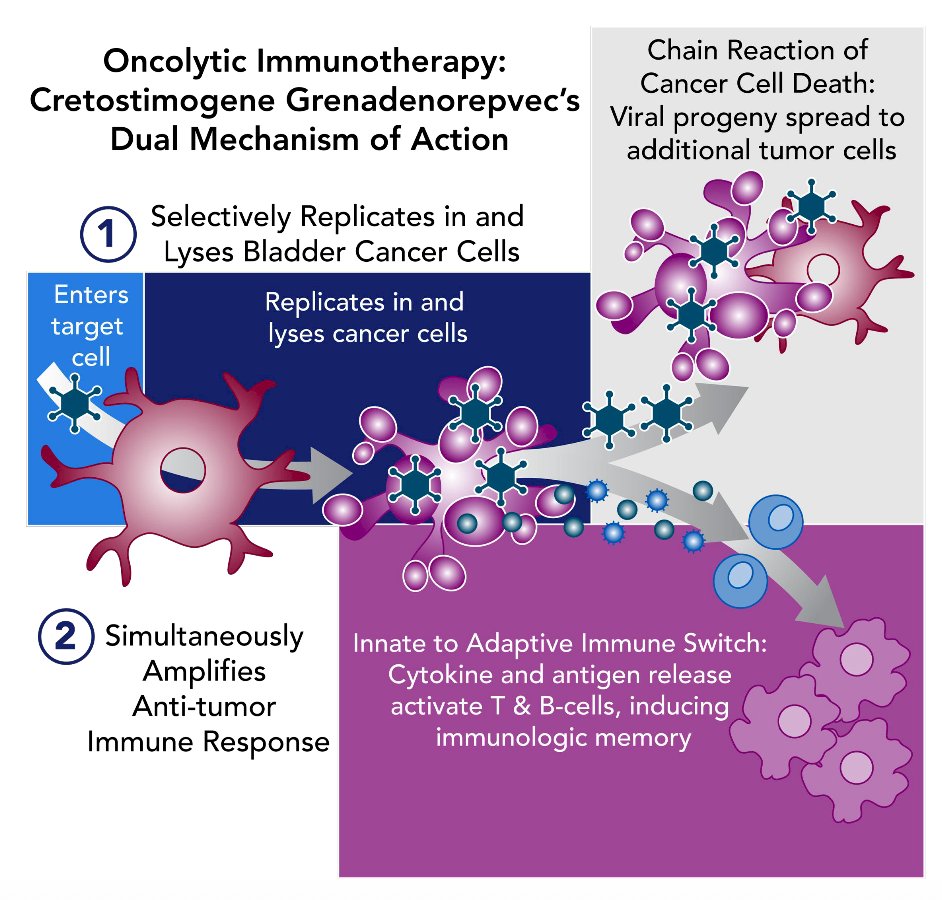
PIVOT-006 is an ongoing phase 3, randomized study of adjuvant intravesical cretostimogene grenadenorepvec versus surveillance for the treatment of intermediate risk non-muscle invasive bladder cancer. Cretostimogene grenadenorepvec, an oncolytic immunotherapy, selectively replicates in and lyses cancer cells with Rb-E2F pathway alterations, releasing antigens that initiate antitumor immune activation, further amplified by the GM-CSF transgene:
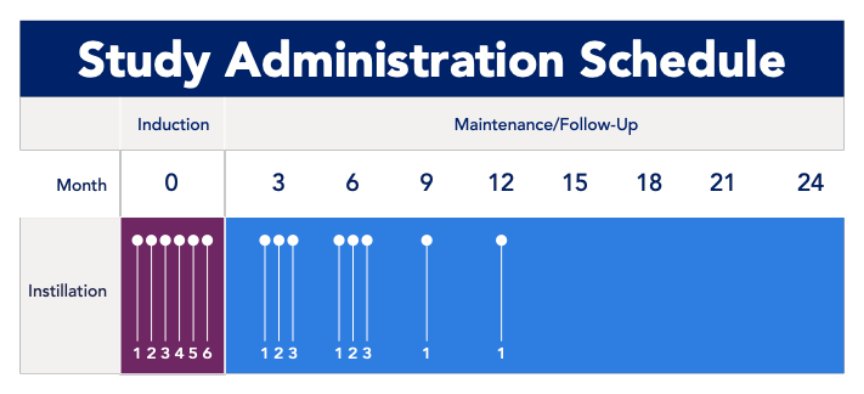
Eligibility criteria for PIVOT-006 include histologically confirmed intermediate risk non muscle invasive bladder cancer diagnosis within 90 days of randomization, as defined by AUA/SUO guidelines. Stratification factors include receipt of single-dose perioperative chemotherapy and tumor grade. Patients (n ~ 364) will be randomized 1:1 to undergo surveillance or to receive intravesical cretostimogene following TURBT. If intermediate risk non muscle invasive bladder cancer recurrence is noted in the surveillance arm, patients will be eligible to receive intravesical cretostimogene. Intravesical cretostimogene is administered in combination with DDM, an excipient that enhances adenoviral delivery, for 6 weekly doses during the induction phase, followed by 3 weekly maintenance cycles at months 3 and 6, and culminating in a single intravesical dose at months 9 and 12. Primary disease assessments include serial cystoscopy, urine cytology, axial imaging, and centralized review of pathologic samples:
