(UroToday.com) The 2025 Colombian Urological Society (SCU) Annual Meeting held in Cartagena, Colombia, between August 20th and August 23rd was host to the Urothelial Carcinoma Plenary. Dr. Ricardo Rendon discussed Stage-Based Management of Non-Muscle Invasive Bladder Cancer.
Dr. Rendon began by highlighting that the majority of bladder cancers are non-muscle invasive (NMIBC), accounting for about 75% of newly diagnosed cases. Among these, Ta tumors represent approximately 60%, T1 tumors 25–30%, and carcinoma in situ (CIS) up to 10%. Despite their early stage, NMIBC carries a high recurrence rate of nearly 70% and a progression rate of 10–20%. Importantly, the risk of progression is strongly linked to grade, ranging from 2% in grade I, 11% in grade II, and up to 45% in grade III disease.
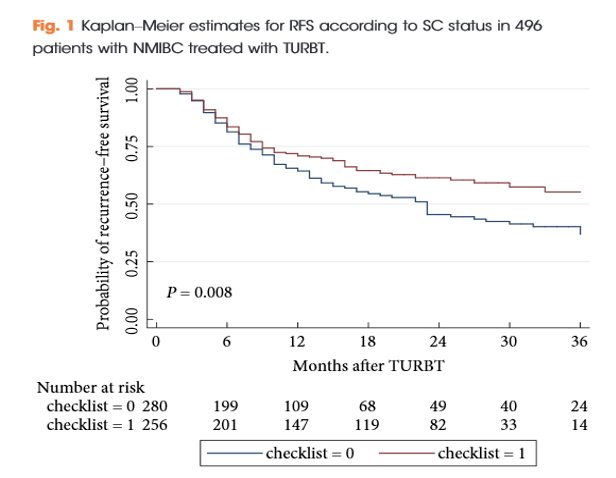
Principles of NMIBC Management #1.Perform a high-quality quality good transurethral resection of bladder tumor (TURBT), not just good enough. Dr. Rendon emphasized that the first and most critical step in the management of NMIBC is the complete resection of all visible tumors. This requires meticulous TURBT technique, ensuring specimens are sent separately, avoiding excessive fulguration, using enhanced visualization methods when available, and including detrusor muscle in the resection for accurate staging. Adequate hemostasis, checking for perforation, and performing EUA risk-stratification are also essential steps to optimize outcomes and guide further therapy. Dr. Rendon highlighted a study evaluating the use of a standardized checklist to improve the quality of TURBT in patients with NMIBC. The findings demonstrated that patients in whom the checklist was applied had a significantly lower risk of recurrence, translating into improved recurrence-free survival compared to those without the checklist, as illustrated below. Underscoring the importance of quality control measures during TURBT to optimize oncologic outcomes.2
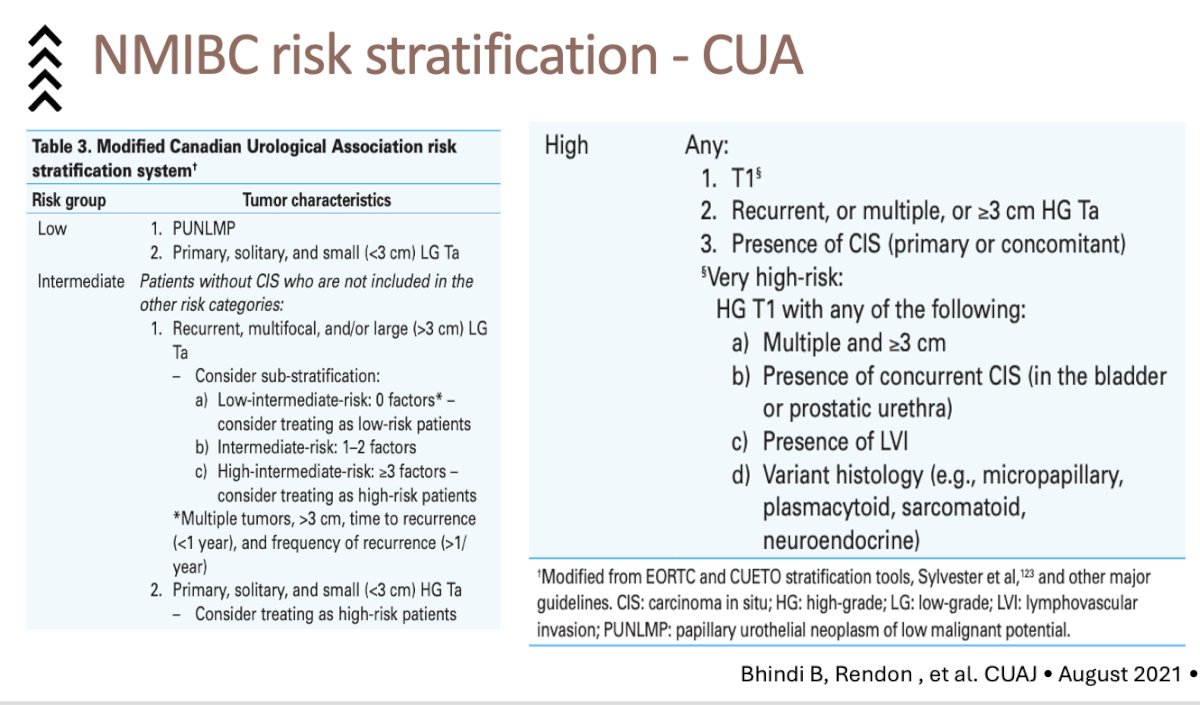
