(UroToday.com) The 2025 Colombian Urological Society (SCU) Annual Meeting held in Cartagena, Colombia, between August 20th and August 23rd was host to the AUA Prostate Cancer Course. Dr. Luis Salgado in a crossfire debated against treatment of the Primary and Metastasis-Directed Therapy in patients with low-volume Hormone-Sensitive Metastatic Prostate Cancer.
Dr. Salgado opened his talk highlighting the natural progression from localized disease, where 76% of patients are treated with surgery or radiation to biochemical recurrence in 38%, and eventual progression to metastatic castration-sensitive disease in 45% of those. He emphasized timely escalation of therapy across states of resistance, including the use of androgen receptor pathway inhibitors (ARPIs), chemotherapy, and radiopharmaceuticals, while underscoring the need to prioritize bone health throughout the disease course. Where does metastasis-directed therapy fit into this continuum?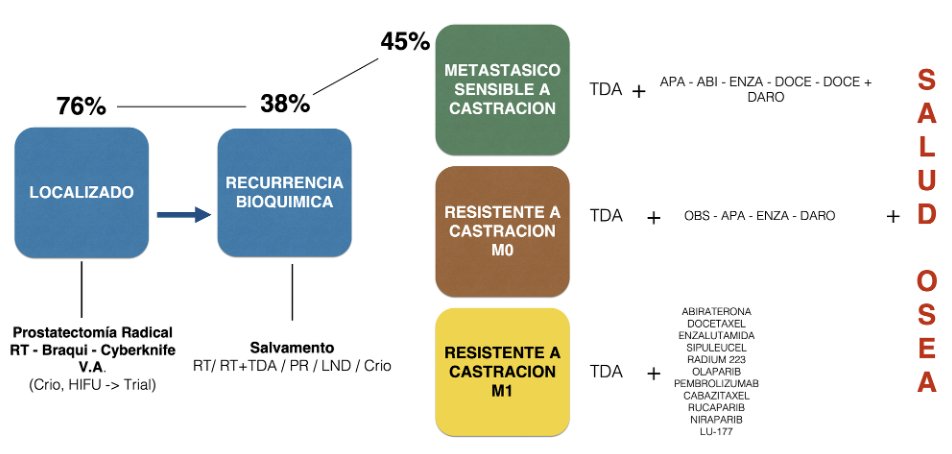
Patients with de novo, high-volume metastatic hormone-sensitive prostate cancer (mHSPC) have significantly worse outcomes, with a median overall survival (OS) of just 3.6 years, compared to 4.3 years in those with low-volume de novo disease. In contrast, patients with metachronous metastases, particularly those with low-volume disease, fare significantly better, with a mOS of 7.7 years. These data underscore the heterogeneity of metastatic prostate cancer and the importance of stratifying patients based not only on volume, but also timing of metastatic presentation.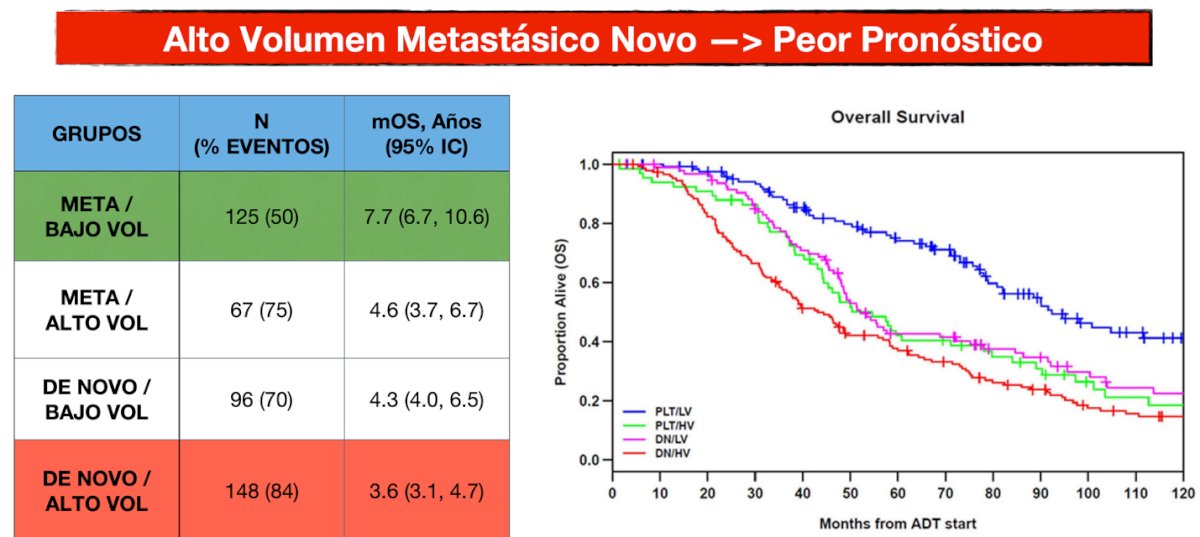
Patients with mHSPC present across a spectrum from those initially diagnosed with localized disease who later progress, to newly diagnosed individuals with synchronous metastatic involvement, including visceral or nodal sites. Despite advances in systemic therapy, outcomes remain poor for many: the 5-year overall survival rate is only 27% and drops below 7% at 10 years. Furthermore, nearly two-thirds (67%) of patients experience disease progression within the first year, underscoring the aggressive nature of mCSPC and the need for early, intensified treatment strategies.
