During the 2025 SUO Annual Meeting, Dr. Matthew Galsky delivered a state-of-the-art lecture discussing how circulating tumor DNA (ctDNA) is reshaping perioperative management of muscle-invasive bladder cancer (MIBC).
At the 2025 SUO Annual Meeting, Dr. Matthew Galsky delivered a comprehensive overview on the emerging role of circulating tumor DNA (ctDNA) for minimal residual disease (MRD) assessment in muscle-invasive bladder cancer (MIBC). His talk centered on how ctDNA can be applied to solve a longstanding and clinically consequential problem in perioperative bladder cancer management: identifying which patients need adjuvant therapy—and which do not.
In 2025, Dr. Galsky noted that we can draw the following conclusions regarding ctDNA in this setting:
- ctDNA tells us who needs adjuvant therapy
- ctDNA may tell us who does not need adjuvant therapy
- ctDNA does not currently identify who does not need neoadjuvant therapy
The historical progression of ctDNA development is as follows:
- 1948: detection of cell-free DNA in human plasma
- 1977: identification of higher cfDNA concentrations in patients with cancer
- 1990s–2000s: emergence of tumor-specific mutations in plasma
These advances culminated in the 2008 demonstration that ctDNA can track tumor dynamics in real time. This paved the way for modern tumor-informed assays capable of detecting MRD with high sensitivity.
Tumor-Informed MRD Testing: Concept and PromiseTumor resection provides the ‘genomic fingerprint’. ctDNA levels can be measured post-surgery to detect residual disease, and ctDNA dynamics can be monitored during and after therapy. This approach has reshaped perioperative trials, enabling biologically informed endpoints beyond traditional imaging.
Adjuvant Immunotherapy Trials: IMvigor010, AMBASSADOR, CheckMate 274
Dr. Galsky reviewed the three major adjuvant PD-1/PD-L1 inhibitor trials in MIBC:
- IMvigor010 (Atezolizumab vs Observation)1
- Did not meet its primary endpoint (DFS).
- AMBASSADOR (Pembrolizumab vs Observation)2
- Met co-primary endpoints of DFS and OS.
- CheckMate 274 (Nivolumab vs Placebo)3
- Met the primary endpoint of DFS in both the ITT and PD-L1 ≥1% cohorts.
- Resulted in regulatory approval of adjuvant nivolumab.
These divergent outcomes raised a central question: How do we identify which patients truly benefit from adjuvant therapy?
The “Double Biomarker Dilemma”Two important questions arise:
- Who needs treatment?
- Who benefits from treatment?
DFS curves from CheckMate 274 illustrate the challenge:
- Some patients who clearly “needed” adjuvant therapy did not benefit
- Others who “needed and benefited” represent the ideal treatment candidates
- A subset would have done well without adjuvant therapy
ctDNA represents a potential biologic tool to distinguish these populations.
Retrospective Analyses: ctDNA as a Strong Prognostic MarkerIn a retrospective analysis of IMvigor010:4
- ctDNA(+) patients had dramatically worse DFS and OS in the observation arm.
- In ctDNA(+) patients, atezolizumab improved DFS (HR 0.58).
- ctDNA(–) patients derived little to no benefit.
These results generated the hypothesis that ctDNA positivity identifies patients who “need” and may benefit from adjuvant immunotherapy, while ctDNA negativity identifies those cured by surgery alone.
Retrospective ctDNA profiling in CheckMate 274 demonstrated similar trends:
- ctDNA(+) patients had worse DFS and OS.
- Nivolumab benefit appeared enriched in ctDNA(+) patients.
Taken together, these findings suggest that ctDNA may act as both a prognostic biomarker and a predictive enrichment tool for adjuvant immunotherapy.