Dr. Rendon emphasized that the second principle of NMIBC management is risk stratification, underscoring the importance of tailoring management strategies to individual patient risk. He highlighted the Canadian Urological Association (CUA) risk-stratification system, which categorizes patients into low, intermediate, high, and very high-risk groups based on tumor characteristics such as size, grade, recurrence, presence of CIS, and variant histology. This framework, adapted from EORTC and CUETO tools, provides a refined approach to identify patients at higher risk of progression, thereby guiding decisions on surveillance, intravesical therapy, or more aggressive treatment.

The third principle in NMIBC management is to select the appropriate intravesical therapy. Dr. Rendon highlighted the landmark Messing study,3 where patients with low-risk and low-grade appearing tumors were randomized to receive either 2 g of gemcitabine or saline after TURBT. Results demonstrated that a single postoperative instillation of gemcitabine significantly reduced recurrences, with a 4-year RFS of 66% versus 46% with saline. Importantly, there were no differences in progression, establishing gemcitabine as an effective, low-toxicity option for recurrence reduction in low-risk patients.

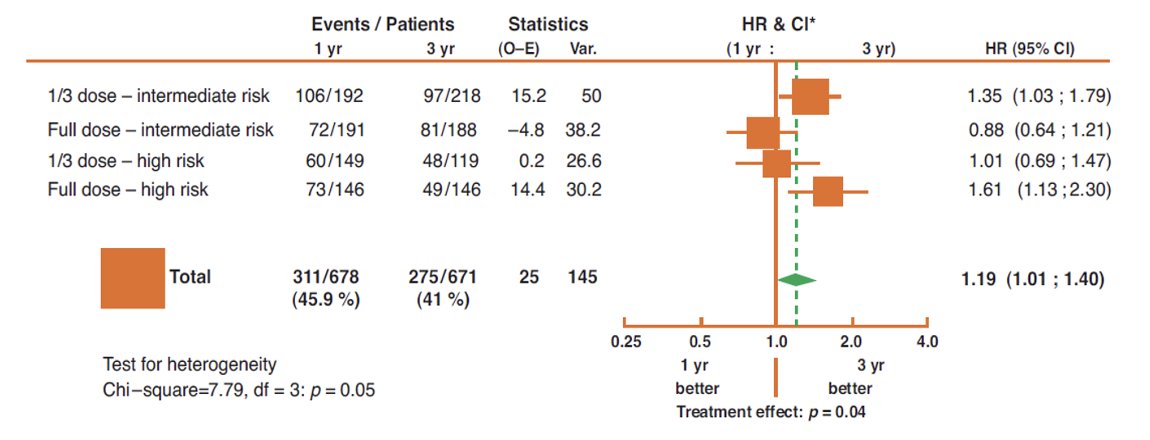
Dr. Rendón noted that for patients with intermediate-risk NMIBC, BCG induction followed by one year of maintenance remains the current standard of care. He highlighted data showing that for this group, full-dose BCG provides effective disease control without requiring prolonged maintenance, whereas for high-risk patients, longer treatment durations and full-dose regimens are necessary to optimize outcomes. (4)
Notably, for patients with high-risk NMIBC, three years of maintenance BCG remains a critical component of management. Dr. Rendon highlighted the pivotal SWOG 8507 trial, which demonstrated that maintenance BCG significantly improved recurrence-free survival and provided the only treatment showing a PFS benefit in this setting.5
Lastly, Dr. Rendon emphasized the merits of timely cystectomy in patients with high-risk features, noting that upfront radical cystectomy with PLND should be strongly considered in cases of HG T1 disease with adverse pathological features such as variant histology, deep invasion into or beyond the muscularis mucosa, presence of LVI or concomitant CIS, and in patients with large, multifocal, or persistent T1 tumors despite re-TURBT.