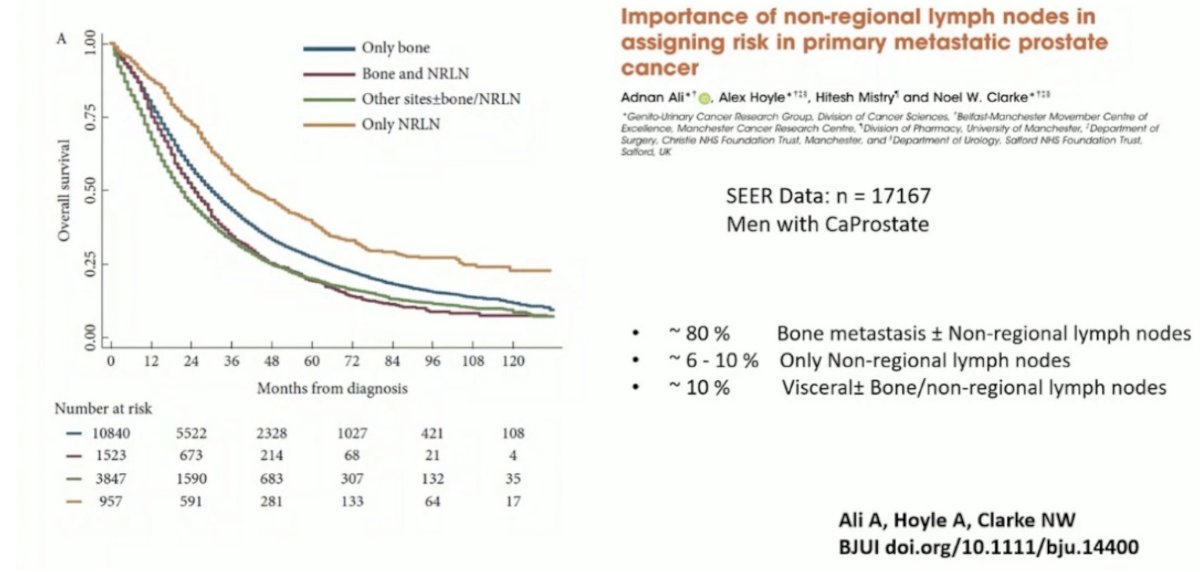
Dr. Salgado highlighted the prognostic significance of the site of metastasis in men with de novo metastatic prostate cancer. Drawing from SEER data on over 17,000 patients, he emphasized that approximately 80% present with bone metastases, often with or without non-regional lymph node (NRLN) involvement. However, a smaller subset (6–10%) present with metastases limited to NRLNs, and around 10% have visceral metastases with or without bone or NRLN involvement. Survival outcomes varied notably by site: patients with isolated NRLN metastases had the most favorable survival, followed by those with bone-only disease, while those with visceral involvement fared worst as outlined below.1
The definitions of high-risk and high-volume mHSPC differ. High-risk disease (LATITUDE) is defined by ≥2 of the following: Gleason ≥8, ≥3 bone lesions, or measurable visceral metastases. High-volume disease (CHAARTED) requires visceral metastases and/or ≥4 bone lesions, with at least one beyond the spine or pelvis. While overlapping, these categories are not interchangeable. Notably, the treatment landscape has evolved considerably over the past decade, culminating in the incorporation of triplet therapy as a standard option in appropriately selected patients.
