(UroToday.com) The 2025 Colombian Urological Society (SCU) Annual Meeting held in Cartagena, Colombia, between August 20th and August 23rd. was host to the AUA Prostate Cancer Course. Dr. Matthew Cooperberg discussed the use of Artificial Intelligence in Screening, Diagnosis, and Treatment of Prostate Cancer.
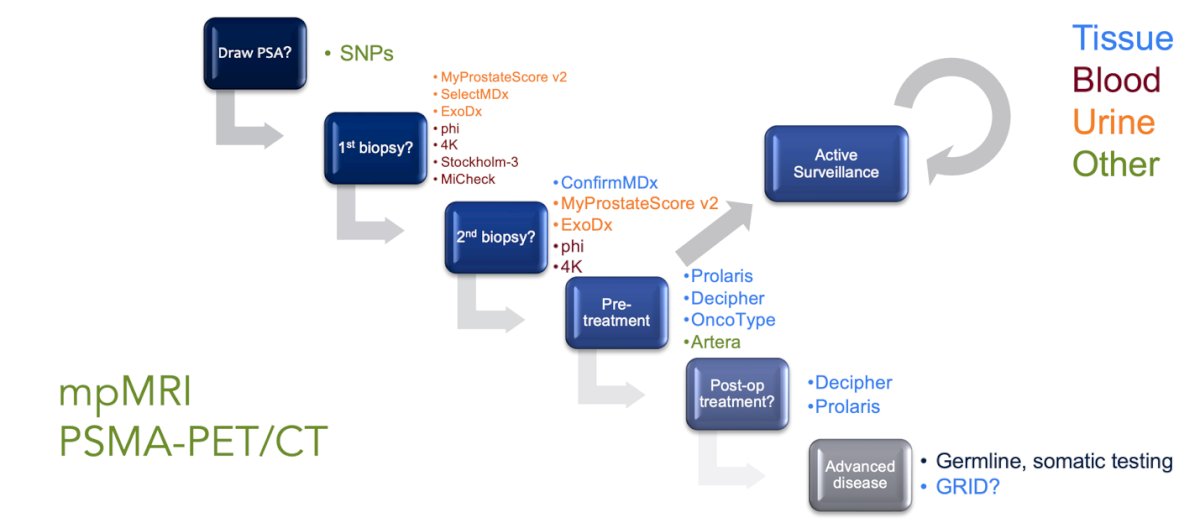
Dr. Cooperberg highlighted that prostate cancer diagnosis and management now rely on a wide range of tools spanning tissue, blood, urine, and imaging. Beyond PSA and SNPs, assays such as MyProstateScore v2, SelectMDx, ExoDx, phi, 4Kscore, Stockholm-3, and MiCheck can refine risk after biopsy, while confirmatory tests like ConfirmMDx and genomic classifiers including Prolaris, Decipher, OncoType, and Artera inform both pre-treatment and post-operative decisions.
The current landscape of FDA-approved AI in the U.S. highlights rapid growth in computer-aided detection and diagnosis tools, particularly for imaging. The majority of clearances since 2016 have been for triage systems (CADt), followed by detection (CADe) and diagnosis (CADx). While the bulk of approvals target conditions like ICH, breast cancer, and lung cancer, prostate cancer is beginning to emerge with a smaller but notable presence in CADx and hybrid tools. This trend underscores the expanding role of AI in oncology and suggests that prostate cancer applications are likely to grow as technology and validation efforts advance, as shown below.1 
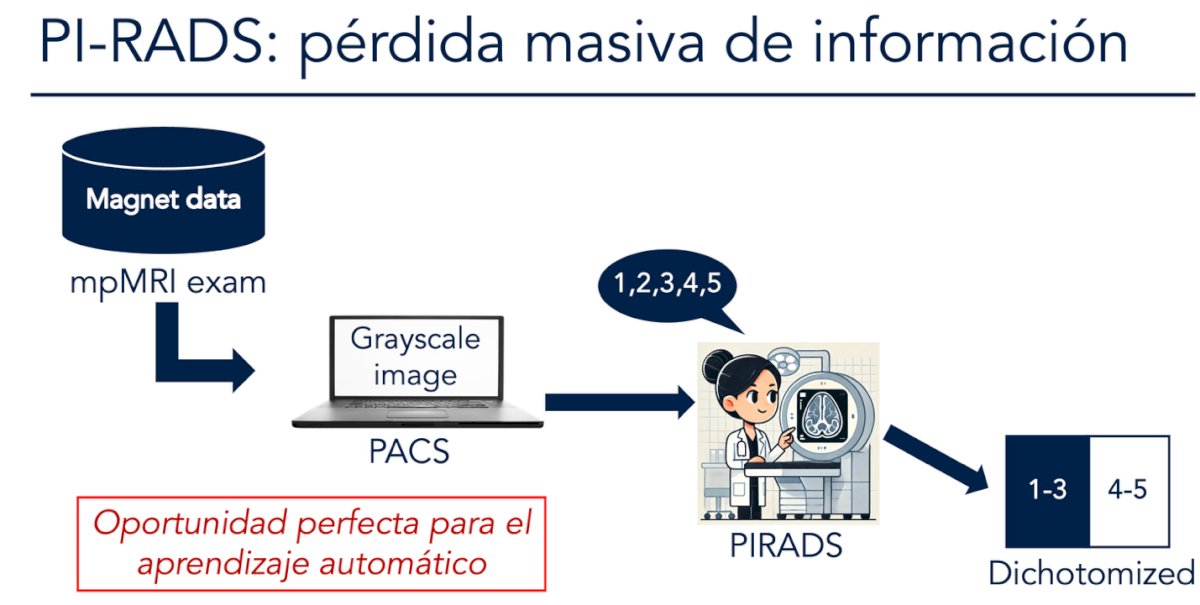