The primary endpoint is recurrence free survival, and secondary outcomes include safety, tolerability, progression free survival, and time to next intervention. Exploratory outcome measures include health-related quality of life and biomarker analyses. 90+ clinical sites, including diverse representations across private practice and academic institutions, were selected for the trial. Enrollment for PIVOT-006 is complete.
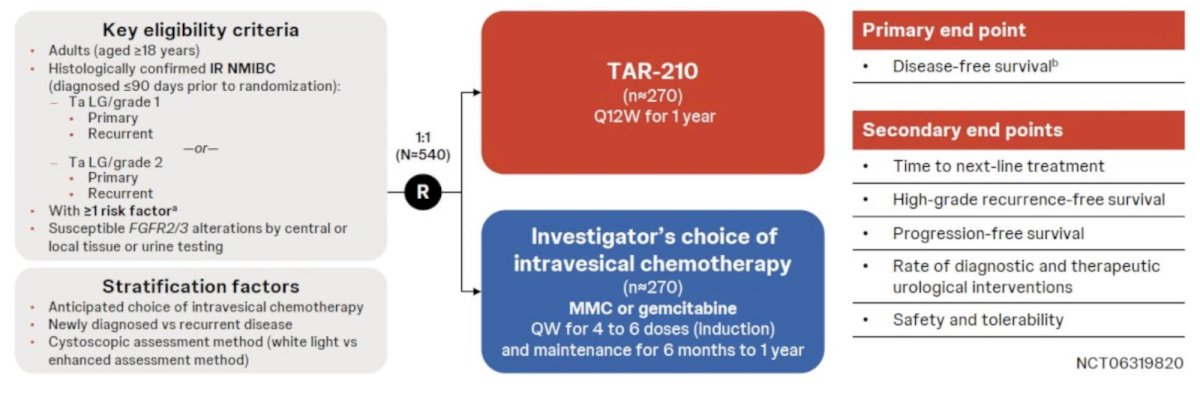
MoonRISe-1 is an open-label, multicenter, randomized phase III trial designed to evaluate the efficacy and safety of TAR-210 versus intravesical chemotherapy in patients with histologically confirmed, FGFR-altered, low-grade, intermediate-risk non muscle invasive bladder cancer (n = 540). Evaluation of FGFR2/3 alteration status is performed using central or local tissue or urine testing. Eligible participants will undergo 1:1 randomization to TAR-210 every 12 weeks for one year versus investigator’s choice of intravesical chemotherapy (mitomycin or gemcitabine) every week for 4–6 doses (induction), followed by maintenance for 6 months to 1 year. The primary endpoint is disease-free survival, with secondary endpoints of:
- Time to next-line treatment
- High-grade recurrence-free survival
- Progression-free survival
- Rate of diagnostic and therapeutic urological interventions
- Safety and tolerability
ABLE-32 is an ongoing, open-label, randomized, controlled, phase IIIb study to evaluate the efficacy of nadofaragene firadenovec administered every 3 months versus observation in participants with intermediate-risk non muscle-invasive bladder cancer. Eligible patients will be randomized to:
- Nadofaragene firadenovec 75 mL (3 × 1011 vp/mL) instilled quarterly; up to 8 intravesical instillations
- Observation
- Patients in the control arm may cross over at recurrence of intermediate-risk disease <24 months
- Participants will be followed for up to 60 months based on the surveillance schedule of the AUA/SUO guidelines (quarterly) over the 24-month treatment period
Approximately 454 participants will be enrolled in ABLE-32. An interim analysis will evaluate early stopping, and if the decision is taken to continue the trial, a sample size reassessment will be performed to evaluate trial population expansion:
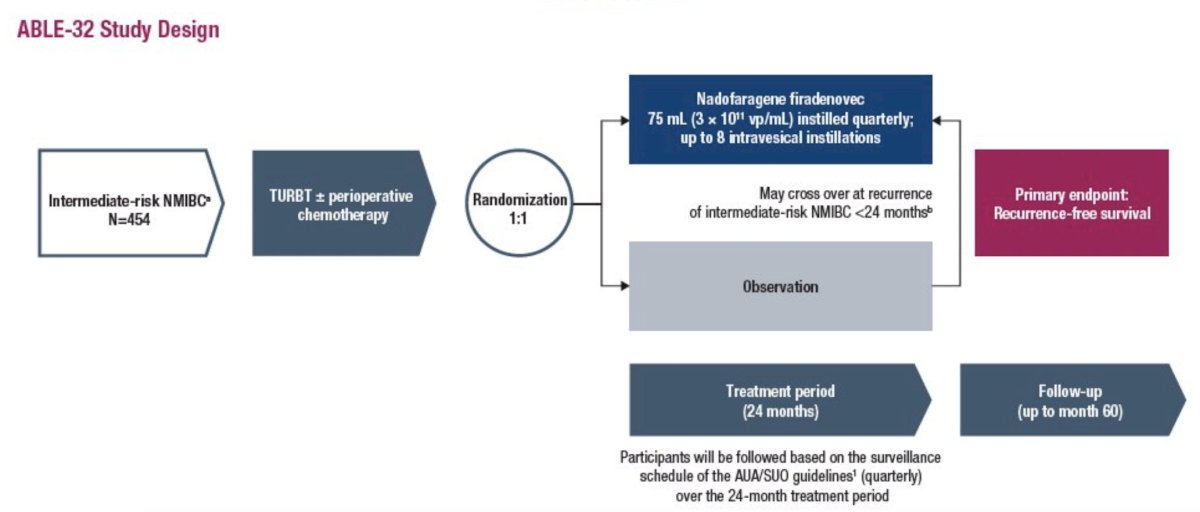
The primary endpoint is recurrence free survival, defined as the time from the date of randomization to first documented recurrence (low-, intermediate-, or high-risk) or progression (high-risk or muscle-invasive) or death (due to any cause), whichever occurs first during the 24-month treatment period.
SURF-302 is an ongoing phase 2 trial (n = 90) assessing the efficacy and safety of an oral FGFR3 inhibitor in FGFR3 activating gene mutated low grade intermediate risk non muscle invasive bladder cancer patients. There will be 30 patients randomized to the 50 mg daily dose and 30 patients randomized to the 60 mg daily dose, with a primary endpoint of complete response at 3 months (and will continue on study treatment). The cohort 3 dose is yet to be determined (n = 30). Secondary endpoints include time to recurrence, median duration of response, recurrence free survival, progression free survival, safety, and tolerability.