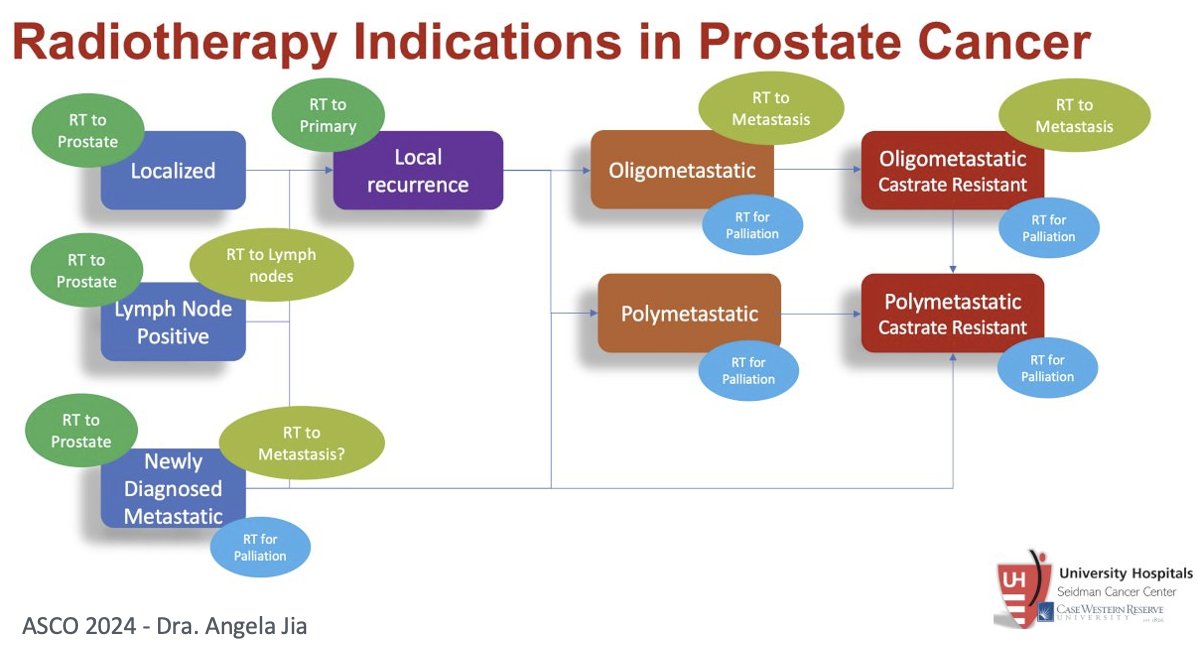
Dr. Salgado highlighted a slide presented by Dr. Angela Jia outlining the spectrum of radiotherapy indications in prostate cancer, from localized disease to metastatic settings. RT to the prostate is a mainstay for localized disease, lymph node–positive cases and select patients with newly diagnosed metastatic disease. For local recurrences, RT may be directed to the primary tumor, while in the oligometastatic setting, it may be used for metastasis-directed therapy or palliation. In the polymetastatic state both hormone-sensitive and castration-resistant RT is generally palliative, though metastasis-directed approaches may be considered in oligometastatic castrate-resistant disease. This framework underscores how radiotherapy remains relevant across the disease continuum, with intent shifting from curative to palliative as disease burden and resistance increase.
