(UroToday.com) The 2025 Colombian Urological Society (SCU) Annual Meeting held in Cartagena, Colombia, between August 20th and August 23rd was host to the Prostate Cancer Plenary. Dr. Ricardo Rendon discussed the evaluation and management of biochemical recurrence in prostate cancer.
Dr. Rendón began by highlighting that biochemical recurrence (BCR) in prostate cancer is a rapidly evolving area in terms of evaluation and treatment options, affecting approximately 20–40% of patients treated with curative intent. He emphasized the considerable heterogeneity in how BCR is defined, which varies depending on whether it occurs after radical prostatectomy or radiation therapy. For example, AUA/ASTRO/SUO defines BCR post-prostatectomy as a PSA increase of ≥0.2 ng/mL with a confirmatory value ≥0.2 ng/mL, while NCCN considers any detectable PSA that rises on ≥2 tests or exceeds 0.1 ng/mL. ASCO defines it as a detectable PSA with a subsequent rise, and EAU/ESTRO/ESUR/ISUP/SIOG sets the threshold at PSA >0.4 ng/mL and rising. After External Beam Radiation Therapy (EBRT), most guidelines define BCR as a PSA increase of >2 ng/mL above nadir, underscoring the variability in criteria used across organizations.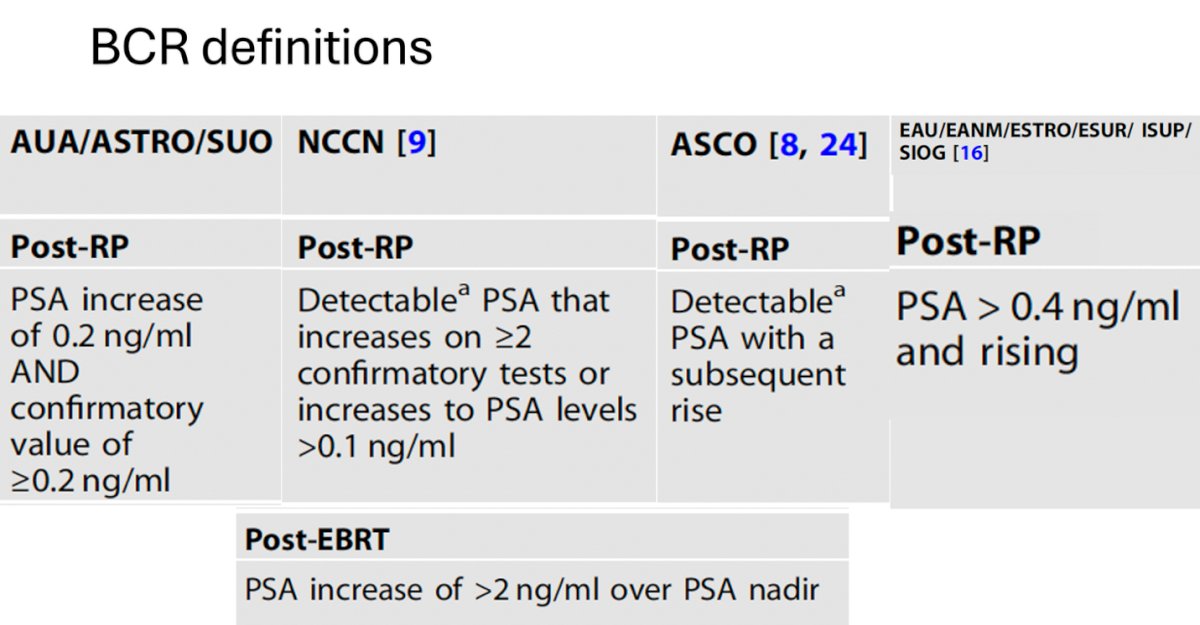
The BCR population is highly heterogeneous, encompassing patients previously treated with surgery, radiation, ADT, or combinations thereof, across a wide spectrum of stages (pT2–pT4, N0–N+) and grades. He noted that to optimize management, it is crucial to understand the natural history of BCR, integrate patient-specific factors such as overall health and life expectancy, consider tumor biology, and draw insights from clinical trial data to guide individualized treatment decisions.
