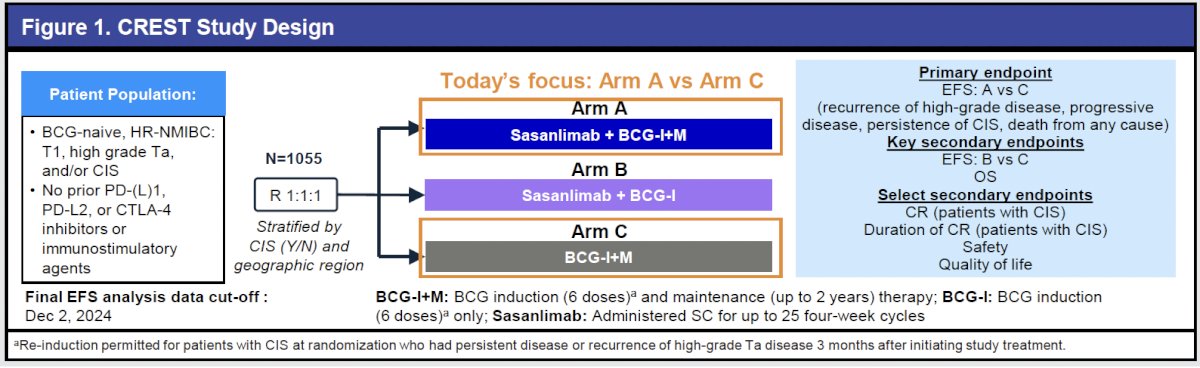
(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting featured a bladder cancer poster session during which Dr. Gary Steinberg presented results from the CREST study, a large, global, phase III randomized trial evaluating sasanlimab, a subcutaneously administered PD-1 inhibitor, in combination with BCG induction and maintenance (BCG-I+M) in BCG-naive, high-risk NMIBC.
Standard-of-care management for high-risk NMIBC consists of TURBT followed by BCG-I+M;1,2 however, approximately 40% of patients experience disease recurrence or progression at 24 months.3 As patients who develop BCG-unresponsive disease derive little benefit from further BCG treatment and have limited bladder-sparing options,2,4 delaying or preventing the development of BCG-unresponsiveness represents a major therapeutic goal.