Dr. Salgado emphasized that metastasis-directed therapy (MDT) is not a concept unique to prostate cancer, with evidence of benefit across multiple tumor types as shown below. MDT, often delivered as stereotactic body radiotherapy (SBRT) has consistently demonstrated improvements in progression-free survival (PFS), with hazard ratios in prostate cancer trials such as STOMP, ORIOLE, EXTEND, and ARTO ranging from 0.25 to 0.48.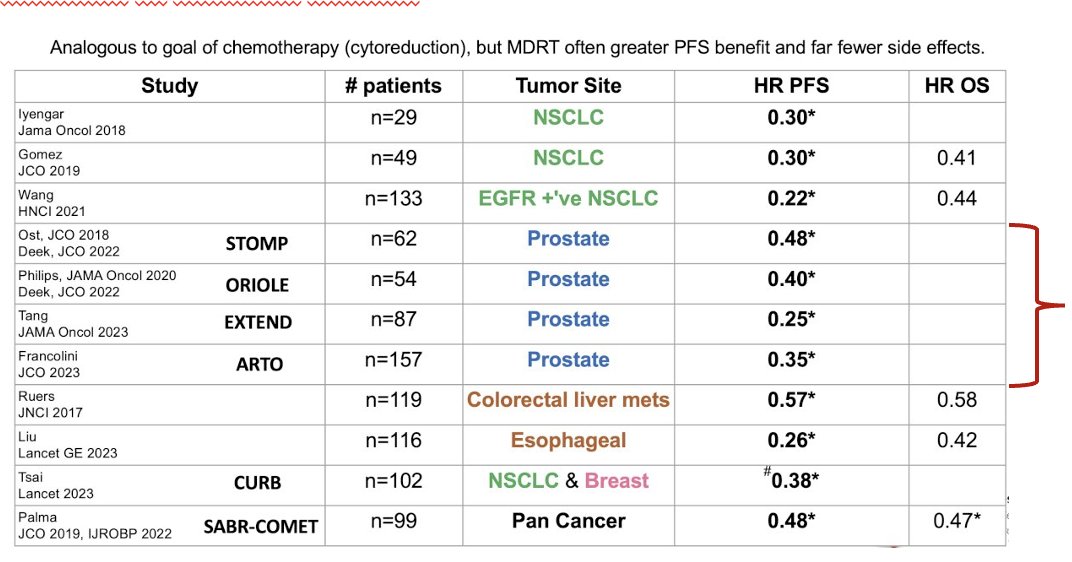
This raises key clinical questions: What is the therapeutic goal in each scenario? Is the intent to delay systemic therapy, achieve durable control, or both? And importantly, does the volume of disease, oligometastatic versus polymetastatic, fundamentally influence outcomes and treatment decisions? The data suggest that while MDT can be effective in carefully selected patients, tailoring its use based on disease burden and biology remains essential.
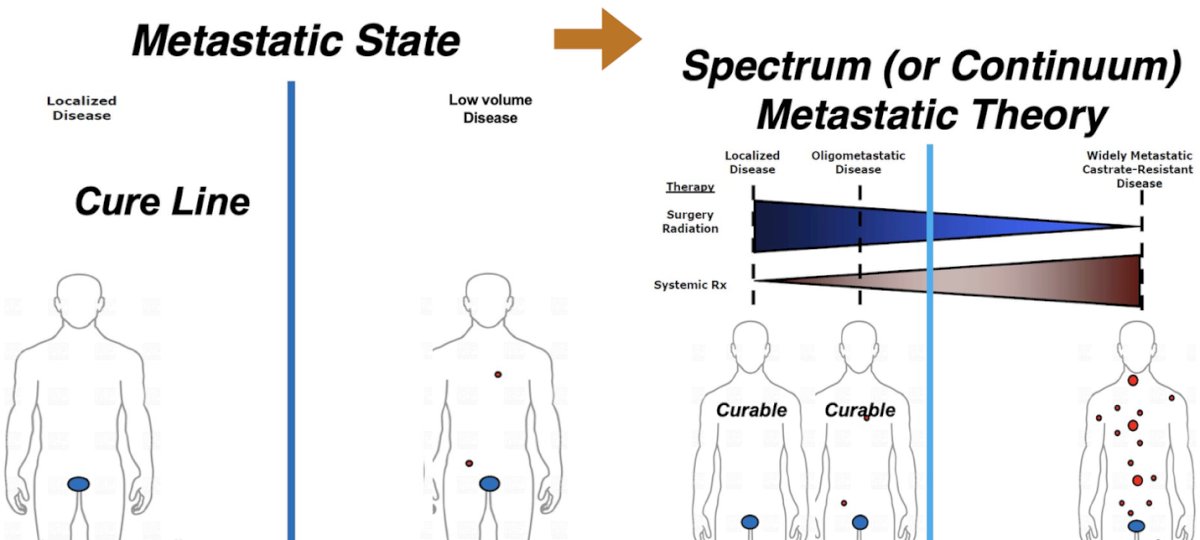
The treatment paradigm for metastatic prostate cancer is shifting from a binary concept, localized versus metastatic, toward a spectrum or continuum model. Traditionally, crossing the “cure line” into metastatic disease implied incurability, with therapy aimed primarily at palliation. In the spectrum-based approach, low-volume or oligometastatic disease is viewed as a potentially curable state, where aggressive local and metastasis-directed therapies, such as surgery or radiation, may meaningfully alter the disease course.