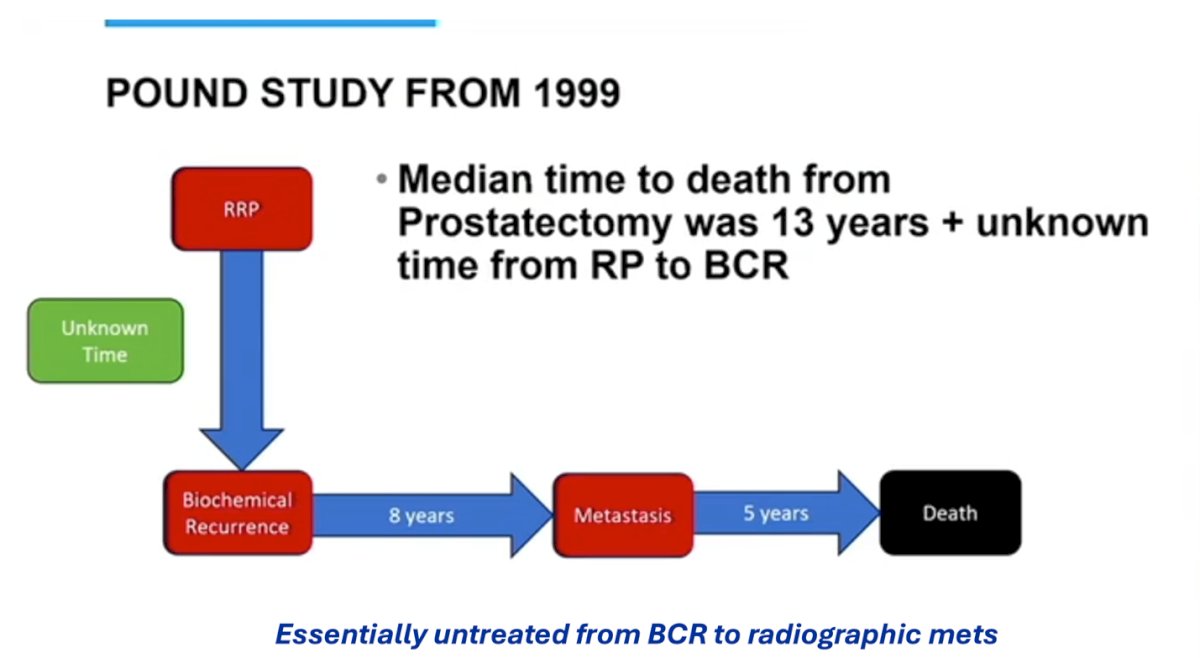
Dr. Rendón referenced the classic Pound et al study from 1999, which demonstrated that the median time from radical prostatectomy to death was about 13 years, plus an additional unknown interval from surgery to BCR. Once BCR occurred, the median time to metastasis was approximately 8 years, followed by another 5 years from metastasis to death. Importantly, this natural history was observed in an essentially untreated population, highlighting how prolonged the disease course can be without intervention.1
Dr. Rendon emphasized that salvage radiotherapy remains the standard of care for patients with BCR following definitive therapy. He highlighted the findings of the ARTISTIC meta-analysis, which pooled data from 2,153 patients across three RCTs (RADICALS-RT, GETUG-AFU 17, and RAVES). The analysis demonstrated no significant difference in event-free survival between adjuvant and early salvage radiotherapy, supporting the strategy of reserving radiation for patients who recur rather than exposing all high-risk patients to immediate adjuvant treatment. This approach allows for more personalized therapy while minimizing overtreatment.2
In BCR prostate cancer, high-risk features include Grade Group 4–5, pT3b–4 stage, node-positive disease, short PSA doubling time, early recurrence after primary therapy, higher post-prostatectomy PSA, adverse genomic classifier results, and PET findings, with positive margins linked to both increased risk of BCR and lower progression after salvage RT. A summary of these high-risk features is shown below.