(UroToday.com) The 2025 Colombian Urological Society (SCU) Annual Meeting held in Cartagena, Colombia, between August 20th and August 23rd was host to the AUA Prostate Cancer Course. Dr. Alvaro Muñoz in a crossfire debate supported Treatment of the Primary and Metastasis-Directed Therapy in patients with low-volume Hormone-Sensitive Metastatic Prostate Cancer.
Dr. Muñoz began by defining oligometastatic disease from a radiation oncologist’s perspective as “an intermediate state between local and systemic disease, in which radical local treatment of the primary tumor and all metastatic lesions has curative potential.” He noted that the most widely accepted definition involves 1–5 lesions, though important questions remain: should the primary tumor be included in cases of de novo oligometastatic disease, and should lymph nodes be counted individually or by chain?
Notably, there are two potential ways to define oligometastatic cancer. The first frames it as a state in which there is a realistic possibility of cure, though the definition of “cure” is not always clear, and the probability decreases as the number of metastases increases. The second defines it as a setting in which the patient can benefit from ablative therapy, raising the question of whether patients with more than 10 metastases might still be candidates for such treatment, even if they do not meet the classic “oligo” criteria.
Moreover, there is a clear need to standardize the terminology used to describe oligometastatic disease. This includes differentiating between:
- Synchronous (de novo): Oligometastatic disease present at diagnosis, with an untreated primary tumor.
- Metachronous (oligorecurrence): Recurrence with limited metastases occurring months or years after definitive treatment of the primary.
- Oligoprogression: A small number of lesions progress while the rest of the disease remains controlled on systemic therapy.
- Oligopersistence: Persistent, limited metastases after systemic treatment, without progression but still detectable.
For decades, androgen deprivation therapy (ADT) was the only treatment option for patients with newly diagnosed metastatic prostate cancer. Oligometastatic hormone-sensitive prostate cancer is a distinct subtype with a more favorable prognosis than widespread metastatic disease. The treatment approach differs depending on whether the disease is synchronous or metachronous. There are important discrepancies between conventional imaging and PSMA PET in staging, which influence treatment decisions. As for which patients might ultimately benefit from local therapy, there is still no consensus highlighted by differing interpretations from trials such as CHAARTED and LATITUDE.1,2