Dr. Cooperberg emphasized that PI-RADS, while widely used, results in a substantial loss of information. mpMRI data are simplified into grayscale images, assigned PI-RADS scores from 1–5, and then often dichotomized into low (1–3) versus high (4–5) suspicion. This reduction strips away the rich underlying imaging data, creating variability in interpretation and limiting precision. He highlighted this as a “perfect opportunity” for machine learning approaches, which could leverage the full spectrum of imaging data to improve consistency and accuracy in prostate cancer detection.2
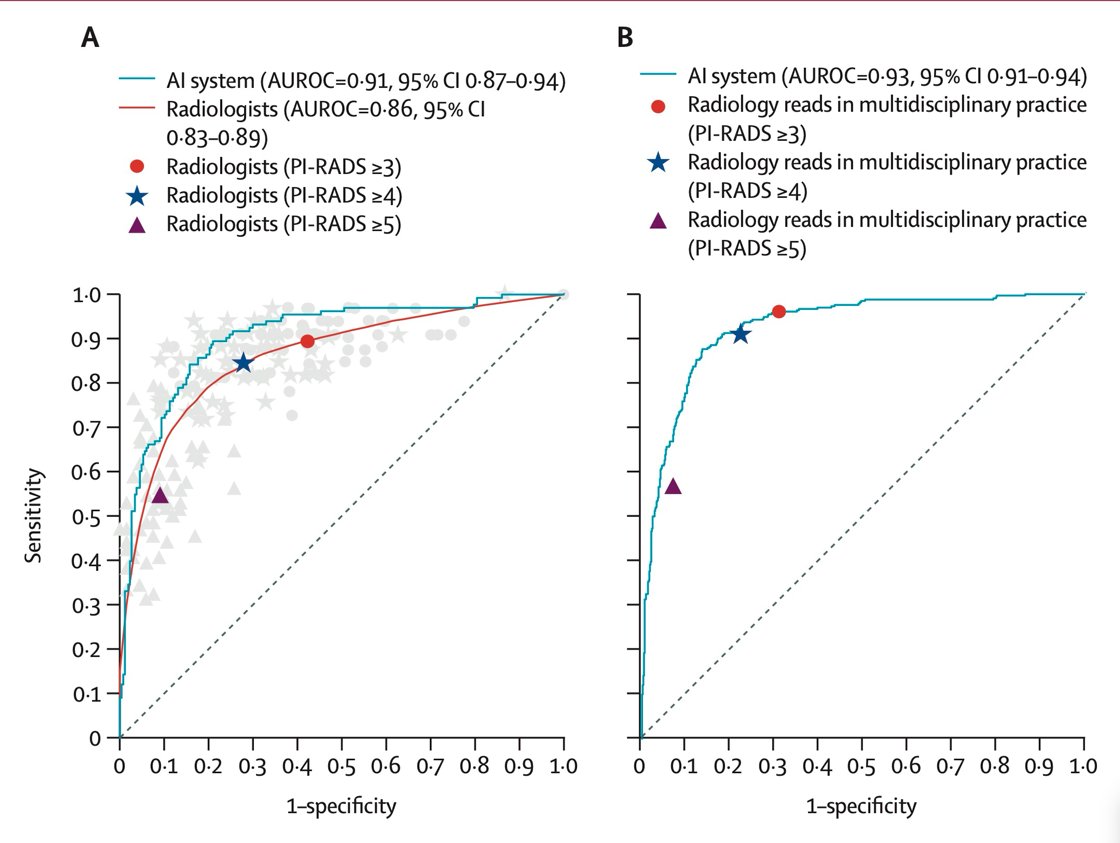
Dr. Cooperberg highlighted the PI-CAI trial, a landmark study led by Saha et al, which directly compared AI with radiologists in prostate cancer detection on MRI. The study included over 10,000 MRI cases from 9,129 patients across four European centers, with long-term follow-up and histopathological validation. Out of 293 AI models submitted through an open competition, the top five were refined and benchmarked against 62 radiologists from 45 centers in 20 countries, each evaluating 400 test cases with likelihood scores and PI-RADS.2
Notably, in the PI-CAI study, pooled radiologists achieved an AUC of 0.86 with a PPV of 53% and NPV of 90%, whereas the AI system outperformed them with an AUC of 0.91, PPV of 68%, and NPV of 94%. Importantly, AI detected nine additional clinically significant cancers, reduced 57 false positives, and avoided eight GG1 overdiagnoses, underscoring its potential to enhance diagnostic accuracy and reduce unnecessary interventions compared to standard PI-RADS assessments as illustrated below.2