The biologic rationale for combining PD-1 inhibition with BCG is supported by increased PD-L1 expression following BCG exposure.5-7 Sasanlimab has demonstrated durable antitumor activity and a manageable safety profile across advanced solid tumors.8,9 The CREST study therefore sought to evaluate whether adding sasanlimab to BCG could improve outcomes in the frontline management of high-risk NMIBC.
CREST randomized 1,055 patients 1:1:1 to receive:
- Sasanlimab plus BCG-I+M (Arm A)
- Sasanlimab plus BCG induction only (Arm B)
- BCG-I+M alone (Arm C)
BCG-unresponsive disease was defined per FDA guidance.10 The primary endpoint was event-free survival (EFS) for Arm A versus Arm C, with key secondary endpoints including:
- EFS for Arm B vs Arm C
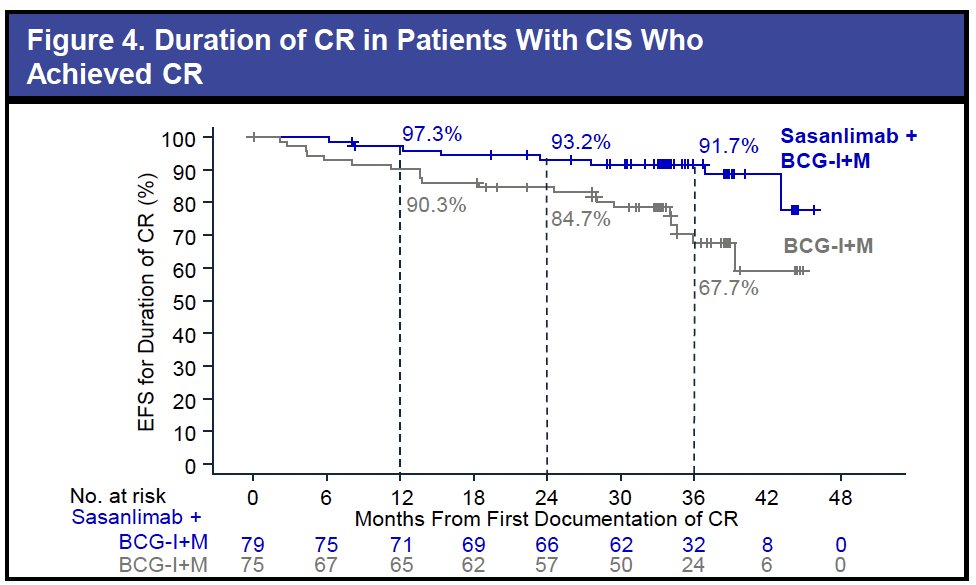