The role of cystectomy for BCG-unresponsive NMIBCDr. Rendon emphasized that the first step in approaching treatment options is to clearly define BCG-unresponsive disease. This includes:
- Persistent or recurrent CIS alone, or with recurrent Ta/T1, within 12 months of completing BCG
- Recurrent high-grade Ta/T1 within 6 months of completing BCG
- High-grade T1 at the first evaluation following induction BCG
In the setting of BCG-unresponsive NMIBC, Dr. Rendon highlighted emerging intravesical options such as gemcitabine plus docetaxel. In a cohort of 275 patients, 38% were BCG-unresponsive and received induction with GEM + DOCE for 6 weeks, followed by monthly maintenance for 12–24 months in responders. Reported outcomes showed a 12-month RFS of 60% and a 24-month RFS of 46%, with high-grade RFS of 52% at 2 years. The cystectomy rate was 15%. Importantly, this regimen is currently undergoing prospective validation, and results from this validation are eagerly awaited.6
Current FDA-Approved therapies for BCG unresponsive NMIBC are:
- IV pembrolizumab (2020)
- Intravesical nadofaragene firadenovec (2022)
- Intravesical nogapendekin alfa inbakicept-pmln (Anktiva) + BCG (2023)
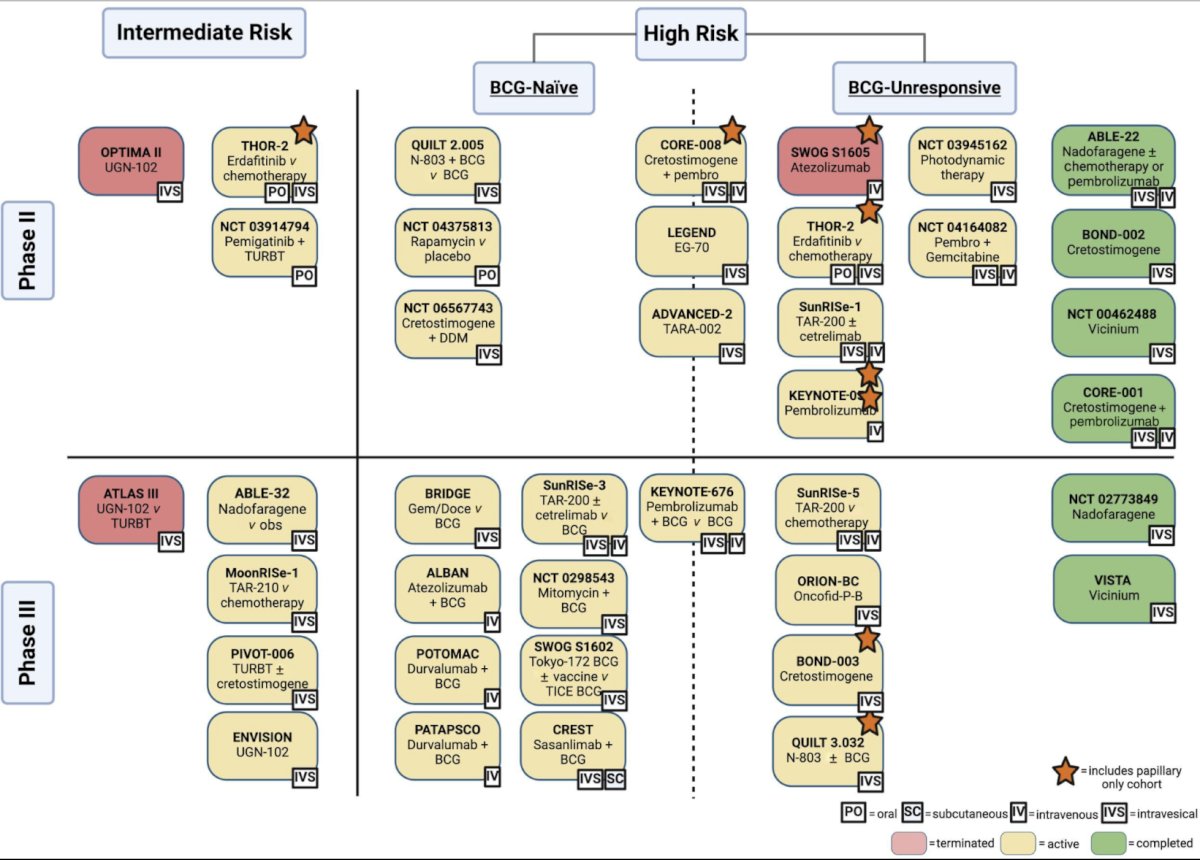
The fourth principle in the management of NMIBC is to consider novel therapies or clinical trials for appropriate patients. As highlighted, there is a broad landscape of ongoing and completed studies across intermediate-, high-risk, and BCG-unresponsive disease. These include intravesical agents (such as gemcitabine, docetaxel, mitomycin, and cretostimogene), systemic immunotherapies (including pembrolizumab, atezolizumab, and durvalumab), and novel approaches such as TAR-200 delivery systems, N-803, and combinations with checkpoint inhibitors. He underscored that these trials represent critical opportunities to improve outcomes beyond standard BCG and to address the unmet need in BCG-unresponsive patients.