This analysis showed that AI not only improved human reader performance but, when applied alone, actually outperformed radiologists in prostate MRI interpretation. The PI-CAI system achieved an AUROC of 0.947, compared to 0.882 for radiologists, with combined AI + reader performance reaching 0.916. These results highlight that AI can function as a supportive tool to enhance radiologist accuracy or potentially take the lead in independent interpretation.3
Furthermore, the aPROMISE platform demonstrated significant advantages over manual interpretation of PSMA PET. It markedly reduced reporting time while maintaining high accuracy across staging domains. Sensitivity and specificity reached 100% in multiple categories, including miT and miM1b staging, with slightly lower sensitivity observed for nodal (88%) and miM1c disease (63%). Compared to manual reads, aPROMISE offered faster, more consistent, and highly reproducible assessments, underscoring its value as an AI-enabled tool in prostate cancer imaging.4
A consensus statement on PI-RADS AI highlighted the need for standardized reporting and validation criteria when applying artificial intelligence to prostate MRI. Key requirements include adherence to PI-RADS v2/v2.1, inclusion of all necessary tabular elements, at least 2 years of MRI or histologic follow-up for negative cases, and transparent reporting of reader expertise and performance metrics. Additional standards involve documenting protocol deviations, describing scoring schemes for bpMRI, specifying annotation software, and ensuring comparisons between independent training and testing datasets as summarized in the table below. Notably, together, these measures aim to ensure rigor, reproducibility, and reliability in AI applications for prostate MRI.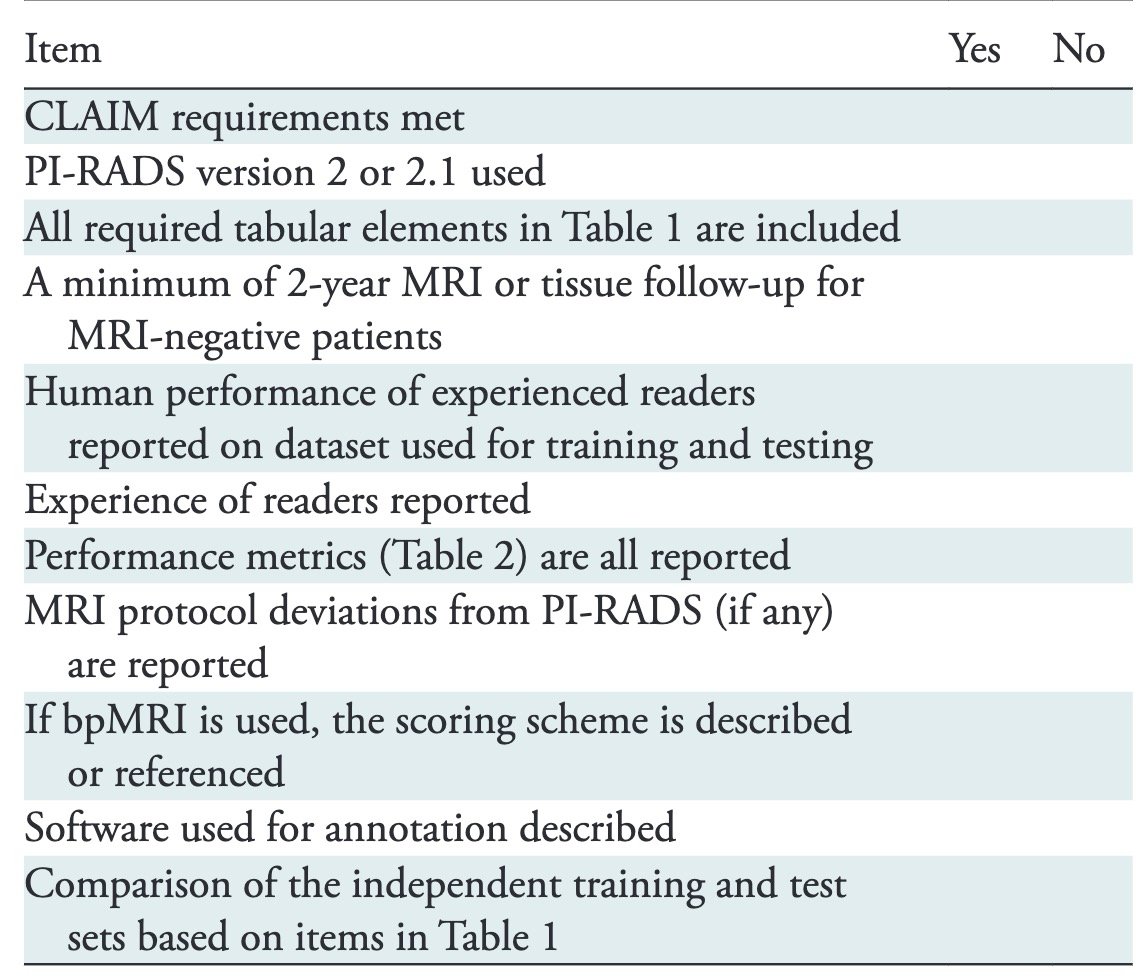