The rationale for local therapy in metastatic prostate cancer is based on several concepts. Tumor progression follows the “seed and soil” model, where both the cancer cells (“seeds”) and the microenvironment (“soil”) influence metastasis. Prostate tumors can release factors that promote metastatic spread; local radiotherapy may reduce tumor burden and circulating factors, potentially enhancing the effectiveness of systemic treatments. Additionally, radiation may stimulate an antitumor immune response, further contributing to systemic disease control.3
The SABR-COMET phase 2 randomized trial compared stereotactic ablative radiotherapy (SABR) with standard palliative care in patients with oligometastatic cancers. The study demonstrated a significant improvement in both overall survival (OS) and progression-free survival (PFS) for the SABR arm. At five years, OS was notably higher in the SABR group, and PFS curves showed a clear and sustained separation favoring SABR (p = 0.006 for OS; p = 0.001 for PFS). These results suggested that, in well-selected patients, ablative treatment of all visible metastases could meaningfully delay disease progression and potentially extend survival.4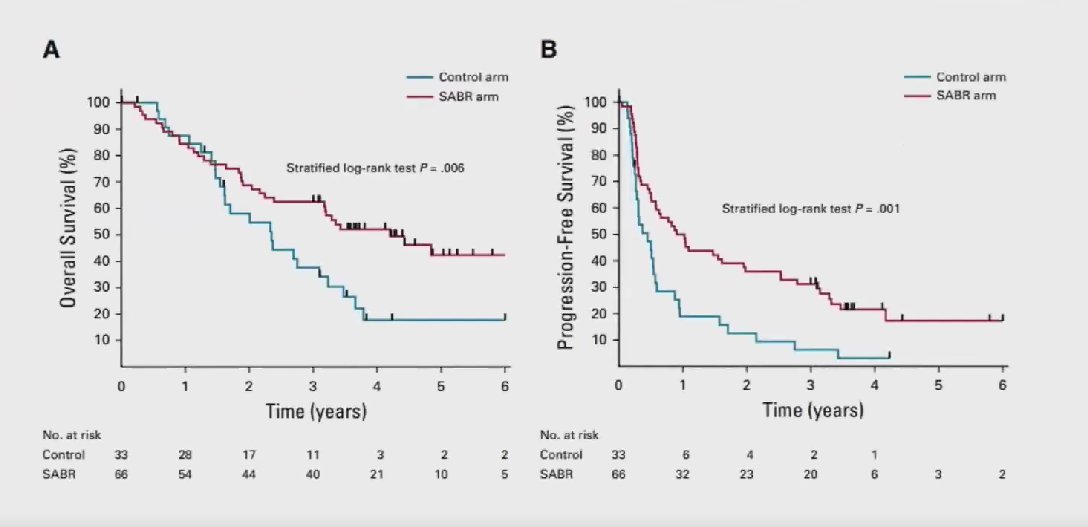
Moreover, Dr. Muñoz highlighted a systematic review and meta-analysis that examined prospective trials of SABR or surgery for oligometastatic hormone-sensitive prostate cancer. The review concluded that MDT consistently improved progression-free survival compared with observation, with a favorable toxicity profile in well-selected patients. However, the evidence for overall survival benefit remains limited, and the authors emphasized the need for biomarker-driven patient selection and standardized definitions to optimize future research and clinical practice. A Summary of the findings is presented below.5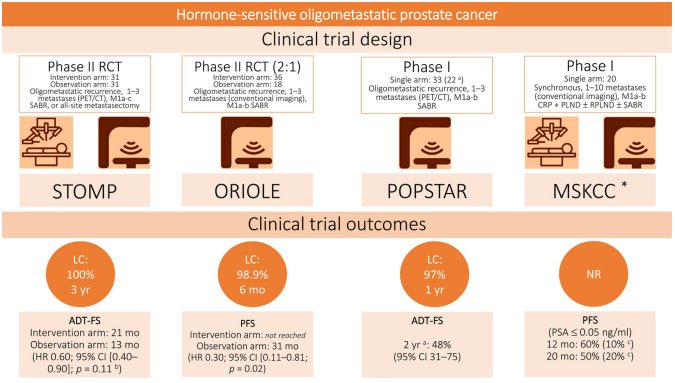