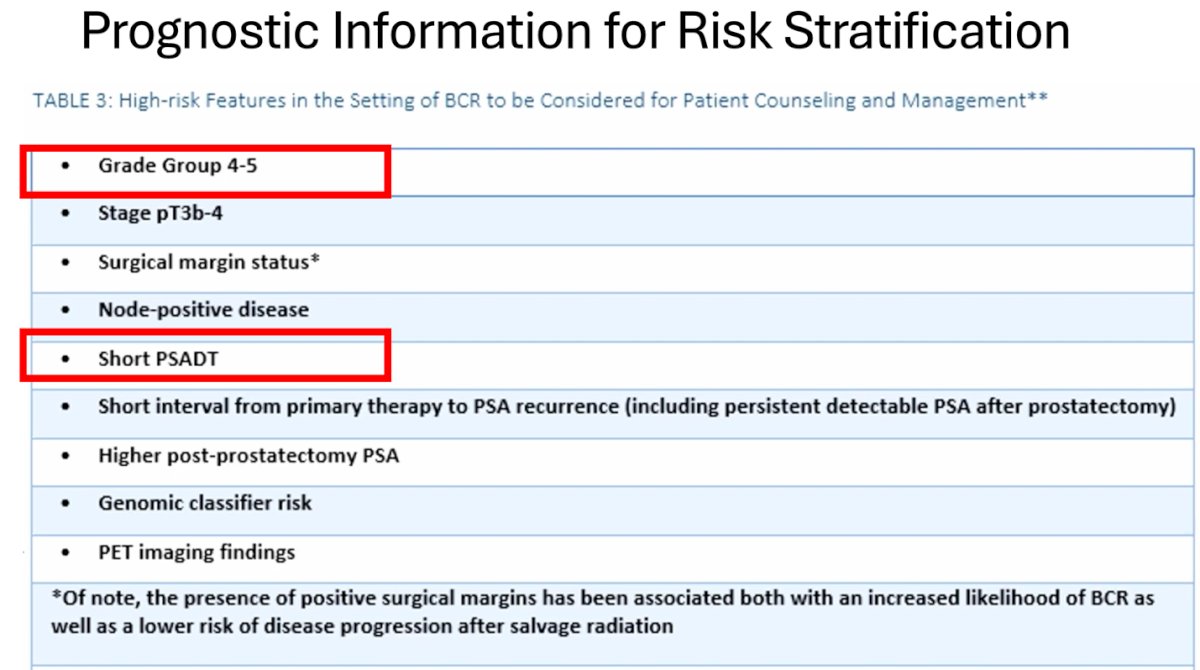
Dr. Rendon emphasized that PSA doubling time (PSADT) is the strongest predictor of progression in BCR prostate cancer. Patients with a PSADT <3 Months have a metastasis-free survival (MFS) of about 1 year, those with PSADT 3–9 months have an MFS of 3–4 years, while many with PSADT >15 months never metastasize. Importantly, 90% of deaths occur in patients with PSADT <15 months, a finding validated across multiple cohorts.1
Dr Rendon highlighted the European Association of Urology (EAU) risk stratification system for BCR:
- EAU High-Risk BCR
- PSA-DT <1 year OR pGS 8-10 (ISUP grade 4-5) for RP
- IBF <18 months OR bGS 8-10 (ISUP grade 4-5) for RT
- EAU Low-Risk BCR
- PSA-DT >1 year AND pGS <8 (ISUP grade <4) for RP
- IBF > 18 months AND bGS <8 (ISUP grade <4) for RT (3)
An external validation study of the EAU risk groups in 1,040 patients with BCR after primary RP confirmed their prognostic value, showing excellent discrimination for MFS and prostate cancer–specific mortality (PCSM). At 5 years, MFS was 99.7% for patients classified as EAU low-risk and 86.7% for those in the high-risk group, underscoring the importance of this stratification in guiding patient counseling and management.