Dr. Cooperberg highlighted the limitations of interobserver reproducibility in Gleason grading. In a multi-institutional study agreement was strong for “easy” cases (κ=0.76) but dropped significantly in “controversial” cases (κ=0.27). This variability underscores the challenges of pathology interpretation in early-stage prostate cancer, particularly for patients managed with active surveillance, where subtle differences in grading can directly impact treatment decisions.5
The PANDA challenge is a large international competition aimed at improving the reproducibility and accuracy of prostate cancer grading using AI. The study involved 1,010 teams and 1,290 participants from 65 countries, generating over 17,000 submissions based on 10,616 biopsies for development and 2,009 biopsies for independent validation, with data sourced from the USA, Netherlands, and Sweden. This initiative demonstrated the potential of AI to match or surpass pathologists in Gleason grading while reducing interobserver variability and promoting greater consistency in prostate cancer diagnosis worldwide Dr. Cooperberg highlighted this algorithm is opened source and can be easily downloaded and access anywhere in the world.6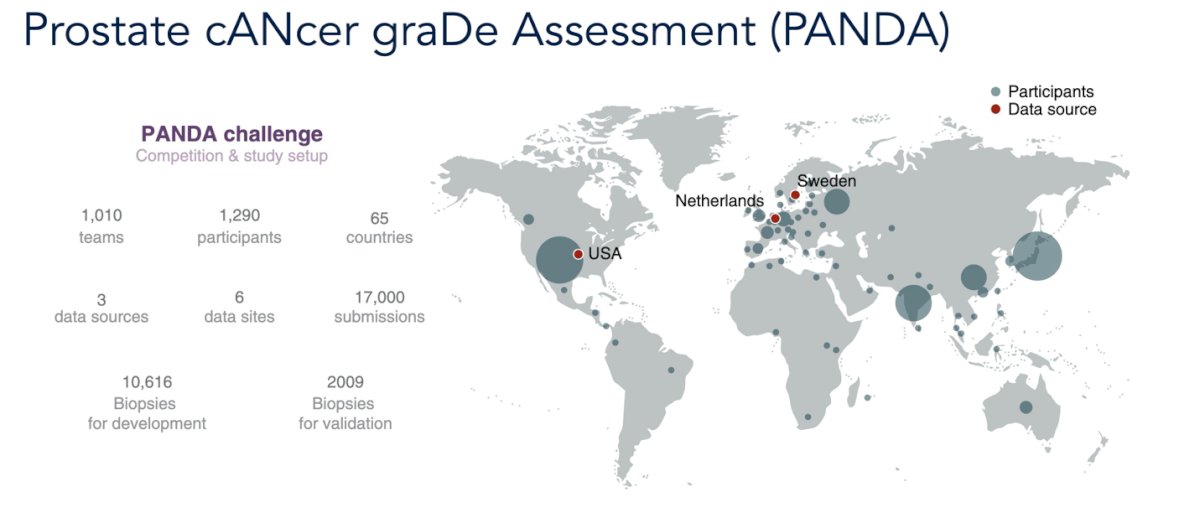
Notably, the PANDA challenge further showed that AI algorithms outperformed general pathologists in Gleason grading reproducibility. While general pathologists demonstrated moderate agreement, algorithms achieved substantially higher concordance with expert consensus, highlighting the potential of AI to provide more consistent and reliable prostate cancer grading across diverse clinical settings.6