The combined long-term analysis of the STOMP and ORIOLE trials demonstrated a sustained benefit of MDT over observation in patients with oligometastatic castration-sensitive prostate cancer as reflected by improved progression-free survival across follow-up. Importantly, genomic alterations appeared to hold prognostic value in this population of patients; those without certain high-risk mutations, such as HRR alterations, experienced more favorable outcomes. These findings suggest that integrating biomarker evaluation into future studies could refine patient selection, optimizing the therapeutic impact of MDT.6 
At ASTRO 2024, investigators presented a multicenter, international retrospective analysis validating a digital pathology–based MMAI model in 222 men with castration-sensitive oligometastatic prostate cancer (≤5 metastases), including patients from the STOMP and ORIOLE phase II trials. The MMAI score was evaluated as a predictive tool for benefit from metastasis-directed therapy. In both trials, patients with a high but not low MMAI score (above 0.33) experienced improved metastasis-free survival when treated with SBRT, suggesting that MMAI could help identify those most likely to benefit from targeted metastasis ablation.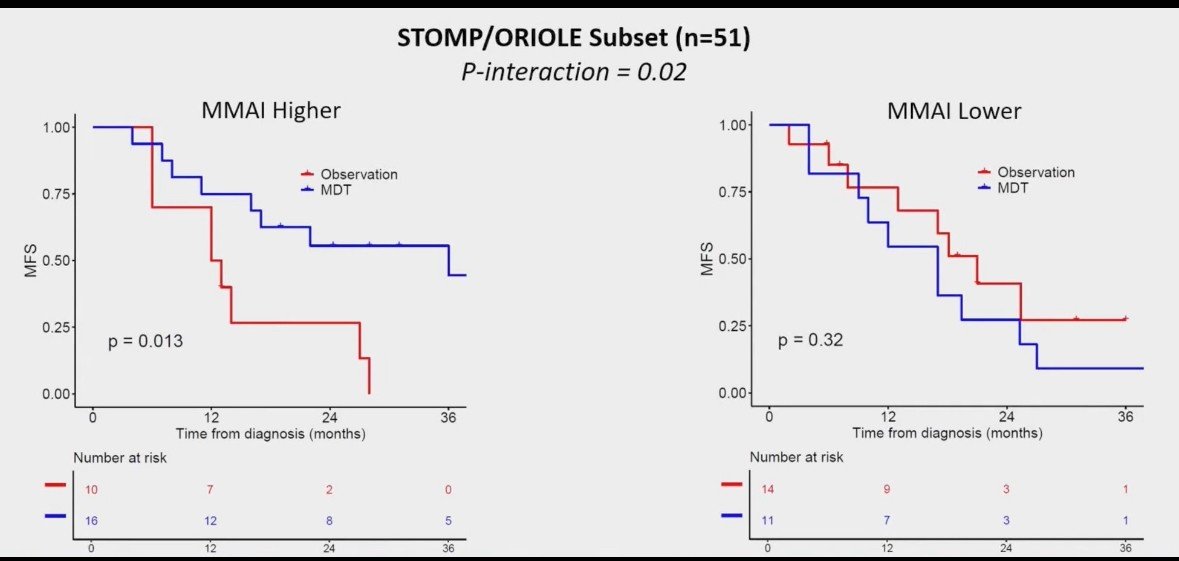
Similarly, in the EXTEND phase 2 trial, adding MDT to intermittent hormone therapy in patients with oligometastatic prostate cancer significantly improved progression-free survival compared to hormone therapy alone. At a median follow-up of 22.1 months, the hazard ratio for progression or death was 0.25 (95% CI, 0.12–0.55; p < 0.001). Median PFS was 15.8 months in the hormone therapy–only arm, whereas it was not reached in the combined therapy arm.7
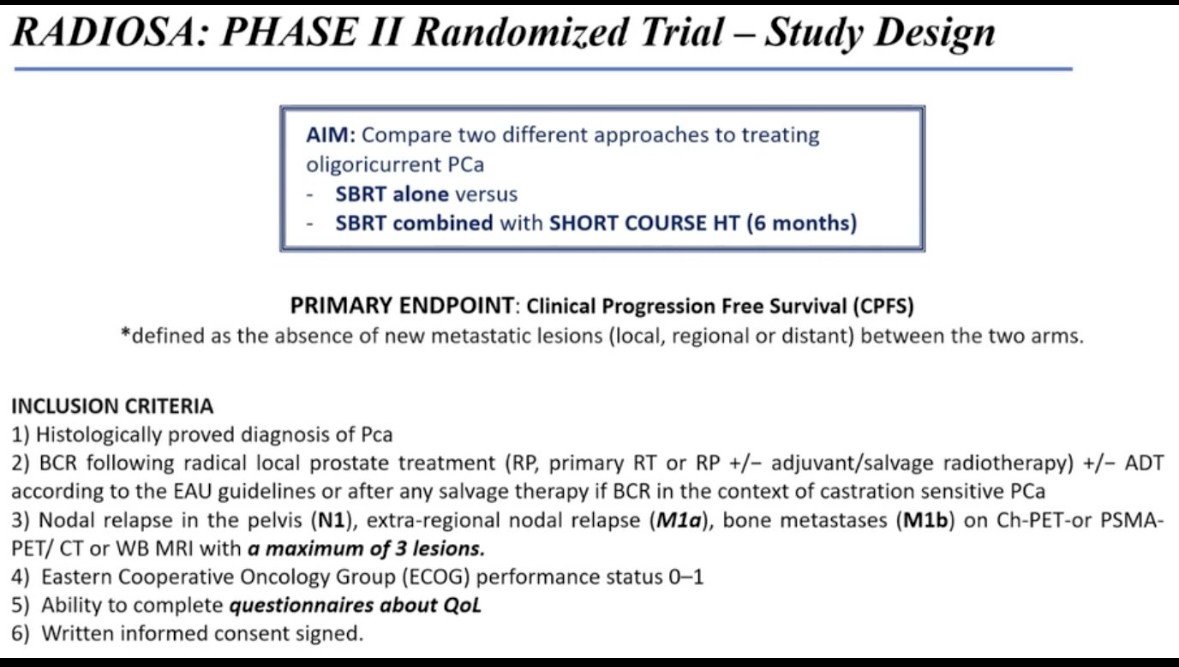
Dr. Muñoz highlighted the RADIOSA phase II randomized trial, designed to compare two treatment strategies for oligorecurrent prostate cancer: stereotactic body radiotherapy (SBRT) alone versus SBRT combined with a short course (six months) of hormone therapy.
The RADIOSA trial showed a significant improvement in clinical progression rates for the group receiving six months of ADT combined with SBRT compared to SBRT alone. Most recurrences were oligorecurrent, with only 6 polymetastatic cases in group B (experimental) compared to 15 in group A. Nearly all patients in group B achieved testosterone recovery at one year, supporting the safety and efficacy of adding short-term ADT to SBRT. Upcoming analyses of quality-of-life questionnaires will help clarify patient-reported outcomes, while molecular studies on collected biological samples aim to identify genomic signatures to refine risk stratification and guide personalized treatment in oligometastatic prostate cancer.
