(UroToday.com) The 2024 Society of Urologic Oncology (SUO) annual meeting held in Dallas, between December 3 and December 6, 2024, was host to the Prostate Cancer Session I. Dr. Sarah Psutka discussed how to measure and mitigate decision regret in the management of genitourinary cancers, and how to improve our shared decision-making skills.
Dr. Psutka began her presentation by stating that in 2024, complex decision-making has become the norm in genitourinary (GU) oncology. She illustrated this with two examples:
- For localized prostate cancer, patients and clinicians face a multitude of options, including focal ablation, robotic prostatectomy, and various forms of radiation therapy (brachytherapy, SBRT, IMRT), with or without androgen deprivation therapy (ADT).
- For localized high-risk renal cell carcinoma (RCC), N1, M1 NED, or pT2+ / muscle-invasive bladder cancer (MIBC) post-radical cystectomy (RC), the decision involves whether to administer adjuvant immunotherapy or not.
The definition of regret is a highly negative emotion caused by the feeling that an outcome would have been better if one had made a different choice. Regret is associated with highly negative emotions in our patients. There are mainly two types of regrets in oncology:
- Anticipatory regret: When a patient takes into consideration regret that could result from a specific decision:
- Experienced by patients & providers
- Influences decision-making strongly
- Postoperative/Posttreatment Regret: Regret regarding a previous decision to accept a specific treatment, experienced in retrospect
- This regret is independently associated with decreased quality of life.
Dr. Psutka highlighted that regret is an area not very well understood in oncology but has garnered growing interest. She noted that a search for "decision regret in oncology" on PubMed reveals an explosion of publications on this topic since 1997.
Decisional regret in oncology can occur, either following initial treatment or following recurrence as illustrated below:
The question to ask is how do can we measure decision regret? And the answer is short: by using validated instruments and tools.