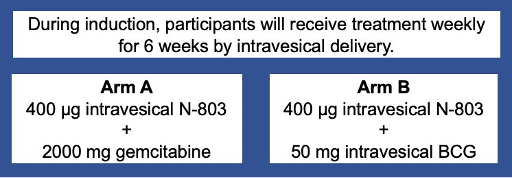
RESQ132A is a phase 2 trial of intravesical gemcitabine + N-803 versus intravesical N-803 and BCG for intermediate risk non muscle invasive papillary bladder cancer. In the ResQ312A trial, the efficacy of N-803 plus BCG will be compared to N-803 + gemcitabine in participants with BCG-naïve intermediate-risk papillary NMIBC. Adult participants with histologically-confirmed BCG-naïve intermediate-risk papillary Ta/T1 NMIBC will be enrolled into either Arm A or B. Up to 10 participants will be enrolled in each arm:
The initial response assessment will be at 3 months. The second treatment period would commence at the end of month 3 and continue through month 15, with treatment depending upon the month 3 response:
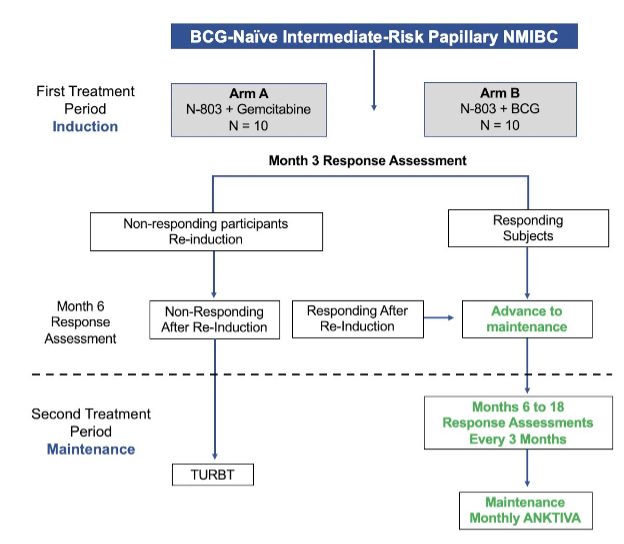
The primary endpoint is the complete response (absence of any grade papillary disease or CIS disease) rate at month 3 as determined by assessment of cystoscopy, cytology, and biopsy, summarized by the number and percent and exact 95% CI using the Clopper-Pearson method.
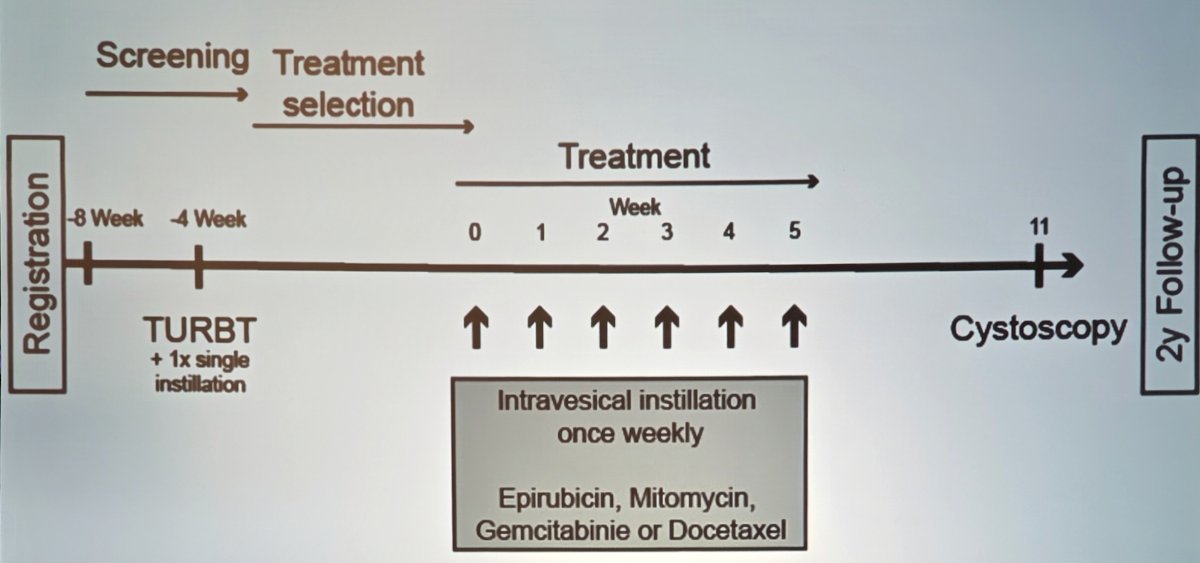
In Europe, the COBRA trial is ongoing and assessing chemoablation or bladder resection with adjuvant chemotherapy in recurrence non muscle invasive bladder cancer. Patients receive 40 mg/40 mL of intravesical mitomycin C three times a week for 2 weeks, with a 2 hour dwell time. The GAIN-INST trial is also ongoing, assessing intravesical instillation (either epirubicin, mitomycin, gemcitabine, or docetaxel) once weekly followed by cystoscopy, with a 2 year follow-up:
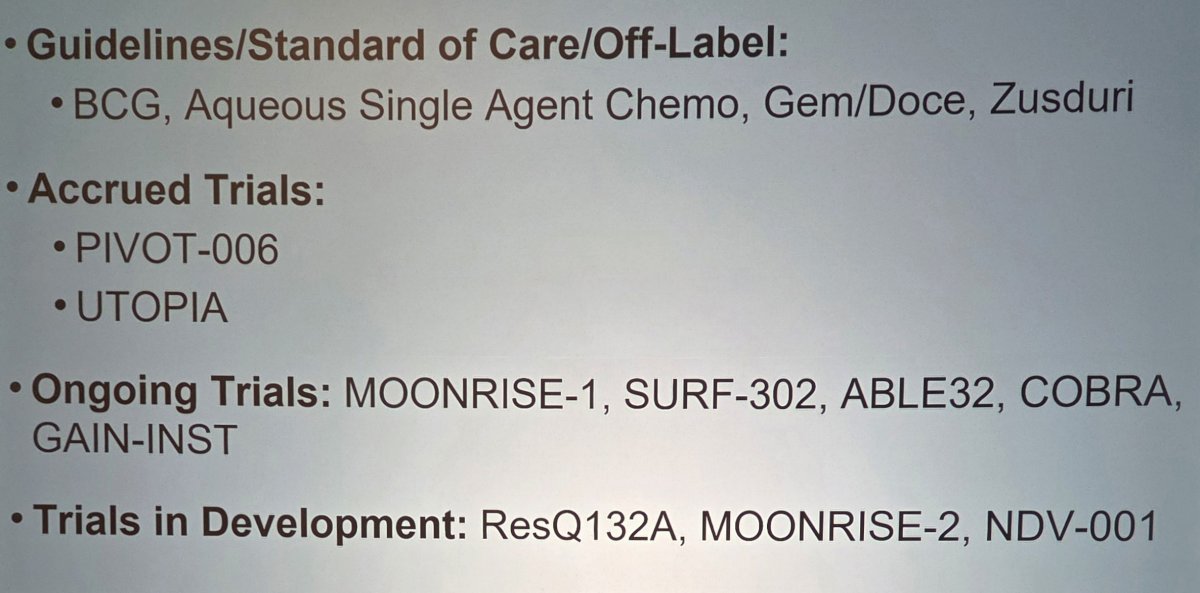
Dr. Packiam concluded his presentation discussing trial updates in intermediate risk non muscle invasive bladder cancer by highlighting the current landscape:
Presented by: Vignesh Packiam, MD, Cancer Institute of New Jersey, New Brunswick, NJ
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
References:
- Prasad SM, Huang WC, Shore ND, et al. Treatment of low-grade intermediate-risk nonmuscle-invasive bladder cancer with UGN-102 +/- transurethral resection of bladder tumor compared to transurethral resection of bladder tumor monotherapy: A randomized, controlled, phase 3 trial (ATLAS). J Urol. 2023 Oct;210(4):619-629.
- Prasad SM, Shishkov D, Vladimirov Mihaylov N, et al. Primary Chemoablation of Recurrent Low-Grade Intermediate-Risk Nonmuscle-Invasive Bladder Cancer with UGN-102: A Single-Arm, Open-Label, Phase 3 Trial (ENVISION). J Urol. 2025 Feb;213(2):205-216.
- Tan WS, McElree IM, Davaro F, et al. Sequential intravesical gemcitabine and docetaxel is an alternative to Bacillus Calmette-Guerin for the treatment of intermediate-risk non-muscle invasive bladder cancer. Eur Urol Oncol. 2023 Oct;6(5):531-534.