- Complete response (CR) among patients with CIS
- Duration of CR
- Overall survival
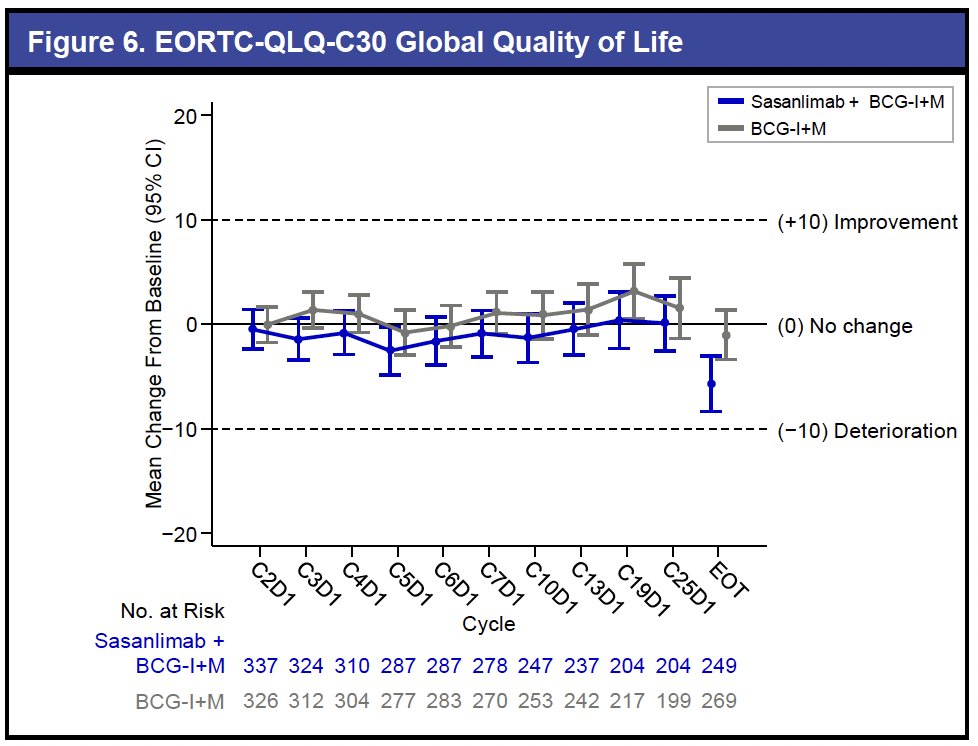
- Quality of life
- Safety.
The baseline demographic and disease characteristics have been reported previously.11 The median age was 67 years, most patients were men (82%), and high-grade T1 disease comprised 54% of cases. CIS with or without papillary tumors was present in roughly one-quarter of patients (25.5%).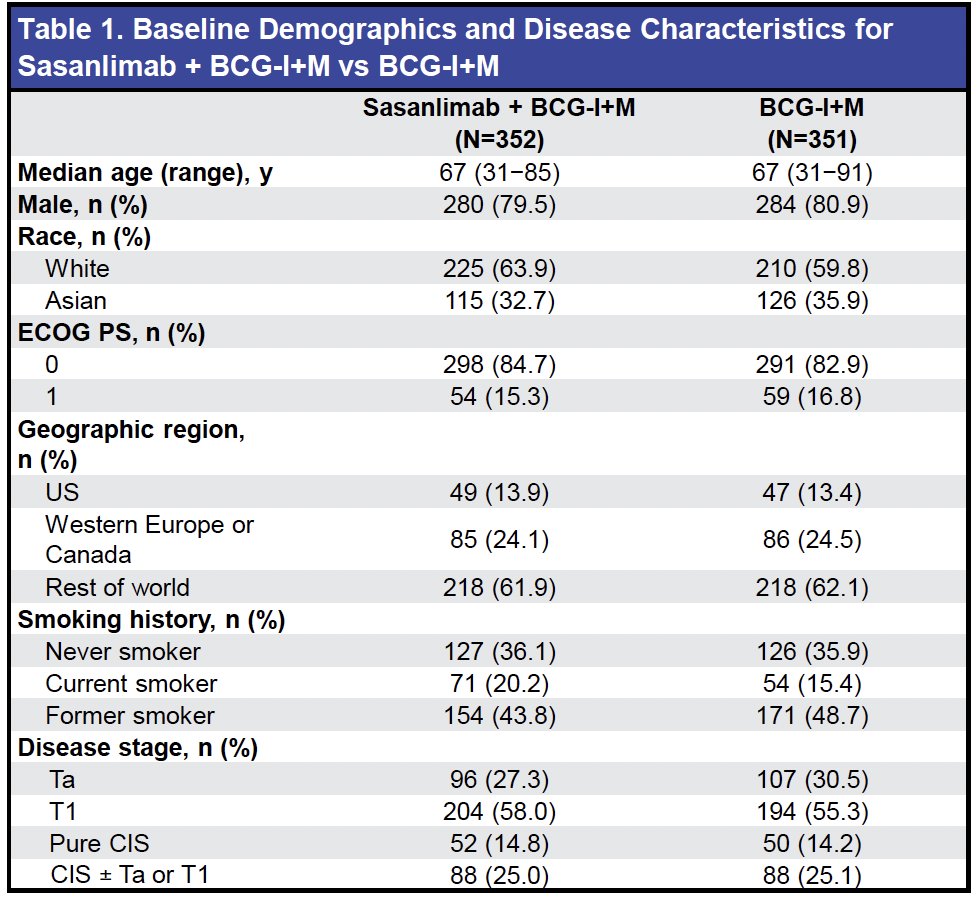
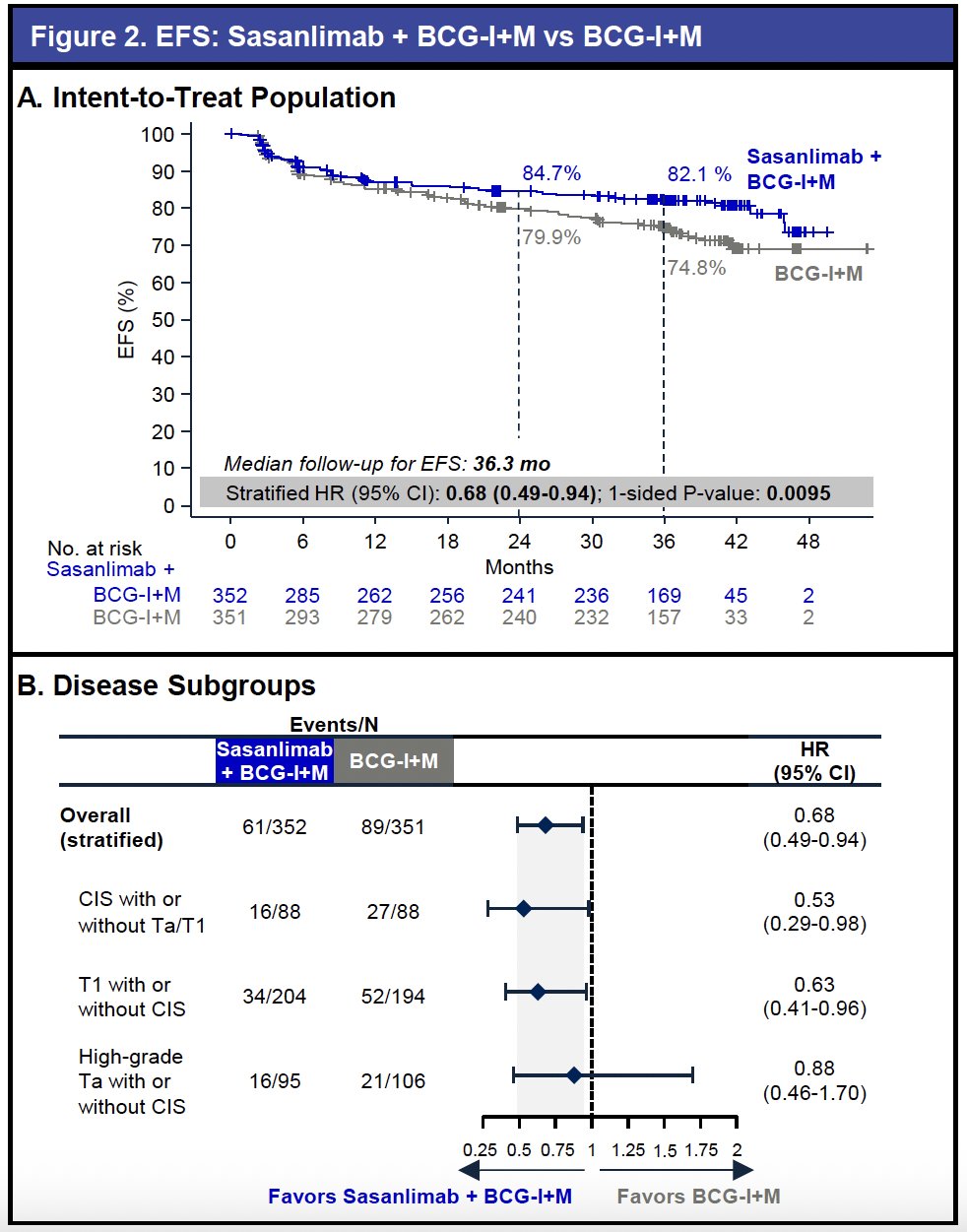
The primary endpoint was met. At a median follow-up of 36.3 months, sasanlimab plus BCG-I+M significantly prolonged EFS compared with BCG-I+M alone (stratified HR: 0.68; 95% CI: 0.49–0.94). There was a 7.3% reduction in the EFS rate at three years with the addition of sasanlimab.
