(UroToday.com) The 2025 Colombian Urological Society (SCU) Annual Meeting was held in Cartagena, Colombia, between August 20th and August 23rd. was host to the Prostate Cancer Plenary. Dr. Carlos Granados delved into the Future of PSMA Theranostics.
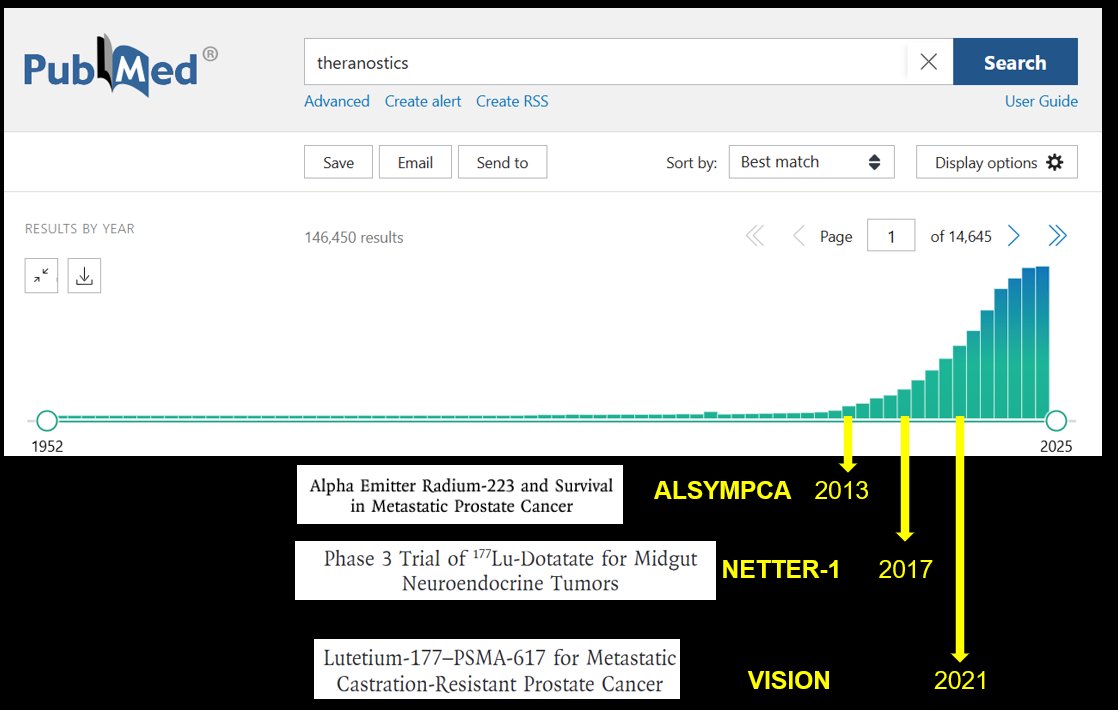
Dr. Granados began by highlighting the rapid growth of publications in the field of theranostics, with more than 146,000 results currently indexed in PubMed. He emphasized landmark phase 3 trials that have shaped the field, including ALSYMPCA (2013) with radium-223 in metastatic prostate cancer, NETTER-1 (2017) with 177Lu-Dotatate in midgut neuroendocrine tumors, and VISION (2021) evaluating 177Lu-PSMA-617 in metastatic castration-resistant prostate cancer (mCRPC).