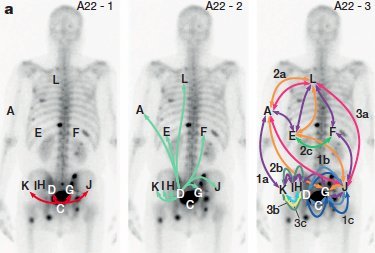
He highlighted the concept that metastatic cells may return to the primary tumor or “self-seed.” Both the primary tumor and established metastases can generate new metastatic deposits. According to the “clone theory,” altering the natural history of oligometastatic disease may require treating both the primary lesion and all detectable metastases, aiming to disrupt the cycle of seeding and reseeding that drives progression as shown below.
Dr Salgado stressed the urgent need to standardize the definition of oligometastatic disease. Should it be based on the number of lesions three, five, or another threshold? Should it be limited to bone metastases, include visceral sites, or focus only on lesions considered “treatable”? Achieving consensus on these criteria is essential for harmonizing clinical trial designs and guiding patient selection in practice.
Historically, oligometastatic prostate cancer was defined as fewer than five lesions, excluding visceral metastases. The proposed evolution of this definition expands the threshold to fewer than ten lesions and includes visceral sites. Dr. Salgado noted that ASTRO continues to use outdated criteria, despite repeated calls from the global oncology community to update and standardize these definitions an ongoing point of contention that impacts both research and clinical practice.
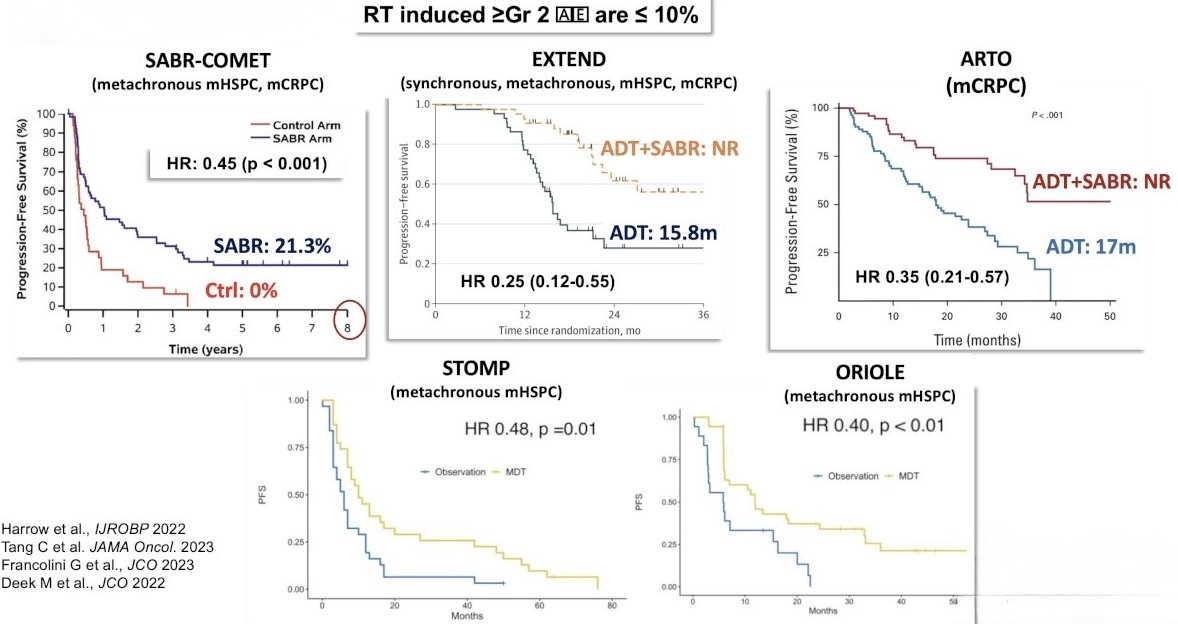
Reviewing the SABR-COMET, EXTEND, ARTO, STOMP, and ORIOLE trials, Dr. Salgado highlighted consistent improvements in progression-free survival with metastasis-directed radiotherapy across both hormone-sensitive and castration-resistant settings, with median PFS gains most pronounced when SBRT and ADT. Importantly, grade ≥2 adverse events were ≤10% across studies, underscoring the favorable safety profile of MDT. However, Dr. Salgado emphasized the glaring gap, OS data are largely absent or immature, leaving unanswered whether these PFS gains ultimately translate into longer life.2-5
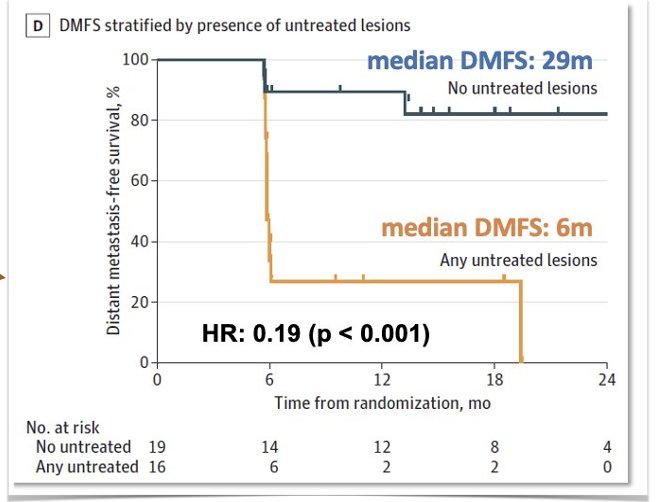