Dr. Cooperberg underscored the need to rethink histology in prostate cancer, highlighting that not all patterns within the same grade group carry the same prognosis. Features such as Gleason 5, large cribriform, intraductal, complex intraluminal papillary, grade 3 stromogenic, and complex anastomosing cordlike patterns were identified as clearly unfavorable, while everything else was considered favorable. Importantly, the data showed that while most grade group 2 cases were favorable, higher-grade groups were increasingly dominated by these unfavorable morphologies, reinforcing the need to move beyond traditional Gleason grouping when assessing risk.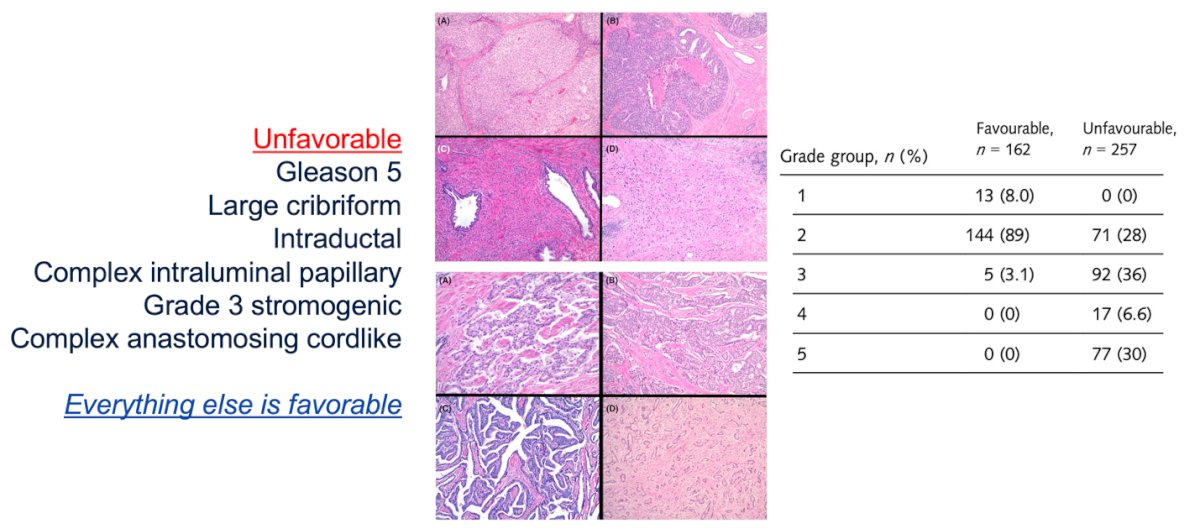
In this study, unfavorable histologic features were the true drivers of poor outcomes. The survival curves clearly demonstrated that patients with “favorable histology” had excellent long-term outcomes, with no cases of metastasis observed in this group. In contrast, unfavorable histology was consistently associated with higher rates of biochemical recurrence, distant metastasis, and prostate cancer–specific mortality, underscoring the importance of integrating histologic patterns not just grade groups into risk stratification and clinical decision-making.7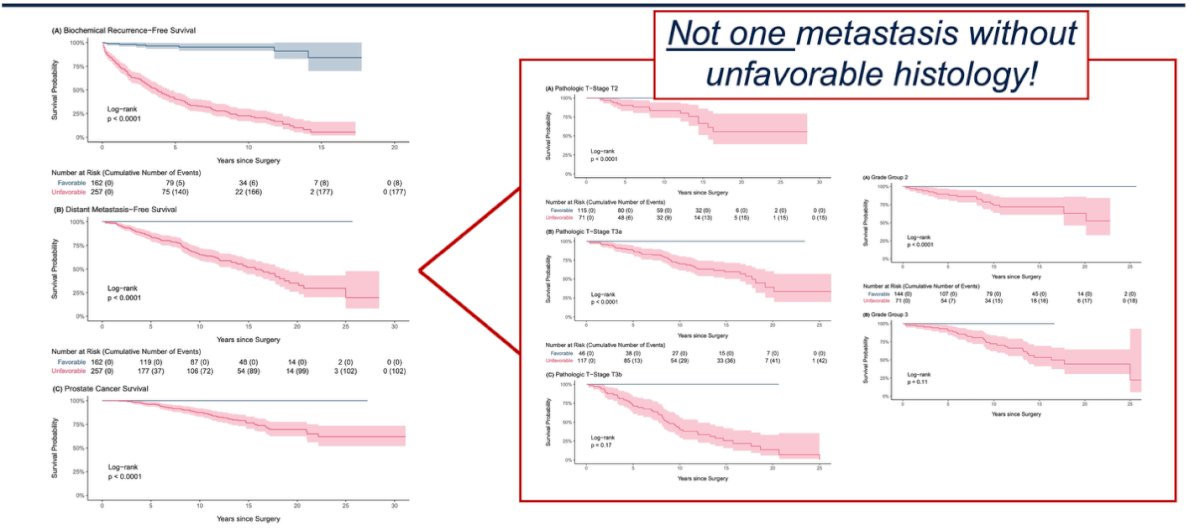