However, there are global disparities in access to theranostics for prostate cancer, Dr Granados highlighted recent data from a recent Lancet Oncology Commission. The map illustrates significant variation in annual use of 177Lu-PSMA and ^225Ac-PSMA per million inhabitants, with the highest utilization seen in countries like Australia and parts of Europe, while large regions in Africa, South America, and Asia show minimal or no access. This underscores both the promise of theranostics and the urgent need to address inequities in global availability.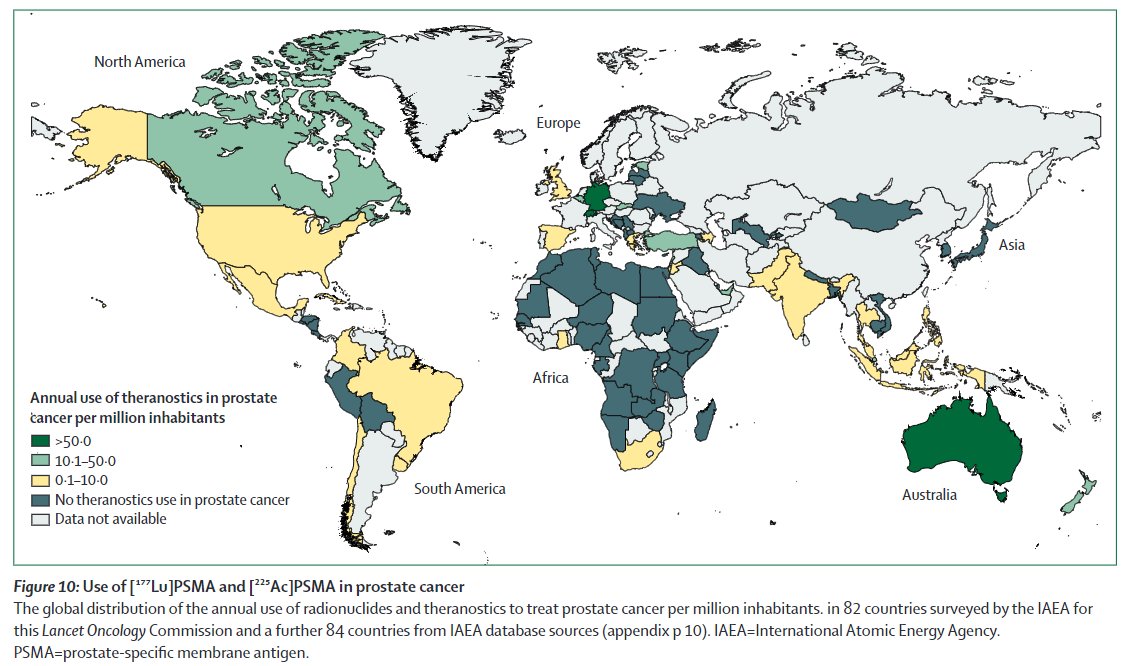
Dr. Granados then outlined the evolving treatment landscape across the prostate cancer disease continuum. Starting with HSPC, patients may benefit from definitive local therapy and additional options such as docetaxel or abiraterone for high-risk disease, and metastasis-directed therapy for oligometastatic cases. As patients progress to nmCRPC and mCRPC, treatment expands to include ARPIs (enzalutamide, apalutamide, darolutamide, abiraterone), taxane-based chemotherapy, PARP inhibitors in BRCA-mutated disease, radiopharmaceuticals (223Ra) and theranostics (177Lu-PSMA). Notably, this would continue to move down the prostate cancer treatment continuum.
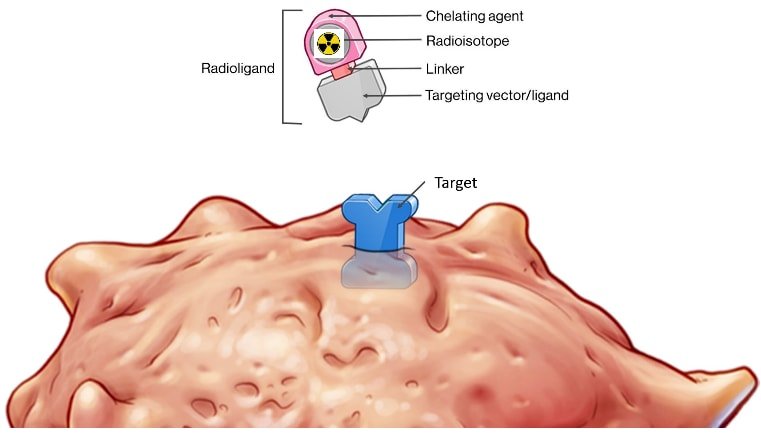
Theranostics represents a rapidly evolving field in prostate cancer that integrates both diagnosis and therapy using the same molecular target. A radioligand is designed with a targeting vector, typically directed against PSMA, which is linked to a radioactive isotope. When labeled with a diagnostic isotope such as 68Ga or 18F, it allows for precise localization of disease through PET imaging. The same ligand can then be coupled with a therapeutic isotope such as 177Lu or 225Ac, delivering targeted radiation directly to tumor cells while sparing surrounding normal tissues. This dual ability to both “see” and “treat” disease exemplifies personalized medicine and has reshaped the management paradigm in advanced prostate cancer.