The TRANSFORM phase II trial reported five-year outcomes of fractionated SBRT in 199 patients with oligometastatic prostate cancer, including those with up to 5 lesions. Results showed similar outcomes for patients with 4–5 lesions compared to those with 1–3 lesions. At a median follow-up of 67.9 months, 19% of participants had not required systemic treatment intensification, and two patients maintained undetectable PSA levels. No grade 3 or higher treatment-related toxicities were observed. These findings support SBRT-based multidisciplinary therapy as an effective approach to delay systemic therapy in oligometastatic prostate cancer. However, randomized trials are needed to directly compare SBRT-based strategies with standard androgen deprivation therapy to determine the survival impact of deferring systemic treatment.8
The CHEERS trial, evaluated the combination of immunotherapy and radiotherapy in solid tumors to explore the potential for an abscopal effect where local radiotherapy induces systemic tumor regression at distant, non-irradiated sites. Preliminary results did not show a statistically significant improvement in progression-free survival (median 2.8 vs 4.4 months; p = 0.7) or overall survival (p = 0.4). These findings suggest that, at least in this setting, combining radiotherapy with immunotherapy did not produce a clear abscopal benefit, highlighting the need for further studies to identify optimal patient populations and treatment sequencing.9
Looking to the future, multiple phase III trials are testing SABR in oligometastatic prostate cancer both in patients with prior local control of the primary and those without. These studies are powered for hard endpoints (metastasis-free survival, overall survival, and treatment-free survival) and incorporate modern staging with PSMA PET, stratifying by de novo vs. recurrent disease and by systemic therapy backbone. Their results should clarify whether SABR meaningfully extends survival beyond the consistent PFS gains seen to date, how it integrates with intensification strategies, and which patients derive the greatest benefit. Results are eagerly awaited.