Dr. Rendon summarized evidence showing that in patients with PSA-DT <6 months, salvage radiotherapy (sRT) significantly reduced PCSM (HR 0.24), with an even greater benefit when combined with ADT (HR 0.14). Importantly, this protective effect was only observed when sRT was initiated within 2 years of BCR and before PSA rose above 0.5 ng/ml. Conversely, in patients with PSA-DT >6 months, sRT ± ADT did not significantly impact outcomes, and delaying sRT initiation had no effect. (3,4)
Guideline recommendations for BCR management emphasize risk-adapted treatment. Observation is preferred in patients with low-risk BCR, while in those with high-risk disease, particularly with short PSA-DT, early initiation of therapy is advised, ideally when PSA remains <0.5 ng/ml, as this timing has been associated with improved outcomes.
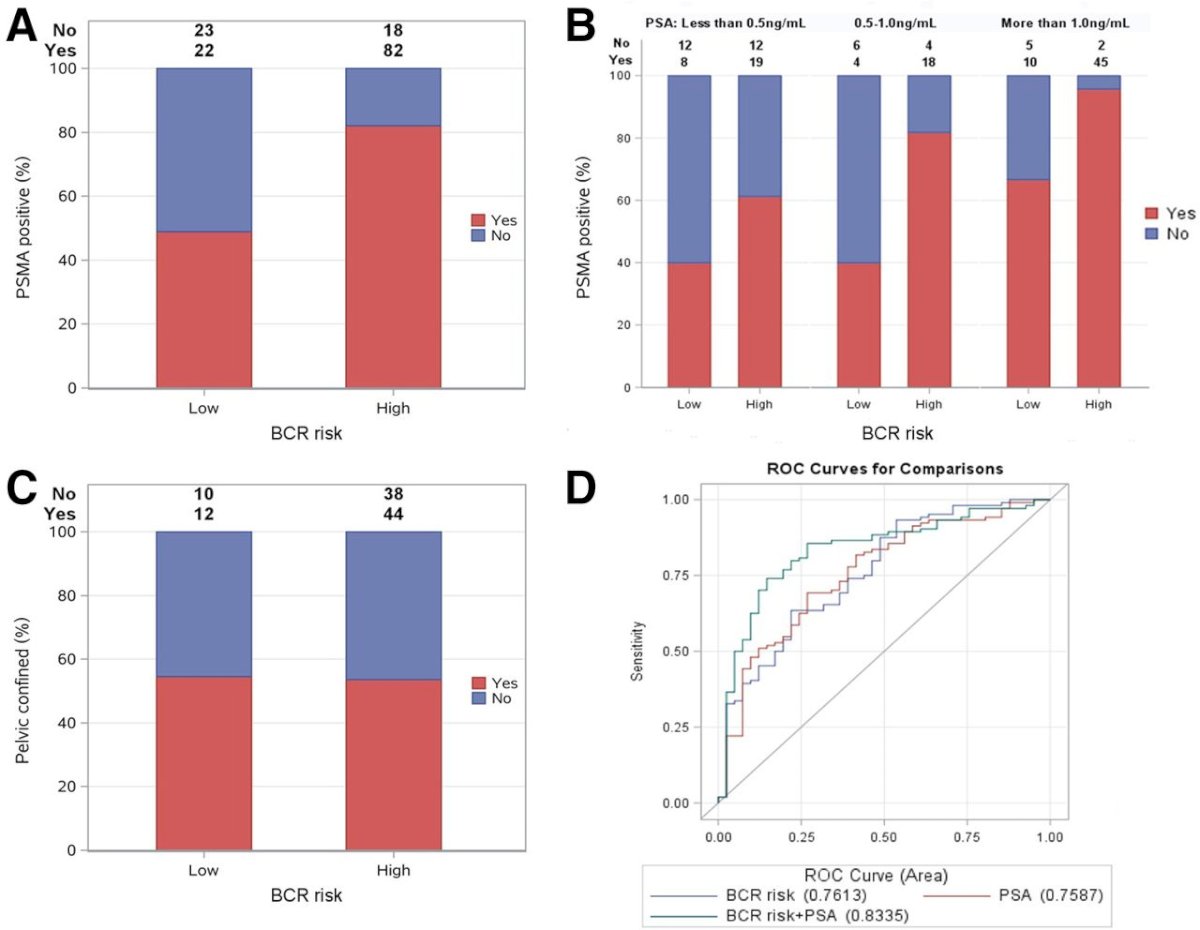