AI in pathology Dr. Cooperberg presented data from the AIRA Prostate AI platform, showing its ability to refine pathology interpretation in men on active surveillance. In a cohort of 169 Johns Hopkins patients with GG1 disease, AI reclassification to ≥GG2 was independently associated with a higher risk of upgrading (HR 1.71, 95% CI 1.05–2.78; p=0.03) on multivariable analysis, even after adjusting for biopsy year, PSA density, and MRI findings as illustrated below.
Moreover, Dr. Cooperberg highlighted the role of Pathomiq’s AI-based pathology platform in risk stratification. Patients classified as high-risk by the Pathomiq score had significantly worse biochemical recurrence-free survival (HR 4.35, p<0.0001) and metastasis-free survival (HR 4.66, p=0.00039) compared to low-risk patients. Importantly, decision curve analysis demonstrated that Pathomiq outperformed traditional clinical models (CAPRA-S, Kattan, Partin) and even genomic scores, providing greater net clinical benefit for predicting 3-year and 5-year risk of recurrence or metastasis.8
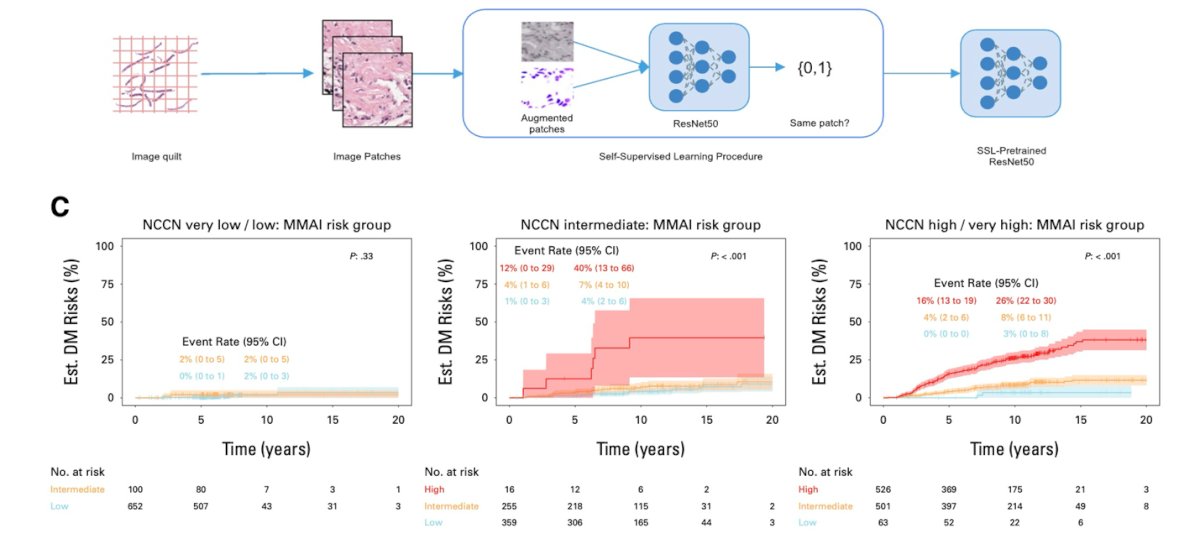
Dr. Cooperberg also highlighted the role of morphology-based multimodal AI (MMAI) in refining risk stratification. By leveraging histology patches and self-supervised learning, MMAI was able to separate patients into distinct prognostic groups. Importantly, while men with very low/low NCCN risk had excellent outcomes regardless of MMAI, those with intermediate or high/very high NCCN risk were further stratified by MMAI, with markedly higher risks of distant metastasis seen in the MMAI “high” groups.9 This suggests that MMAI may add important prognostic value beyond standard clinical classifiers, particularly in identifying the subset of men most likely to benefit from treatment intensification.