PSMA PET has emerged as the preferred imaging modality for prostate cancer, enabling accurate detection of metastatic disease. In this setting, MDT is a valid option for patients with up to five lesions, either in de novo oligometastatic disease, where it should be integrated with systemic therapy, or in castration-resistant oligoprogressive disease, where its use aims to delay systemic therapy change and prolong disease control.
Dr. Munoz concluded his presentation with the following take-home messages:
- Some patients with oligometastatic disease may be cured, but this is not the only outcome that we should be aiming for.
- Principle: treat all detectable metastases whenever possible.
- SBRT has the strongest current randomized evidence among metastasis-directed therapies.
- Uncertainty remains regarding optimal patient selection, dosing, treatment planning, and integration with systemic therapy.
- Patients with low disease burden and highly effective systemic options may not show early benefits.
- Despite the lack of level I evidence, metastasis-directed therapy is widely used in clinical practice.
- There is a need for more consistent treatment indications and radiotherapy practices while awaiting results from ongoing randomized prospective trials.
Presented by: Alvaro Muñoz, MD, Radiation Oncologist at Fundacion Santa Fe de Bogota, Bogota, Colombia.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Colombian Urological Society (SCU) Annual Meeting held in Cartagena, Colombia, between August 20th and August 23rd
Reference:
- Sweeney CJ, Chen YH, Carducci M, Liu G, Jarrard DF, Eisenberger M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N Engl J Med. 2015;373(8):737-46.
- Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev BY, et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med. 2017;377(4):352-60.
- Parker C, Castro E, Fizazi K, Heidenreich A, Ost P, Procopio G, Tombal B, Gillessen S; ESMO Guidelines Committee. Electronic address: . Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020 Sep;31(9):1119-1134. doi: 10.1016/j.annonc.2020.06.011. Epub 2020 Jun 25. PMID: 32593798.
- Palma DA, Olson R, Harrow S, Gaede S, Louie AV, Haasbeek C, Mulroy L, Lock M, Rodrigues GB, Yaremko BP, Schellenberg D, Ahmad B, Senthi S, Swaminath A, Kopek N, Liu M, Moore K, Currie S, Schlijper R, Bauman GS, Laba J, Qu XM, Warner A, Senan S. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J Clin Oncol. 2020 Sep 1;38(25):2830-2838. doi: 10.1200/JCO.20.00818. Epub 2020 Jun 2. PMID: 32484754; PMCID: PMC7460150.
- Connor MJ, Smith A, Miah S, Shah TT, Winkler M, Khoo V, et al. Targeting oligometastasis with stereotactic ablative radiation therapy or surgery in metastatic hormone-sensitive prostate cancer: a systematic review of prospective clinical trials. Eur Urol Oncol. 2020;3(5):582-93.
- Deek MP, Van der Eecken K, Sutera P, Deek RA, Fonteyne V, Mendes AA, et al. Long-term outcomes and genetic predictors of response to metastasis-directed therapy versus observation in oligometastatic prostate cancer: analysis of STOMP and ORIOLE trials. J Clin Oncol. 2022;40(29):3377-86.
- Tang C, Sherry AD, Haymaker C, Bathala T, Liu S, Fellman B, et al. Addition of metastasis-directed therapy to intermittent hormone therapy for oligometastatic prostate cancer: the EXTEND phase 2 randomized clinical trial. JAMA Oncol. 2023;9(6):825-34.
- See AW, Conway P, Frydenberg M, Haxhimolla H, Costello AJ, Moon D, et al. Five-year outcomes of fractionated stereotactic body radiotherapy for oligometastatic prostate cancer from the TRANSFORM phase II trial. Int J Cancer. 2024;155(7):1248-56. doi:10.1002/ijc.35052.
- Spass M, Sundahl N, Rottey S, Reynders D, Coeckelbergh E, Ost P, et al. Immuno-radiotherapy in solid tumors: preliminary results of the randomized phase 2 CHEERS trial. Eur J Cancer. 2021;161(Suppl 1):S491. doi:10.1016/S0959-8049(21)06981-4.