Dr. Psutkga presented multiple validated decision regret validated scales and tools:
- Decision Regret Scale (5-item): measures “distress" or "remorse" after a medical treatment decision
- The Regret and Disappointment Scale
- Was It Worth It (Treatment Utility)
- Anticipated Regret Questionnaire
- Anticipated Regret Scale
- Experienced Regret Scale
- Regret Experience Measure
- Regret and Maximization Scale
- Regret measurement scale
Dr. Psutka discussed the Decision Regret Scale (DRS), a 5-item tool used to assess regret after medical treatment decisions. She emphasized that this scale is her preferred tool due to its practicality and ease of use.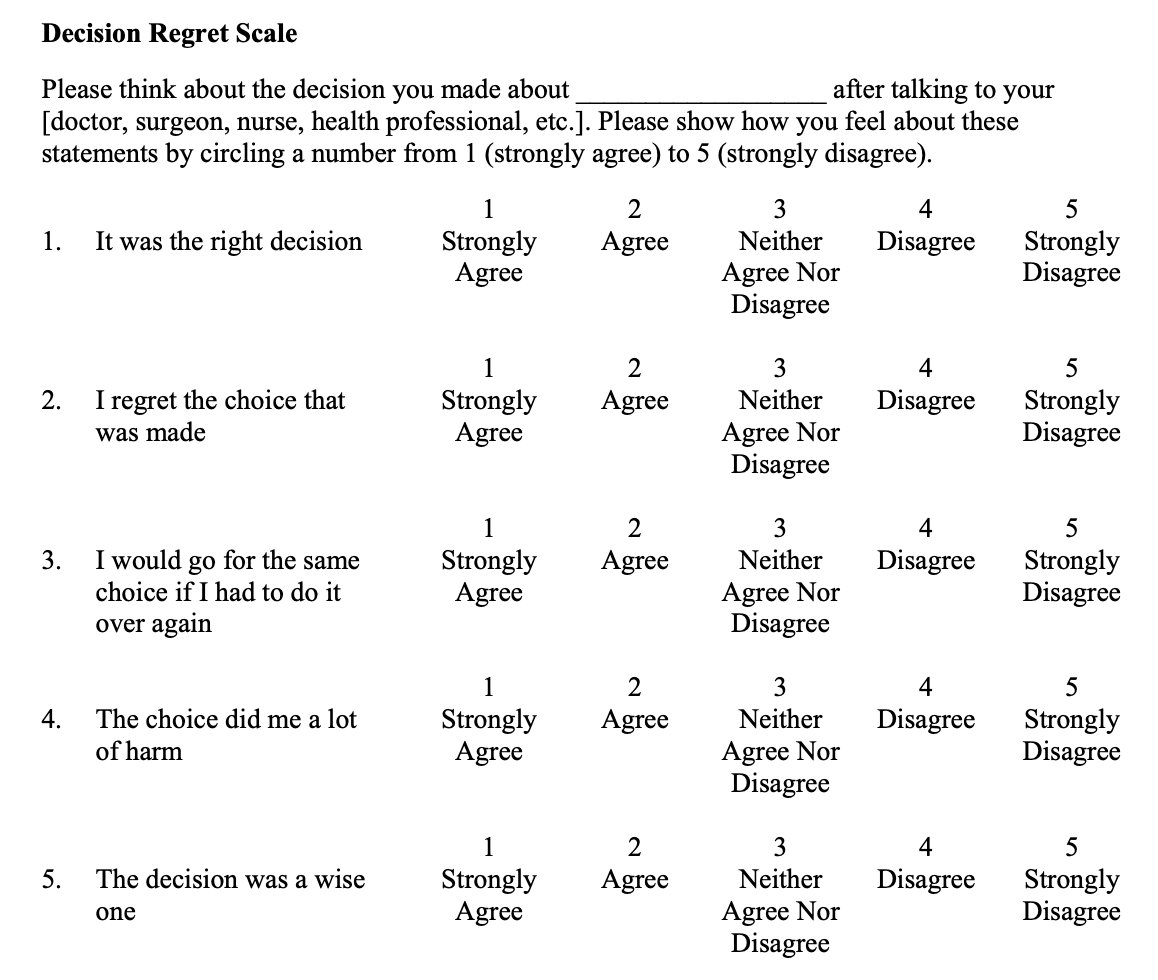
Dr. Psutka highlighted that decision regret in genitourinary (GU) oncology is prevalent yet variable in its frequency, with approximately 1 in 7 patients experiencing it. The incidence of decision regret is notably higher in surgical oncology compared to benign disease treatments. For instance, regret is quite common following treatment for localized prostate cancer” and it could be over 50% independent of the type of treatment/surveillance that was chosen:
Dr. Psutka emphasized that decision regret is not only common in localized prostate cancer treatment but also prevalent in other GU cancers. For instance, one year following treatment for bladder cancer, approximately 15% of patients experience moderate to severe decision regret. Additionally, decision regret is notably high among patients with benign renal masses, with 49% experiencing regret regardless of the treatment received. Specifically, 62% of patients who underwent active surveillance reported decision regret, compared to 41% of those who opted for surgery. Despite these significant findings, there remains a paucity of data in other GU cancer disease spaces, highlighting the need for further research and better decision-making support for patients across all GU oncology diagnoses.
There are many implications of decisional regret for our patients. Including worse postoperative pain, increased anxiety and distress, reduced quality of life and decision regret can strain the relationship between the patient and the surgeon.