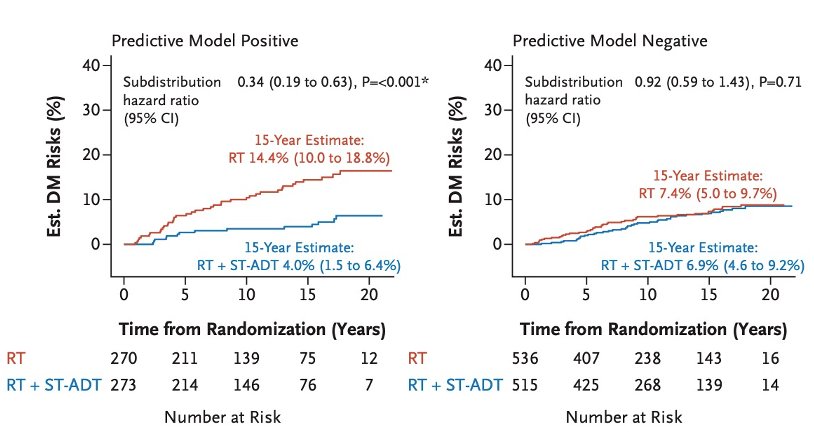
Lastly, Dr. Cooperberg presented a study using ARTERA AI to identify which patients derive long-term benefit from adding short-term ADT to radiotherapy. In predictive model–positive patients, RT + ST-ADT significantly reduced the 15-year risk of distant metastasis (14.4% with RT vs. 4.0% with RT + ST-ADT). In contrast, model-negative patients had similar outcomes regardless of ADT, underscoring the potential of ARTERA AI to personalize therapy by selecting patients most likely to benefit while sparing others unnecessary toxicity.9
Dr. Cooperberg concluded his presentation with the following take-home messages:
- AI is revolutionizing health care, and development will only accelerate, maybe in ways we cannot anticipate.
- AI tools can spread globally at very low cost.
- These developments may be good for patients if we deploy them carefully.
- I would not recommend my kids become pathologists or radiologists, but AI will radically affect all our workflows eventually and we need to be ready when the time comes.
Presented by: Matthew R. Cooperberg. MD, MPH, Professor of Urology and Epidemiology & Biostatistics and Helen Diller Family Chair in Urology at the University of California, San Francisco, CA
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Colombian Urological Society (SCU) Annual Meeting held in Cartagena, Colombia, between August 20th and August 23rd
References:
- McNamara SL, Yi PH, Lotter W. The clinician-AI interface: intended use and explainability in FDA-cleared AI devices for medical image interpretation. NPJ Digit Med. 2024 Mar 26;7(1):80. doi: 10.1038/s41746-024-01080-1. PMID: 38531952; PMCID: PMC10966080.
- Saha A, Bosma JS, Twilt JJ, van Ginneken B, Bjartell A, Padhani AR, Bonekamp D, Villeirs G, Salomon G, Giannarini G, Kalpathy-Cramer J, Barentsz J, Maier-Hein KH, Rusu M, Rouvière O, van den Bergh R, Panebianco V, Kasivisvanathan V, Obuchowski NA, Yakar D, Elschot M, Veltman J, Fütterer JJ, de Rooij M, Huisman H; PI-CAI consortium. Artificial intelligence and radiologists in prostate cancer detection on MRI (PI-CAI): an international, paired, non-inferiority, confirmatory study. Lancet Oncol. 2024 Jul;25(7):879-887. doi: 10.1016/S1470-2045(24)00220-1. Epub 2024 Jun 11. PMID: 38876123; PMCID: PMC11587881.