Imaging in the setting of BCR plays a key role in ruling out metastatic disease and avoiding unnecessary salvage radiation. The pre-test probability of a positive scan is strongly influenced by PSA level, with detection rates of approximately 45% in patients with PSA values between 0.2–0.49 ng/ml.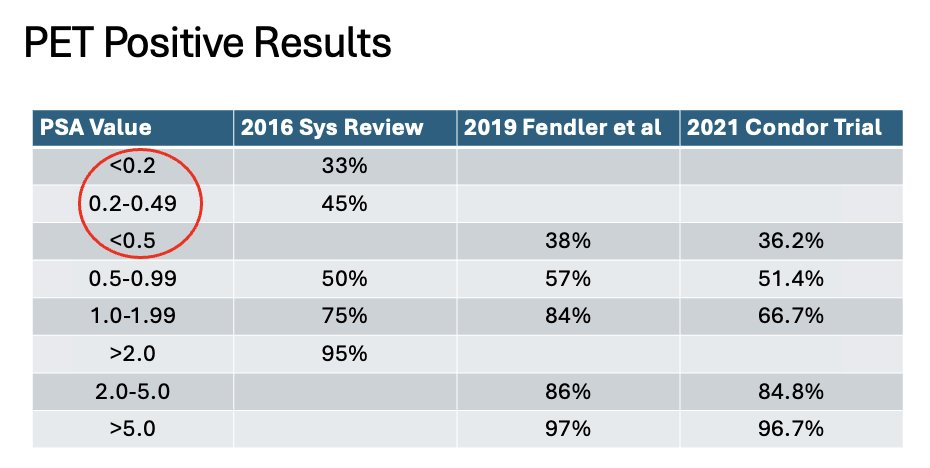
As illustrated below, higher-risk BCR patients showed greater rates of PSMA positivity compared to low-risk cases, with positivity increasing as PSA levels rose, particularly above 1.0 ng/ml. Roughly half of the recurrences in both low- and high-risk groups were pelvic-confined. ROC analyses demonstrated that combining PSA with BCR risk improved predictive accuracy (AUC 0.8335) compared with either factor alone. Notably PSA doubling time is also a strong predictor of PSMA PET positivity.
What if all local therapy fails?