Recurrence of high-grade disease was reduced by more than 50% (7.4% vs 15.1%). A consistent benefit was observed across key clinical subgroups, including CIS-containing, T1, and high-grade Ta disease.
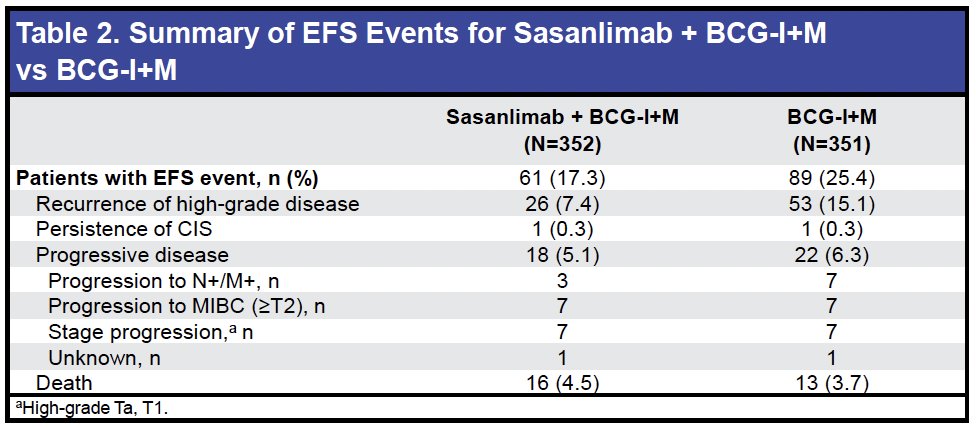
Overall survival results remain immature at a median follow-up of 40.9 months, with few deaths reported and no meaningful differences observed between arms at this stage.

Among patients with CIS, the CR rate at any time was 89.8% with sasanlimab plus BCG-I+M and 85.2% with BCG-I+M. The probability of maintaining a CR at 36 months was high in both groups, including 92% for sasanlimab plus BCG-I+M.
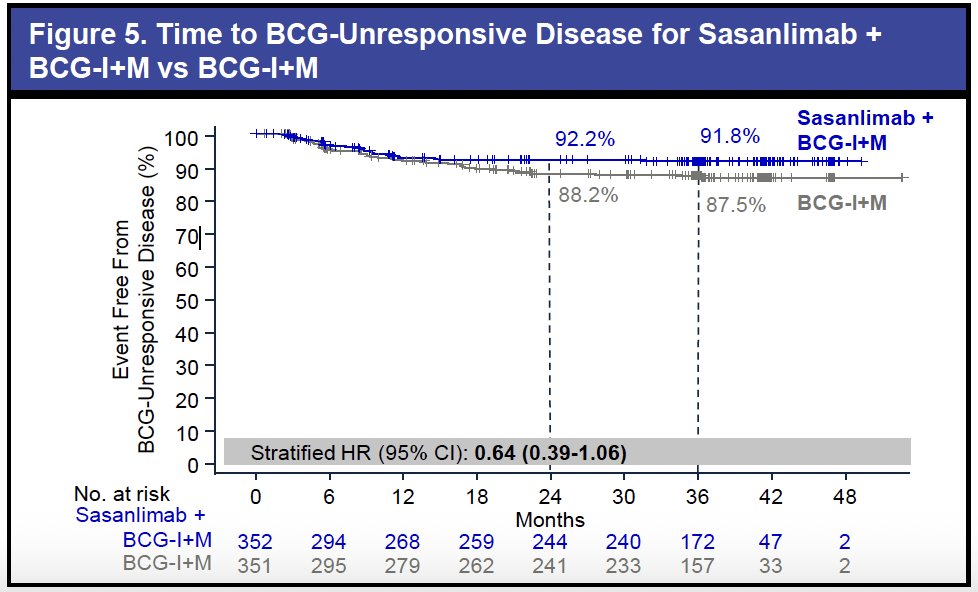
An exploratory analysis assessed the development of BCG-unresponsive disease. A lower proportion of patients in the sasanlimab plus BCG-I+M arm developed BCG-unresponsive disease (7.1% vs 11.1%), and time to BCG-unresponsiveness numerically favored the combination (stratified HR: 0.64; 95% CI: 0.39–1.06). These findings suggest that sasanlimab may delay progression to BCG-unresponsive disease, a clinical milestone associated with increased treatment burden and limited bladder-sparing options.