Notably, the ORIOLE trial demonstrated a striking difference in distant metastasis–free survival (DMFS) when all PSMA PET–detected lesions were treated compared to when any lesions were left untreated. Patients with complete lesion treatment achieved a median DMFS of 29 months, versus only 6 months for those with untreated lesions (HR 0.19; p < 0.001). These findings underscore the importance of comprehensive lesion coverage in metastasis-directed therapy to maximize disease control.4
Dr. Salgado also reviewed the WOLVERINE meta-analysis, which pooled data from five randomized controlled trials: SABR-COMET, STOMP, ORIOLE, EXTEND, and ARTO encompassing 472 patients with oligometastatic prostate cancer. Patients were randomized to MDT with or without standard of care versus SOC alone. While the analysis reinforced the consistent progression-free survival benefit of MDT across trials, there was no statistically significant improvement in overall survival.

Dr. Salgado cautioned that the potential benefits of MDT must be weighed against its toxicity profile. A recent systematic review and meta-analysis in JAMA Oncology reported acute grade 3–5 adverse events in 1.2% of patients (95% CI, 0.0–3.8) and late grade 3–5 events in 1.7% (95% CI, 0.2–4.6). While these pooled rates are low, he emphasized that certain series have reported toxicity rates as high as 23%, underscoring the need for careful patient selection, meticulous treatment planning, and realistic counseling about potential risks.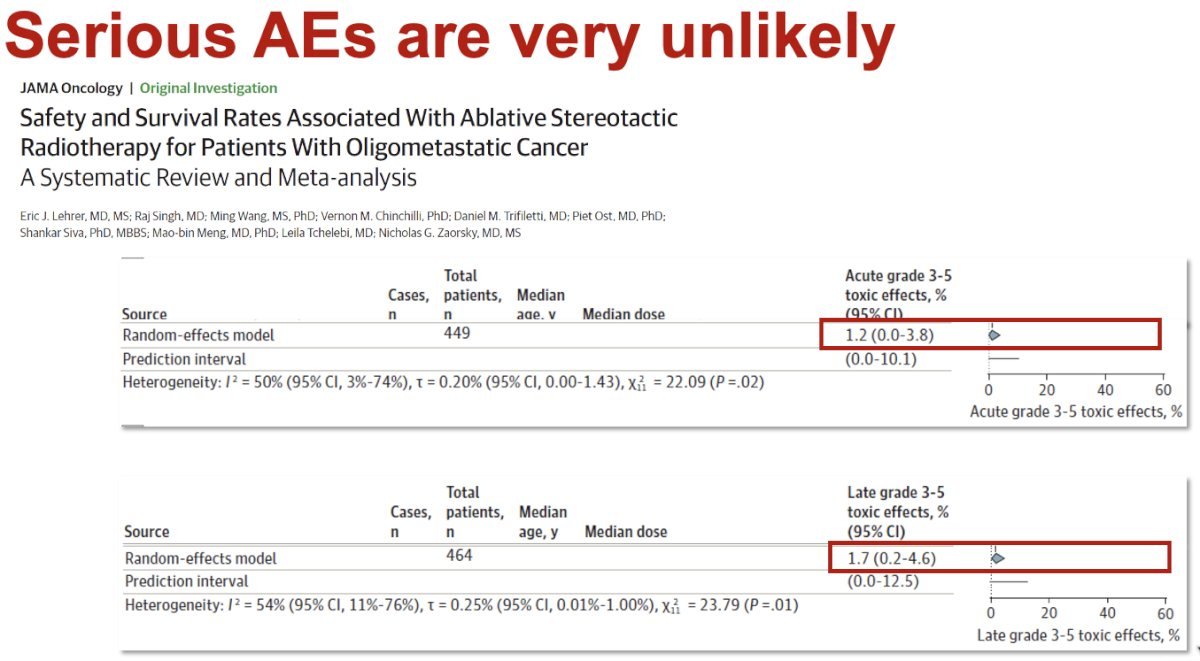
Dr. Salgado then asked a practical question: are we truly treating the full metastatic burden? Most MDT trials were designed and staged with conventional imaging, not PSMA PET. If PSMA PET detects additional lesions that were invisible on baseline scans, many patients in those studies likely had untreated disease from the start. In that scenario, the “clone/selfseeding” rationale for comprehensive lesion ablation weakens MDT may delay progression but is less likely to change the natural history.
Dr. Salgado closed his presentation with several key takeaways:
- Metastasis-directed therapy can improve certain oncologic parameters, but not the primary endpoints that matter most, such as overall survival.