Dr. Psutka mentioned that there are three buckets of factors related to decisional regret in patients with GU malignancies: patient-related factors, procedure/condition related factors, and lastly physician related factors. These factors are summarized in the table below: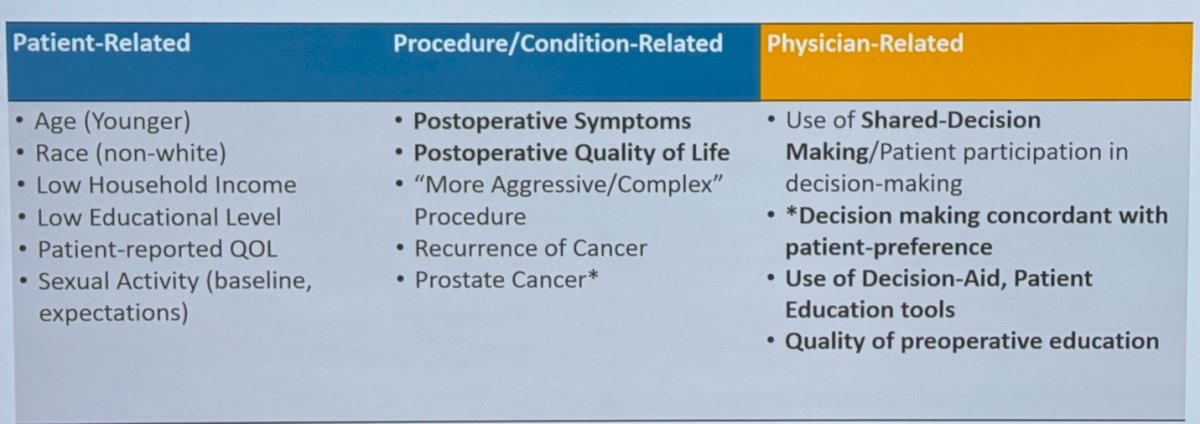
We need tools to mitigate Decisional Regret and Provide Goal-Aligned Care to our patients, including patient engagement in decision-making and care, increasing patient knowledge which should help to improve their health, and finding out that the Value/Priority for each patient is concordant with the care we are offering these tools could be:
- Affective Forecasting
- Informed Consent
- Decision Coaches for Patients
- Shared Decision-Making
- Decision Aids
Dr. Psutka discussed the concept of affective forecasting, which refers to a patient's prediction of how they will feel in the future about a decision they are making in the present. She highlighted several risk factors that contribute to poor affective forecasting, including:
- Intense emotions during the decision-making process
- Involvement of multiple people in the decision-making process
- The impact of the decision or cancer on the patient's life beyond their physical health, such as quality of life (QOL) and relationships
- Inadequate prognostic information provided to the patient
Dr. Psutka emphasized the importance of strategies to avoid poor affective forecasting and resultant decisional regret. These strategies include:
- Providing clear and accurate predictions to help patients understand potential outcomes
- Limiting emotional distress and minimizing the impact of clinician bias on the decision-making process
We all do informed consents in our clinics, but do we know what they are? It is a detailed and unbiased explanation of side effects, consequences, expected outcomes of a treatment on:
- Cancer outcomes (efficacy)
- Quality of life
- Post-treatment symptoms
- Post-treatment function
- Short-term/long-term trade-offs
This is non-directive support delivered by a healthcare provider to help patients prepare to actively participate in making health decisions. This approach is increasingly popular and involves decision coaches who support patients by identifying decision-making needs, reviewing evidence-based data regarding options, clarifying values for outcomes, encouraging communication of preferences to others, and providing patients with decision aids. This helps patients be better prepared to engage in active discussions during their clinic visits.
This is an actual agreement on a treatment plan that incorporates patient preferences. Moreover, strengthens patient autonomy, increases patient engagement in their care, and can lead to decreased overdiagnosis and overtreatment. Additionally, this approach improves patient satisfaction and can enhance long-term health-related quality of life, It is also associated with a decrease in decisional regret, as patients feel more confident in their choices and more involved in the decision-making process. The requirements for shared-decision making are outlined below.
Evidence-based tools, such as decision aids, are designed to help patients acquire disease- and treatment-specific information, personalize it, and identify their preferences. These tools aim to increase patient knowledge about the risks of their disease and treatment options while supplementing physician counseling. They offer valuable datapoints that can help provide personalized estimates of risk.
Both patients and physicians can benefit from using decision aids, as they:
- Feel more informed and less uncertain about their options
- Participate more actively in the decision-making process
- Make decisions that are more aligned with their personal preferences
- Experience better healthcare experiences and improved health outcomes
- Have less decision regret, as they are more confident in their choices and feel their voices have been heard.