The tumor microenvironment plays a critical role in shaping theranostic response. As illustrated, radioligands not only bind to cancer cell surface targets such as PSMA, GRPR, or CXCR4, but also interact within a complex ecosystem of macrophages, fibroblasts, and immune cells. Once internalized, radioligands generate DNA damage that can be potentiated by agents like PARP or ATR inhibitors, increasing tumor mutational burden and the release of neoantigens. This, in turn, may enhance immunogenicity and response to immune checkpoint blockade. Understanding this interplay between radioligand therapy, DNA damage response pathways, and immune modulation is key to advancing combination strategies and optimizing patient outcomes.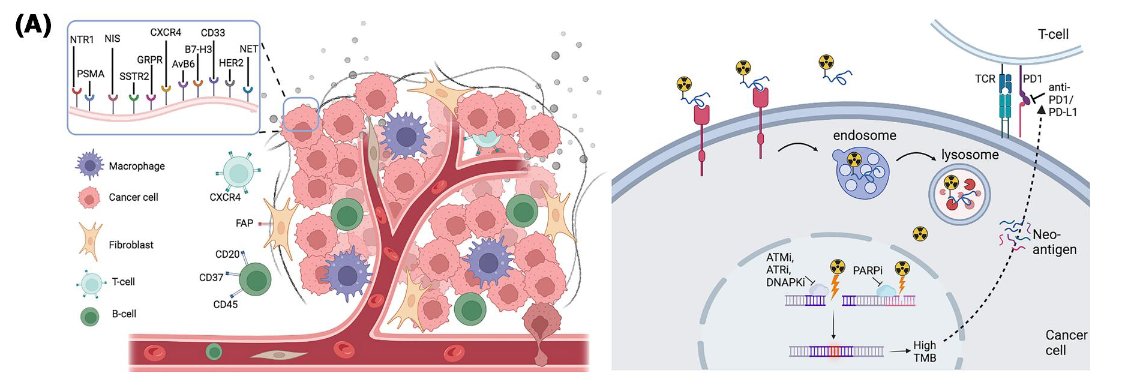
Notably, there are multiple ligand modalities that can be utilized in theranostics, each with distinct structural and pharmacologic properties. These include small molecules (~100 Daltons), peptides (~1,000 Daltons), small proteins and antibody fragments (~10,000 Daltons), and full antibodies (~100,000 Daltons). Their differences in size, molecular weight, and binding characteristics influence factors such as tumor penetration, specificity, circulation half-life, and potential therapeutic applications.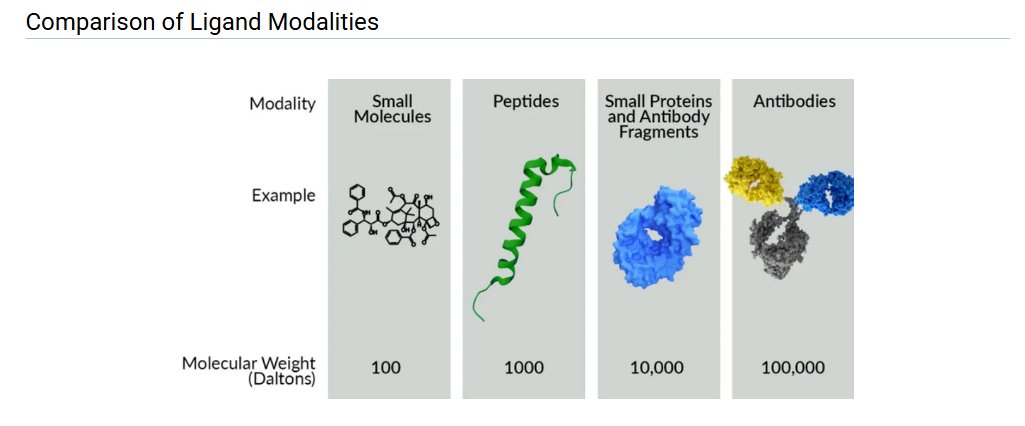
Dr. Granados noted that the global theranostics landscape is booming and increasingly diversified. Beyond PSMA, active programs now target SSTR2, GRPR, FAP, CXCR4, HER2, DLL3, and more, using a range of ligands (small molecules, peptides, minibodies, full antibodies) paired with multiple isotopes (177Lu, 225Ac, 212Pb, 131I, 67Cu). Most agents remain in preclinical or early phase trials, but a growing number have advanced into phase 2/3, and a few are already approved most notably lutetium-177–based therapies such as Lutathera and Pluvicto. Dozens of companies are contributing to this pipeline, underscoring broad commercial and clinical momentum as the field moves from proof of concept to scalable, disease-specific applications.