- Extrapolating outcomes from conventional imaging–based trials to PSMA PET–staged patients is not appropriate, given the differences in detection sensitivity.
- MDT is not yet the new standard of care for oligometastatic prostate cancer; the current standard remains systemic intensification.
- The definition of oligometastatic disease should evolve, potentially toward a concept of “treatable lesions” rather than fixed lesion counts.
- While the approach is promising, the ultimate promise of MDT in altering long-term outcomes has not yet been fulfilled.
Presented by: Luis Salgado, MD, Urologic Oncologist at Clinica Universitaria Colombia (CUC), Bogota D.C., Colombia.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Colombian Urological Society (SCU) Annual Meeting held in Cartagena, Colombia, between August 20th and August 23rd
Reference:
- Ali A, Hoyle A, Mistry H, Clarke NW. Importance of non-regional lymph nodes in assigning risk in primary metastatic prostate cancer. BJU Int. 2019 Jan;123(1):65-73. doi: 10.1111/bju.14400. Epub 2018 Jun 13. PMID: 29777564.
- Palma DA, Olson R, Harrow S, Gaede S, Louie AV, Haasbeek C, et al. Stereotactic ablative radiotherapy for the comprehensive treatment of oligometastatic cancers: long-term results of the SABR-COMET phase II randomized trial. J Clin Oncol. 2020;38(25):2830–8.
- Ost P, Reynders D, Decaestecker K, Fonteyne V, Lumen N, De Bruycker A, et al. Surveillance or metastasis-directed therapy for oligometastatic prostate cancer recurrence (STOMP): five-year results of a randomized phase II trial. J Clin Oncol. 2020;38(10_suppl):10. BioMed CentralNaturePMC
- Phillips R, Shi WY, Deek M, Radwan N, Lim SJ, Antonarakis ES, et al. Outcomes of observation vs stereotactic ablative radiation for oligometastatic prostate cancer: the ORIOLE phase 2 randomized clinical trial. JAMA Oncol. 2020;6(5):650–9. PMC+1Nature
- Tang C, Sherry AD, Haymaker C, Bathala T, Liu S, Fellman B, et al. Addition of metastasis-directed therapy to intermittent hormone therapy for oligometastatic prostate cancer: the EXTEND phase 2 randomized clinical trial. JAMA Oncol. 2023;9(6):825–34.