- Twilt JJ, Saha A, Bosma JS, Padhani AR, Bonekamp D, Giannarini G, van den Bergh R, Kasivisvanathan V, Obuchowski N, Yakar D, Elschot M, Veltman J, Fütterer J, Huisman H, de Rooij M; PI-CAI Consortium. AI-Assisted vs Unassisted Identification of Prostate Cancer in Magnetic Resonance Images. JAMA Netw Open. 2025 Jun 2;8(6):e2515672. doi: 10.1001/jamanetworkopen.2025.15672. PMID: 40512493; PMCID: PMC12166490.
- Enei Y, Yanagisawa T, Okada A, Kuruma H, Okazaki C, Watanabe K, Lenzo NP, Kimura T, Miki K. Comparison of diagnostic performance between manual diagnosis following PROMISE V2 and aPROMISE utilizing Ga/F-PSMA PET/CT. Ann Nucl Med. 2025 Jul 15. doi: 10.1007/s12149-025-02086-9. Epub ahead of print. PMID: 40665093.
- McKenney JK, Simko J, Bonham M, True LD, Troyer D, Hawley S, Newcomb LF, Fazli L, Kunju LP, Nicolas MM, Vakar-Lopez F, Zhang X, Carroll PR, Brooks JD; Canary/Early Detection Research Network Prostate Active Surveillance Study Investigators. The potential impact of reproducibility of Gleason grading in men with early-stage prostate cancer managed by active surveillance: a multi-institutional study. J Urol. 2011 Aug;186(2):465-9. doi: 10.1016/j.juro.2011.03.115. Epub 2011 Jun 15. PMID: 21679996.
- Bulten W, Kartasalo K, Chen PC, Ström P, Pinckaers H, Nagpal K, Cai Y, Steiner DF, van Boven H, Vink R, Hulsbergen-van de Kaa C, van der Laak J, Amin MB, Evans AJ, van der Kwast T, Allan R, Humphrey PA, Grönberg H, Samaratunga H, Delahunt B, Tsuzuki T, Häkkinen T, Egevad L, Demkin M, Dane S, Tan F, Valkonen M, Corrado GS, Peng L, Mermel CH, Ruusuvuori P, Litjens G, Eklund M; PANDA challenge consortium. Artificial intelligence for diagnosis and Gleason grading of prostate cancer: the PANDA challenge. Nat Med. 2022 Jan;28(1):154-163. doi: 10.1038/s41591-021-01620-2. Epub 2022 Jan 13. PMID: 35027755; PMCID: PMC8799467.
- Nguyen JK, Harik LR, Klein EA, Li J, Corrigan D, Liu S, Chan E, Hawley S, Auman H, Newcomb LF, Carroll PR, Cooperberg MR, Filson CP, Simko JP, Nelson PS, Tretiakova MS, Troyer D, True LD, Vakar-Lopez F, Weight CJ, Lin DW, Brooks JD, McKenney JK. Proposal for an optimised definition of adverse pathology (unfavourable histology) that predicts metastatic risk in prostatic adenocarcinoma independent of grade group and pathological stage. Histopathology. 2024 Oct;85(4):598-613. doi: 10.1111/his.15231. Epub 2024 Jun 3. PMID: 38828674; PMCID: PMC11365761.
- Nair SS, Muhammad H, Jain P, Xie C, Pavlova I, Brody R, Huang W, Nakadar M, Zhang X, Basu H, Wilding G, Roy R, Chakravarty D, Tewari AK. A Novel Artificial Intelligence-powered Tool for Precise Risk Stratification of Prostate Cancer Progression in Patients with Clinical Intermediate Risk. Eur Urol. 2025 Jun;87(6):728-729. doi: 10.1016/j.eururo.2024.07.013. Epub 2024 Sep 3. PMID: 39232981.
- Spratt DE, Tang S, Sun Y, Huang HC, Chen E, Mohamad O, Armstrong AJ, Tward JD, Nguyen PL, Lang JM, Zhang J, Mitani A, Simko JP, DeVries S, van der Wal D, Pinckaers H, Monson JM, Campbell HA, Wallace J, Ferguson MJ, Bahary JP, Schaeffer EM, Sandler HM, Tran PT, Rodgers JP, Esteva A, Yamashita R, Feng FY. Artificial Intelligence Predictive Model for Hormone Therapy Use in Prostate Cancer. NEJM Evid. 2023 Aug;2(8):EVIDoa2300023. doi: 10.1056/EVIDoa2300023. Epub 2023 Jun 29. PMID: 38320143; PMCID: PMC11195914.