If we look at the current trial landscape, theranostics has rapidly expanded across oncology, but prostate cancer clearly leads the field. A quick search of ongoing trials highlights that multiple radiolabeled molecules are being investigated, with prostate cancer far outpacing other tumor types such as breast, lung, neuroendocrine, and hepatocellular carcinoma. This surge underscores how PSMA-targeted theranostics has transformed prostate cancer management and continues to dominate global clinical research efforts in this space.

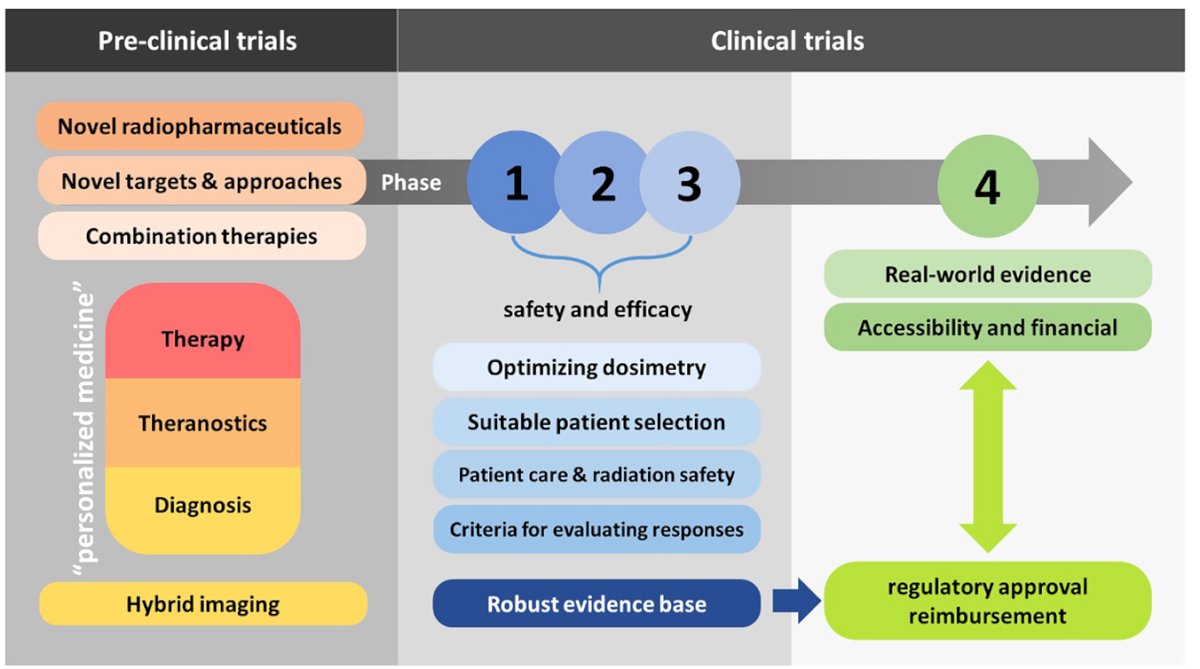
Dr. Granados outlined how the process of bringing theranostics into practice is lengthy, beginning with pre-clinical trials that test novel radiopharmaceuticals, new targets and approaches, and potential combination strategies. Once therapies advance into clinical development, phases 1–3 focus on establishing safety and efficacy, while also refining dosimetry, patient selection, and radiation safety, as well as setting clear criteria for evaluating responses. These steps are essential to build a robust evidence base before moving into phase 4, which emphasizes real-world data, accessibility, and financial considerations. Importantly, regulatory approval and reimbursement decisions depend on this evidence, highlighting why the translation of theranostics into clinical use is a rigorous but necessary process.