Dr. Rendon highlighted the EMBARK trial, a randomized Phase 3 study that enrolled patients with high-risk BCR, defined as PSADT ≤9 months and a screening PSA ≥1 ng/mL after RP or ≥2 ng/mL above the nadir following EBRT, with additional criteria including serum testosterone ≥150 ng/dL, ECOG PS 0–1, no distant metastases, and no recent hormonal therapy. Patients were randomized 1:1:1 to enzalutamide plus leuprolide, enzalutamide monotherapy, or leuprolide alone, stratified by PSA level, PSADT, and prior hormonal therapy. Treatment was suspended at week 36 if PSA fell <0.2 ng/mL, with re-initiation upon PSA rise. The primary endpoint was MFS for enzalutamide plus leuprolide versus leuprolide, with key secondary endpoints including MFS for enzalutamide monotherapy, time to PSA progression, time to new antineoplastic therapy, OS, and safety.5

Notably, the primary endpoint of EMBARK, MFS, was strongly positive in favor of enzalutamide plus ADT, showing a 58% reduction in the risk of metastasis or death, with a median follow-up of 61 months. Dr. Rendon highlighted that just over a month ago it was confirmed that the trial also met its secondary endpoint of overall survival.5

Dr Rendon concluded his presentation with the following take-home messages:
- Not all patients and recurrences are the same
- Best predictors post-RP: PSA-DT <1 year and Gleason >7
- Key endpoints: MFS, CSS
- PSMA PET/CT is changing the management landscape
- PSA >0.3 in EAU high-risk patients is clinically relevant
- Limited accuracy for nodal disease (Sensitivity ~ 43%) is not sufficient to guide treatment decisions
- Low-risk patients should be considered for surveillance, assess PSA-DT (no RT, no ADT)
- High-risk patients need early sRT before PSA rises to 0.5 ng/ml
- High-risk patients benefit from sRT + ADT (6 vs 24 months, RADICALS-HD
- We should be considering ARPI for 2 years for very high-risk, node-positive patients (STAMPEDE)
- Lastly, he encourages us to consider enzalutamide for high-risk patients with no further local therapy options (EMBARK)
Presented by: Ricardo Rendon, MD, Urologic Oncologist at Dalhousie University, Halifax, NS, Canada.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Colombian Urological Society (SCU) Annual Meeting held in Cartagena, Colombia, between August 20th and August 23rd
References:
- Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999 May 5;281(17):1591-7. doi: 10.1001/jama.281.17.1591. PMID: 10235151.
- Vale CL, Fisher D, Kneebone A, Parker C, Pearse M, Richaud P, Sargos P, Sydes MR, Brawley C, Brihoum M, Brown C, Chabaud S, Cook A, Forcat S, Fraser-Browne C, Latorzeff I, Parmar MKB, Tierney JF; ARTISTIC Meta-analysis Group. Adjuvant or early salvage radiotherapy for the treatment of localised and locally advanced prostate cancer: a prospectively planned systematic review and meta-analysis of aggregate data. Lancet. 2020 Oct 31;396(10260):1422-1431. doi: 10.1016/S0140-6736(20)31952-8. Epub 2020 Sep 28. PMID: 33002431; PMCID: PMC7611137.
- Preisser F, Abrams-Pompe RS, Stelwagen PJ, Böhmer D, Zattoni F, Magli A, Rivas JG, Dilme RV, Sepulcri M, Eguibar A, Heidegger I, Arnold C, Fankhauser CD, Chun FK, van der Poel H, Gandaglia G, Wiegel T, van den Bergh RCN, Tilki D; EAU-YAU Prostate Cancer Working Group. European Association of Urology Biochemical Recurrence Risk Classification as a Decision Tool for Salvage Radiotherapy-A Multicenter Study. Eur Urol. 2024 Feb;85(2):164-170. doi: 10.1016/j.eururo.2023.05.038. Epub 2023 Jun 22. PMID: 37355358.
- van den Bergh RC, van Casteren NJ, van den Broeck T, Fordyce ER, Gietzmann WK, Stewart F, MacLennan S, Dabestani S, Bellmunt J, Bolla M, Briers E, Cornford P, Joniau S, Mason MD, Matveev V, van der Poel HG, van der Kwast TH, Rouvière O, Wiegel T, Lam TB, Mottet N. Role of Hormonal Treatment in Prostate Cancer Patients with Nonmetastatic Disease Recurrence After Local Curative Treatment: A Systematic Review. Eur Urol. 2016 May;69(5):802-20. doi: 10.1016/j.eururo.2015.11.023. Epub 2015 Dec 12. PMID: 26691493.
- Freedland SJ, De Giorgi U, Gleave M, Rosbrook B, Shen Q, Sugg J, Haas GP, Shore ND. A phase 3 randomised study of enzalutamide plus leuprolide and enzalutamide monotherapy in high-risk non-metastatic hormone-sensitive prostate cancer with rising PSA after local therapy: EMBARK study design. BMJ Open. 2021 Aug 12;11(8):e046588. doi: 10.1136/bmjopen-2020-046588. PMID: 34385241; PMCID: PMC8362713.