IMvigor011: Prospective ctDNA-Guided Adjuvant ImmunotherapyDr. Galsky then presented IMvigor011, the first prospective ctDNA-directed adjuvant immunotherapy trial,6 utilizing the following approach:
- Identify patients ctDNA(+) after radical cystectomy
- Randomize them to atezolizumab versus placebo
- ctDNA(–) patients receive no adjuvant treatment
The primary endpoint was DFS in ctDNA-positive patients. This trial tests whether molecular recurrence is an actionable disease state and whether treatment in this window improves outcomes.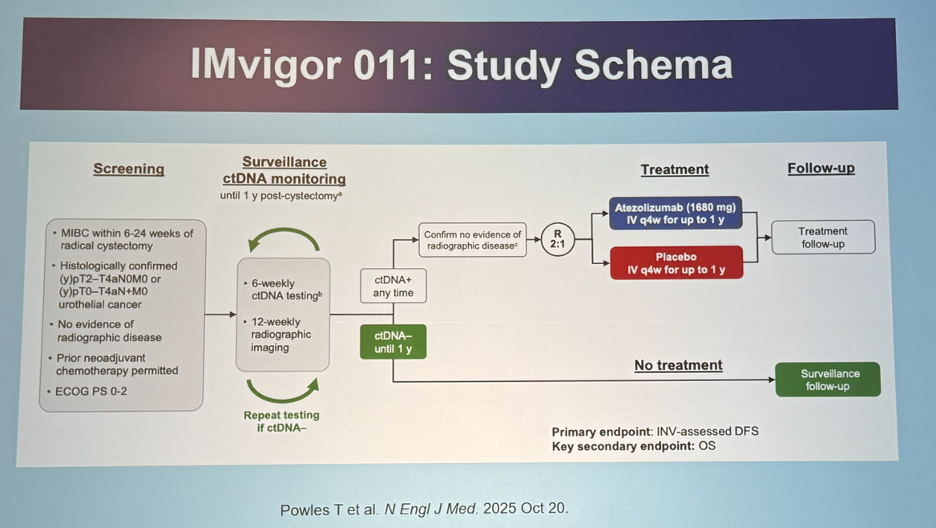
ctDNA Kinetics in IMvigor011
Overall, 607 patients were included for analysis:
- 459 (76%) were baseline ctDNA(–)
- 148 (24%) were ctDNA(+)
- 22% of baseline ctDNA(–) patients converted to ctDNA(+) over follow-up
- 4% developed metastatic disease before ctDNA conversion
For patients who were ctDNA(+):
- DFS and OS are significantly worse compared to the overall population
- Treatment benefit appears to align with ctDNA positivity
- DFS benefit: Median, 9.9 versus 4.8 months (HR: 0.64, 95% CI: 0.47–0.87, p=0.005)
- OS benefit: Median, 32.8 versus 21.1 months (HR: 0.59, 95% CI: 0.39–0.90, p=0.01)
Patients who remained persistently ctDNA(–):
- Remarkably favorable prognosis
- Median DFS and OS not reached
- Very low event rates over long-term follow-up
These data reinforce ctDNA(–) status as a high-confidence biomarker of cure after cystectomy.
Dr. Galsky’s take-home messages from IMvigor011 were as follows:
- Patients ctDNA(+) after surgery need adjuvant therapy, and outcomes remain suboptimal with current regimens.
- Molecular recurrence (conversion from ctDNA– to ctDNA+) is a distinct, actionable disease state.
- Persistently ctDNA(-) patients generally have an excellent prognosis, suggesting that adjuvant therapy may be safely omitted.
- A definitive question remains: Is treatment upon molecular recurrence non-inferior to upfront adjuvant therapy? This is not yet known.
NIAGARA Study: Although NIAGARA is not a ctDNA-directed study, Dr. Galsky used this study to highlight the broader evolution of perioperative systemic therapy. NIAGARA demonstrated improved overall survival outcomes with neoadjuvant chemotherapy plus durvalumab followed by adjuvant durvalumab in unselected patients (24 months: 82.2% versus 75.2%; HR: 0.75, 95% CI: 0.59–0.93, p=0.01).7
The exploratory ctDNA data embedded within NIAGARA mirror the same patterns seen across other datasets:
- Patients who achieve ctDNA clearance after neoadjuvant therapy exhibit excellent survival, with curves resembling persistently ctDNA-negative cystectomy-only cohorts.
- Patients who remain ctDNA-positive despite neoadjuvant therapy show rapid divergence in survival curves, reinforcing MRD as the central determinant of relapse biology.
These results underscore the inevitability of ctDNA’s integration: even in trials not designed around MRD, ctDNA provides prognostic information that pathology alone cannot.
Notably, pre-RC ctDNA status did not reliably predict pathologic complete responses (pCR), with pre-RC ctDNA(-) patients having a pCR in only 51% of cases. Conversely, almost all (97%) of pre-RC ctDNA+ patients did not achieve a pCR.
In conclusion, Dr. Galsky’s presentation provided a clear and compelling narrative for the integration of ctDNA into perioperative MIBC management. Retrospective and emerging prospective data consistently show that:
- ctDNA positivity = high risk = likely to benefit from adjuvant therapy
- Persistent ctDNA negativity = excellent prognosis = potential to avoid adjuvant treatment
As ctDNA-guided trials mature, this approach may redefine perioperative treatment—not by intensifying therapy for all, but by personalizing escalation and de-escalation based on molecular risk.
Presented by: Matthew Galsky, MD, Professor of Medicine, Hematology and Medical Oncology, Director of Genitourinary Medical Oncology, Co-Director of the Center of Excellence for Bladder Cancer at The Tisch Cancer Institute, and Associate Director for Translational Research at The Tisch Cancer Institute, New York, NY
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, December 2nd–5th, 2025
References:- Bellmunt J, Hussain M, Gschwend JE, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): A multicentre, open-label, randomized, phase 3 trial. Lancet Oncol. 2021; 22(4):525-537.
- Apolo AB, Ballman KV, Sonpavde G, et al. Adjuvant Pembrolizumab versus Observation in Muscle-Invasive Urothelial Carcinoma. N Engl J Med. 2025; 392:45-55.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021 3;384(22):2102-2114.
- Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021; 595(7867):432-437.
- Galsky MD, Gschwend JE, Milowsky MI, et al. Adjuvant nivolumab versus placebo for high-risk muscle-invasive urothelial carcinoma: 5-year efficacy and ctDNA results from CheckMate 274. Ann Oncol. 2025; S0923-7534(25)04930-0.
- Powles T, Kann AG, Castellano D, et al. ctDNA-Guided Adjuvant Atezolizumab in Muscle-Invasive Bladder Cancer. N Engl J Med. 2025.
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024; 391:1773-1786.