Dr. Granados emphasized that prostate cancer is characterized by marked tumor heterogeneity, which directly impacts the use of theranostics. While some lesions demonstrate strong PSMA uptake, others may only be detected with FDG radiotracers as shown below, leaving a subset of patients ineligible for PSMA-targeted therapies. This variability underscores the complexity of PSMA heterogeneity and highlights the need for a more nuanced, personalized approach in determining which patients are most likely to benefit from theranostic treatment strategies and still to be determined if we should be doing both PSMA and FDG PET/CTs on these patients.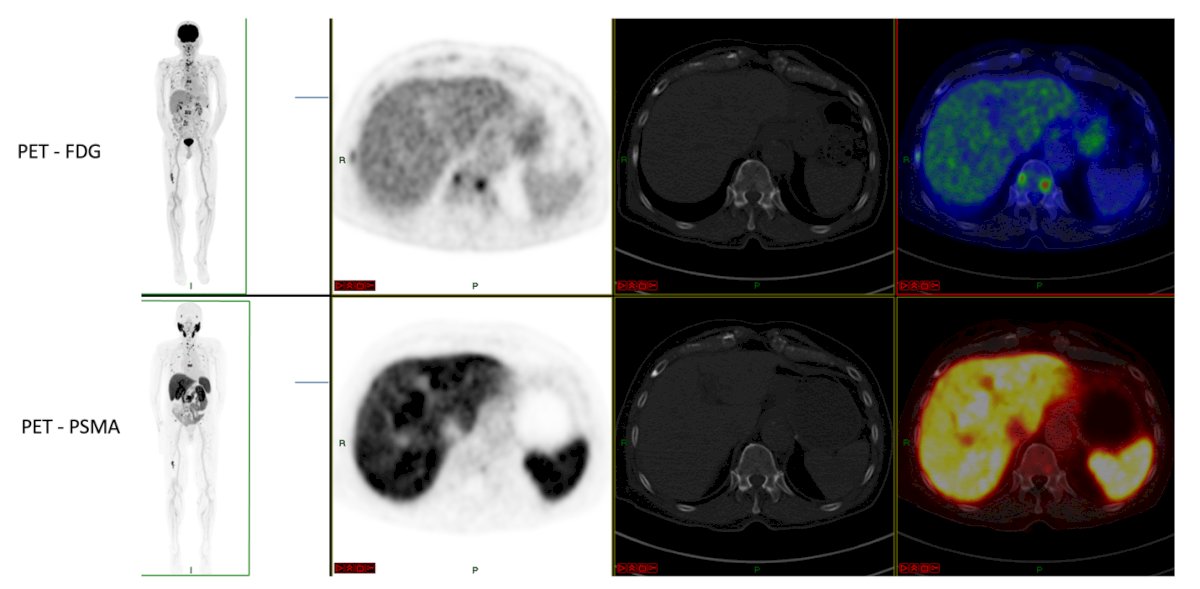
Defining PSMA positivity is essential when determining eligibility for PSMA-targeted radioligand therapy. As illustrated, PSMA uptake varies across lesions, with heterogeneity observed both between and within patients over time. The miPSMA scoring system helps standardize assessment, distinguishing PSMA-negative from positive disease and guiding trial inclusion, as in VISION. Importantly, heterogeneity at the pathological or radiological level can result in patchy PSMA expression, underscoring the need for careful selection to optimize outcomes and opening opportunities for research in this field. This reinforces the principle that theranostic treatment in prostate cancer must be personalized, balancing imaging findings, tumor biology, and clinical context.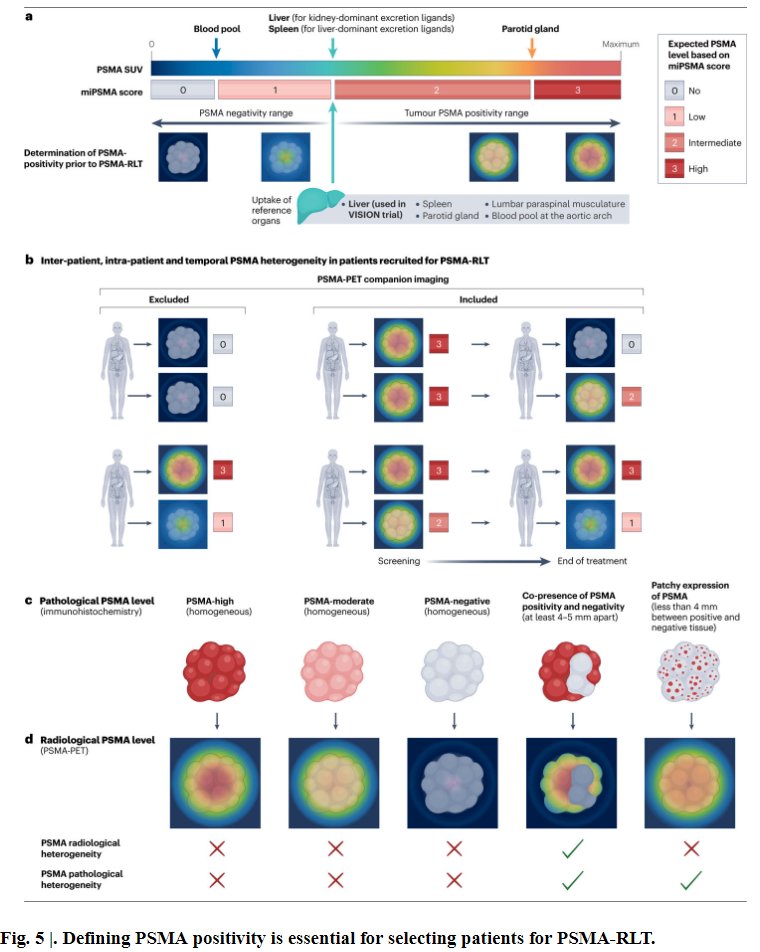