Quality-of-life outcomes were maintained with the combination, with high completion rates exceeding 84% through end of treatment.
The safety findings were consistent with the established profiles of sasanlimab and BCG. There were no treatment-related deaths. Treatment-related adverse events (TRAEs) were observed in 58% and 64% of patients in the sasanlimab plus BCG-I+M and BCG-I+M arms, respectively. The most common TRAEs in both arms were dysuria (29–32%), pollakiuria (19–23%), and hematuria (17%).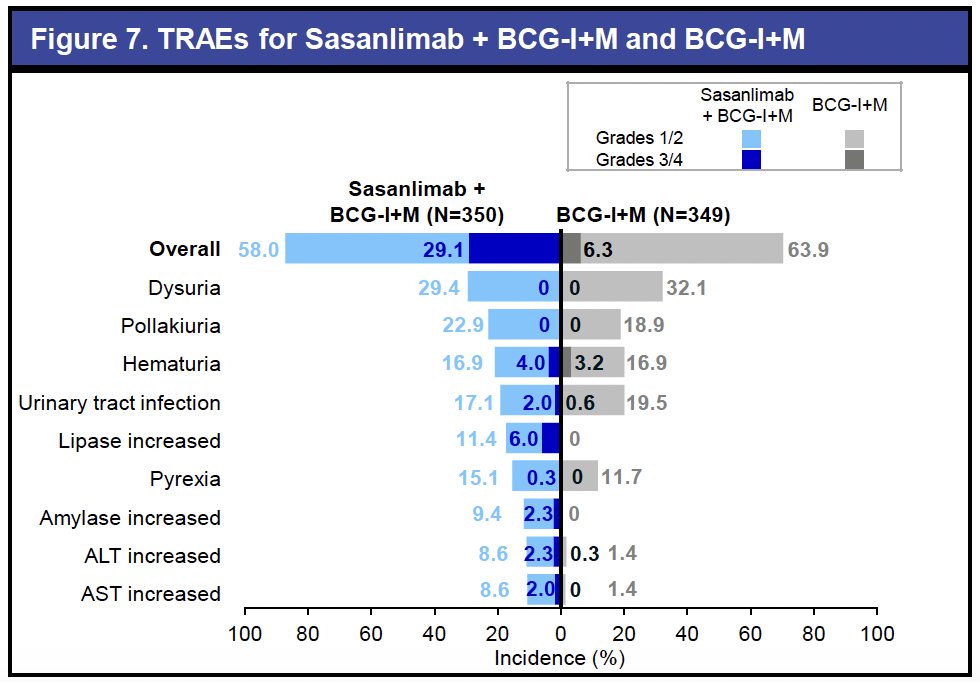
Immune-related adverse events occurred at rates comparable to prior PD-1 inhibitor experience, and the combination did not substantially increase their incidence or severity.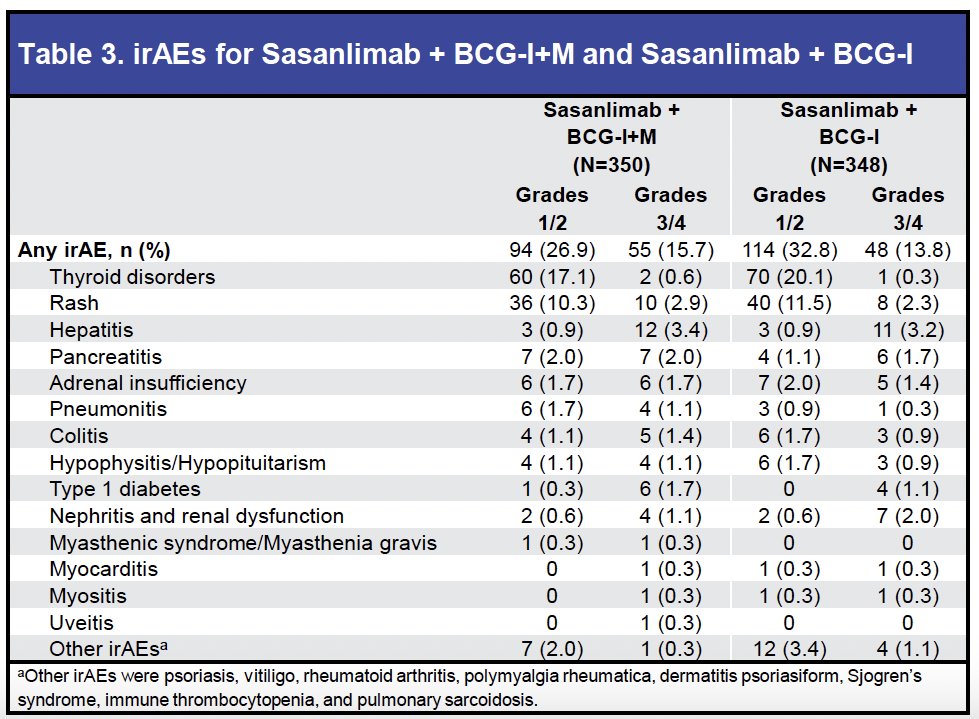
Dr. Steinberg concluded as follows:
- The CREST study is the first to show a statistically significant improvement in event-free survival with sasanlimab plus BCG induction and maintenance, compared to BCG induction and maintenance alone in BCG-naive, high-risk NMIBC
- The addition of sasanlimab delayed the development of BCG-unresponsive disease and may reduce treatment burden by postponing subsequent anticancer therapies
- The safety profile of the combination was consistent with known profiles for each agent
- Sasanlimab plus BCG has the potential to shift clinical decision-making and redefine the treatment paradigm for high-risk NMIBC
Presented by: Gary Steinberg, MD, Professor, Department of Urology, Rush University Medical Center, Chicago, IL
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, December 2nd–5th, 2025