Unmet needs in decision aid tools is that most of them are primarily developed in English, which limits accessibility for non-English-speaking populations. Additionally, patients often want to know specific, practical information that extends beyond medical details. For instance, they may be concerned with day-to-day activities, such as when they can go grocery shopping, travel by plane, or visit their family. Incorporating treatment burden, including these personal and lifestyle factors, into decision aids is essential to provide patients with a holistic view of their treatment and recovery journey. Moreover, incorporation of patient-specific information including functional status, life expectancy in prediction models is critical, as well as optimization of best practices regarding how to implement decision aids in clinical practice.
Dr. Psutka summarized critical areas in GU oncology where we need decision aids to support shared decision-making, these are shown below: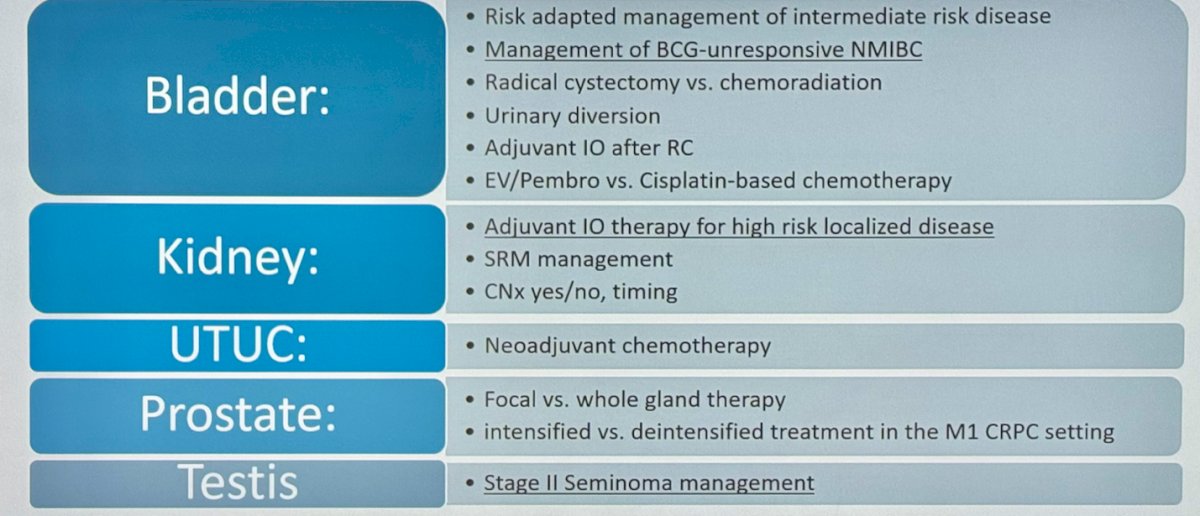
There is a clear need to create opportunities for training in shared decision-making. While the American Urological Association (AUA) has actively engaged in promoting shared decision-making, many providers report feeling uncomfortable with the process, especially when working with disparate populations. To address this, the AUA has developed case-based courses and promotes workshops aimed at educating providers on the principles and practice of shared decision-making.
Dr. Psutka concluded her presentations with the following messages:
- Decision Regret is common in GU Oncology and there is a need to understand patient preferences in treatment decisions.
- Poor affective forecasting, such as emotional distress and inadequate prognostic information, can lead to decision regret.
- We need to use strategies to mitigate decisional regret, including providing clear predictions, reducing emotional distress, and using decision aids to ensure that patients feel informed and involved in their decision-making.
- Decision aids, help patients feel more informed, make decisions aligned with their preferences, and improve long-term health-related quality of life supporting shared decision-making
Presented by: Sarah Psutka, MD, MSc, Associate Professor of Urology in the Department of Urology at the University of Washington and Fred Hutchinson Cancer Center
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2024 Society of Urologic Oncology (SUO) annual meeting held in Dallas, between the 3rd and 6th of December, 2024.