Dr. Granados emphasized one of the unique advantages of radioligand therapy (RLT): the ability to both “treat what we see” and “see what we treat.” He illustrated this with the case of a patient who underwent therapy with 177Lu-PSMA. On baseline imaging, the patient had extensive disease, but after three treatment cycles, follow-up PET/CT demonstrated near complete resolution of disease activity with no evidence of residual disease, underscoring the precision and therapeutic impact of PSMA-targeted R.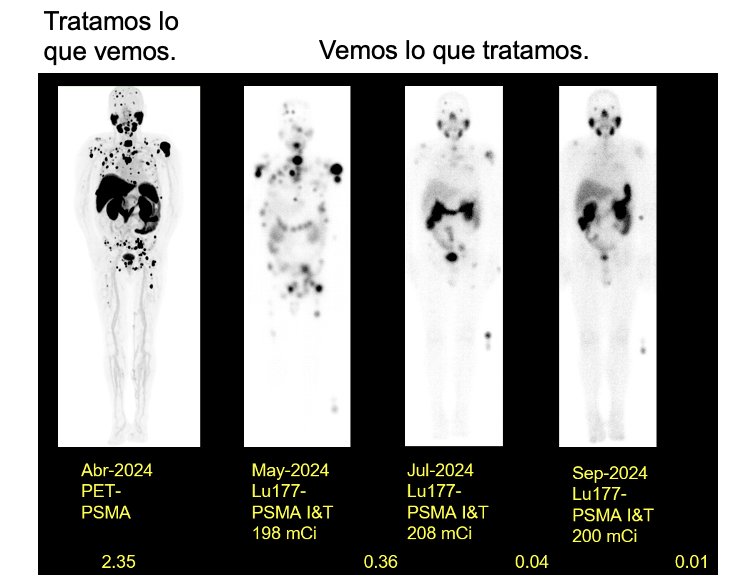
Another critical aspect is the difference between activity and dose in RLT. While activity (measured in Ci/mCi or Bq/MBq) represents the prescribed amount of radioactivity administered, the absorbed dose (measured in Gy) reflects the actual radiation delivered to the tumor and organs at risk. Importantly, imaging-based dosimetry allows quantification of tumor dose versus limiting doses in critical organs. For example, as shown below, a patient receiving RLT achieved an average tumor dose of 25 Gy after the first cycle, but also absorbed 3.6 Gy in the kidneys, 0.29 Gy in