Related content: Subgroup Findings from CREST Trial in High-Risk Bladder Cancer - Gary Steinberg
- Holzbeierlein JM, Meng MV, Chang SS, et al. Diagnosis and treatment of non-muscle invasive bladder cancer. J Urol. 2024; 211:533-538.
- Gontero P, Sylvester R, Kamat AM, et al. Management of high-risk non–muscle-invasive bladder cancer. Eur Urol. 2024; 86:531-549.
- Kamat AM, Sylvester RJ, Bohle A, et al. Predicting risk of progression in non-muscle-invasive bladder cancer: A decision tool. J Clin Oncol. 2016; 34:1935-1944.
- Alhunaidi O, Zlotta AR. High-risk non–muscle-invasive bladder cancer: Current management and future directions. Ecancermedicalscience. 2019; 13:905.
- Hashizume A, Fukumoto K, Sakamoto N, et al. BCG induces PD-L1 expression in bladder cancer cells. Oncotarget. 2018; 9:34066-34078.
- Maas M, Stevenson S, Laird A, et al. Mechanisms of immune modulation following BCG therapy. Cancers (Basel). 2024; 16:1356.
- Wang Y, Liu J, Huang Y, et al. PD-L1 expression and immune activation after BCG instillation. Onco Targets Ther. 2018; 11:2891-2899.
- Johnson ML, Cho BC, Luft A, et al. A phase 1 study of sasanlimab in advanced solid tumors. JAMA Oncol. 2019; 5:999-1007.
- Cho BC, Powell C, Wang Y, et al. Safety and efficacy of sasanlimab in early-phase trials. Ann Oncol. 2020; 31(suppl 4):S721.
- U.S. Food and Drug Administration. BCG-unresponsive non-muscle-invasive bladder cancer: Developing drugs and biologics. 2025.
- Shore ND, Powles T, Bedke J, et al. Sasanlimab plus BCG in BCG-naive high-risk NMIBC: Primary analysis of the CREST trial. Nat Med. 2025; 31:2806-2814.