Lastly, Dr. Rendon reminded the audience that upper tract and prostatic urethral evaluation should never be overlooked, particularly given the risk of recurrence every 1–2 years in patients with high-risk disease. He further emphasized the importance of incorporating counseling on smoking cessation strategies as a key component of NMIBC management.
Presented by: Ricardo Rendon, MD, Urologic Oncologist at Dalhousie University, Halifax, NS, Canada.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Colombian Urological Society (SCU) Annual Meeting held in Cartagena, Colombia, between August 20th and August 23rd
References:
- Kaufman DS, Shipley WU, Feldman AS. Bladder cancer. Lancet. 2009 Jul 18;374(9685):239-49. doi: 10.1016/S0140-6736(09)60491-8. Epub 2009 Jun 10. PMID: 19520422.
- Suarez-Ibarrola R, Soria F, Abufaraj M, D'Andrea D, Preto M, Gust KM, Briganti A, Shariat SF, Gontero P. Surgical checklist impact on recurrence-free survival of patients with non-muscle-invasive bladder cancer undergoing transurethral resection of bladder tumour. BJU Int. 2019 Apr;123(4):646-650. doi: 10.1111/bju.14557. Epub 2018 Oct 23. PMID: 30248235.
- Messing EM, Tangen CM, Lerner SP, Sahasrabudhe DM, Koppie TM, Wood DP Jr, Mack PC, Svatek RS, Evans CP, Hafez KS, Culkin DJ, Brand TC, Karsh LI, Holzbeierlein JM, Wilson SS, Wu G, Plets M, Vogelzang NJ, Thompson IM Jr. Effect of Intravesical Instillation of Gemcitabine vs Saline Immediately Following Resection of Suspected Low-Grade Non-Muscle-Invasive Bladder Cancer on Tumor Recurrence: SWOG S0337 Randomized Clinical Trial. JAMA. 2018 May 8;319(18):1880-1888. doi: 10.1001/jama.2018.4657. PMID: 29801011; PMCID: PMC6583489.
- Oddens J, Brausi M, Sylvester R, Bono A, van de Beek C, van Andel G, Gontero P, Hoeltl W, Turkeri L, Marreaud S, Collette S, Oosterlinck W. Final results of an EORTC-GU cancers group randomized study of maintenance bacillus Calmette-Guérin in intermediate- and high-risk Ta, T1 papillary carcinoma of the urinary bladder: one-third dose versus full dose and 1 year versus 3 years of maintenance. Eur Urol. 2013 Mar;63(3):462-72. doi: 10.1016/j.eururo.2012.10.039. Epub 2012 Nov 2. PMID: 23141049.
- Lamm DL, Blumenstein BA, Crissman JD, Montie JE, Gottesman JE, Lowe BA, Sarosdy MF, Bohl RD, Grossman HB, Beck TM, Leimert JT, Crawford ED. Maintenance bacillus Calmette-Guerin immunotherapy for recurrent TA, T1, and carcinoma in situ transitional cell carcinoma of the bladder: a randomized Southwest Oncology Group Study. J Urol. 2000 Apr;163(4):1124-9. PMID: 10737480.
- Steinberg RL, Thomas LJ, Brooks N, Mott SL, Vitale A, Crump T, Rao MY, Daniels MJ, Wang J, Nagaraju S, DeWolf WC, Lamm DL, Kates M, Hyndman ME, Kamat AM, Bivalacqua TJ, Nepple KG, O'Donnell MA. Multi-Institution Evaluation of Sequential Gemcitabine and Docetaxel as Rescue Therapy for Nonmuscle Invasive Bladder Cancer. J Urol. 2020 May;203(5):902-909. doi: 10.1097/JU.0000000000000688. Epub 2019 Dec 10. PMID: 31821066.