the bone marrow, and 1.06 Gy in the parotid glands. These data highlight the delicate balance between maximizing tumor control and minimizing toxicity, underscoring the importance of individualized dosimetry in treatment planning.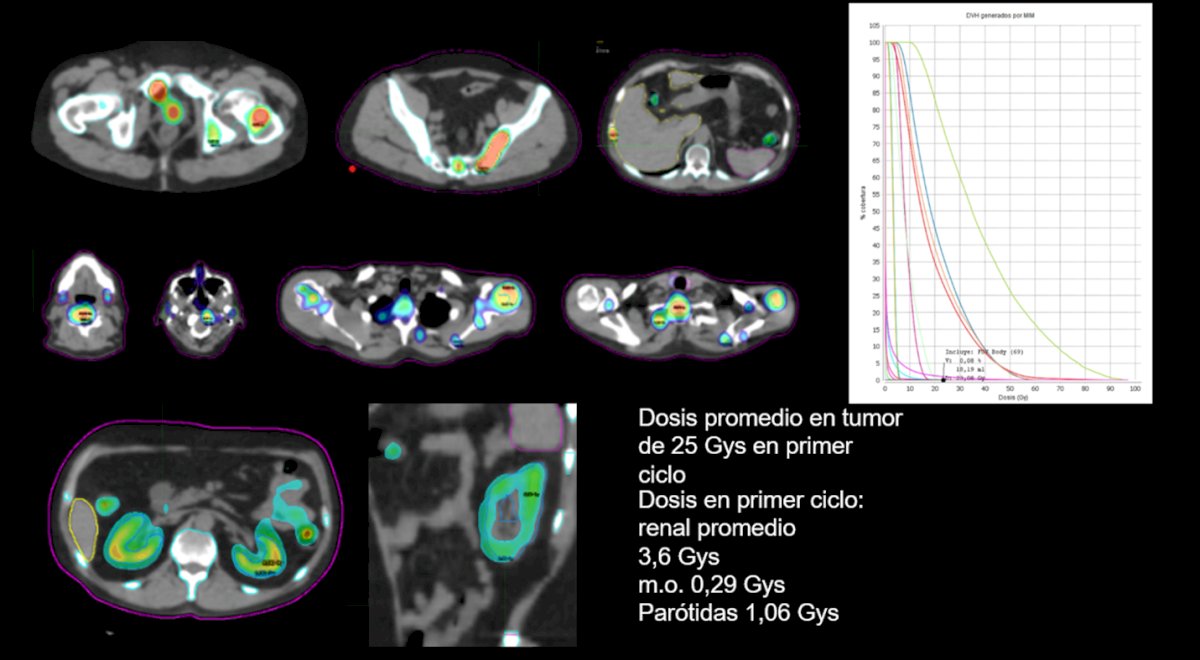
To move towards personalized radiopharmaceutical therapies, Dr. Granados emphasized the role of theranostic digital twins (TDTs), a patient-specific model designed to integrate baseline imaging, clinical features, and dosimetry to optimize treatment planning in PSMA theranostics. The pipeline involves standardizing multimodal data, segmenting lesions and organs at risk, modeling radiotracer kinetics for voxel-level dosimetry, and predicting treatment benefit while enforcing safety thresholds for kidneys, salivary glands, and marrow. Importantly, TDTs allow adaptive replanning with each treatment cycle, updating predictions based on follow-up imaging and therapy response. This iterative framework not only personalizes isotope selection, dose, and cycle number but also provides a learning loop to refine predictions over time, ultimately aiming to maximize tumor control while minimizing toxicity.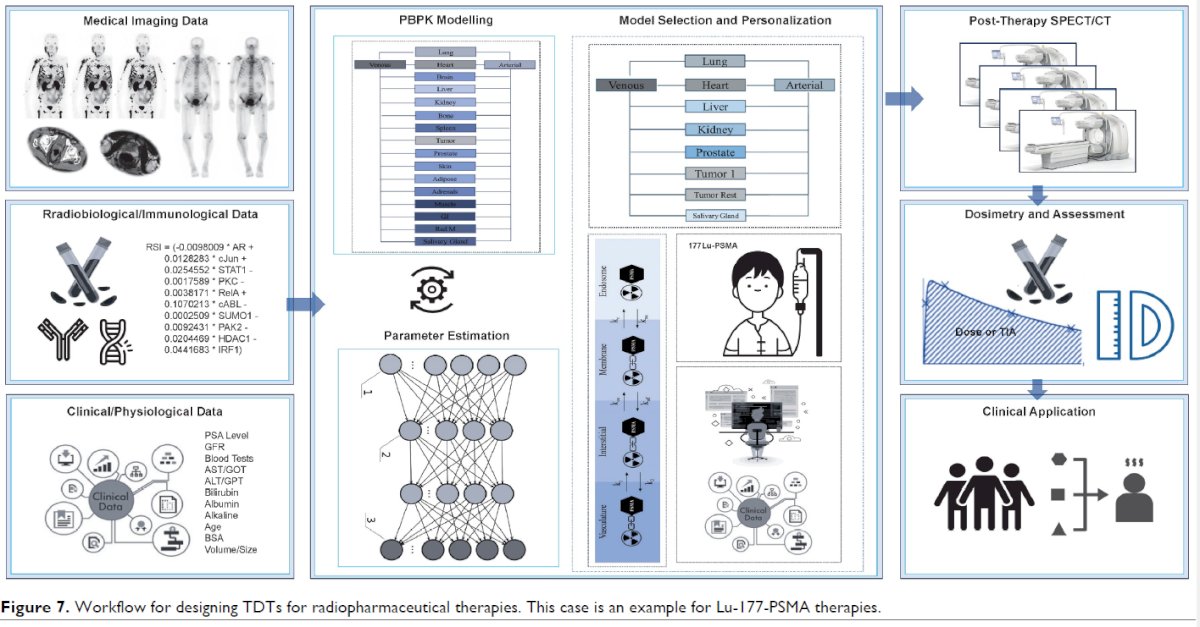
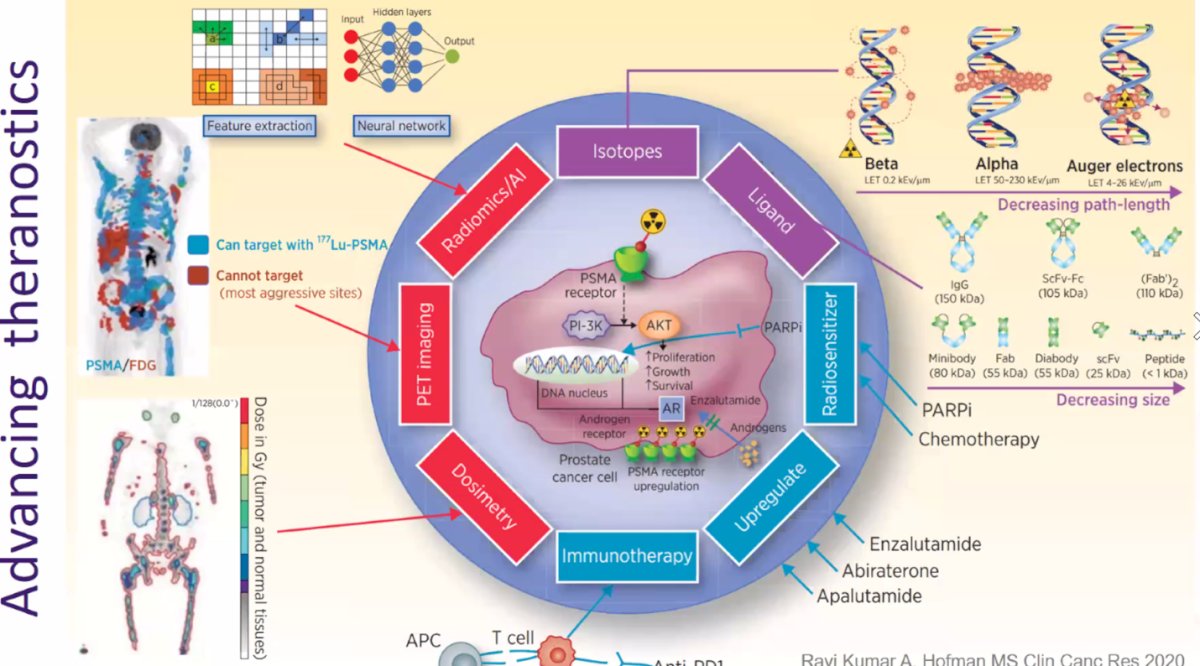
Lastly, Dr. Granados wrapped up highlighting this graphic from Dr. Michael Hofman. Notably, advancing theranostics will require the integration of multiple innovations, including the use of novel isotopes with varying particle emissions and path lengths, optimized ligands of decreasing size to enhance tumor targeting, and radiosensitizers to improve treatment efficacy. He emphasized the importance of combining PSMA-targeted RLT with other systemic therapies such as PARPi, chemotherapy, and AR-targeted agents (enzalutamide, abiraterone, apalutamide), as well as exploring synergies with immunotherapy. Additionally, tools like PET imaging, dosimetry, radiomics, and AI-driven feature extraction and neural networks will play a central role in tailoring treatment, refining dose delivery, and identifying aggressive disease sites that may not be targetable with conventional PSMA ligands. This multidimensional approach forms the roadmap toward more precise and effective theranostic strategies in prostate cancer.
Presented by: Carlos Granados, MD, MSc, Nuclear Medicine Physician at Cancer Treatment and Research Center (CTIC) and Hospital Universitario San Ignacio (HUSI). Bogotá, Colombia.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Colombian Urological Society (SCU) Annual Meeting held in Cartagena, Colombia, between August 20th and August 23rd