(UroToday.com) The 2025 Sociedad Colombiana de Urologia annual meeting featured a prostate cancer session and a presentation by Dr. Julian Chavarriaga discussing an update of tumor markers in prostate cancer. Dr. Chavarriaga started his presentation discussing biomarkers in localized and locally advanced prostate cancer. By definition, a tumor marker is a molecular, biological, or physical characteristic that indicates a specific physiological state. Specifically, tumor or biomarkers are used in clinical practice to:
- Identify disease risk
- Diagnose disease and characterize its severity
- Guide intervention strategies
- Monitor the patient’s response to therapy
One of the original prostate cancer risk stratification strategies was developed by Dr. Anthony D’Amico more than 25 years ago, categorizing patients into low, intermediate, and high risk disease:

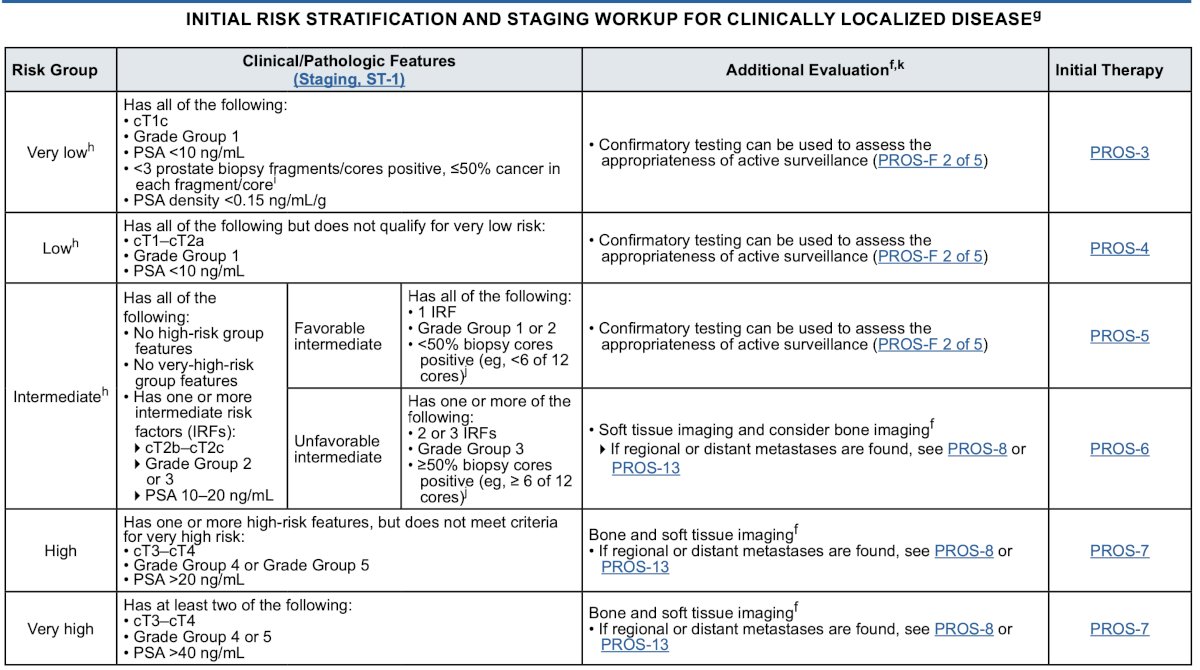
Since then, the NCCN guidelines for prostate cancer risk stratification have become quite robust, with stratification including very low, low, intermediate, high, and very high risk:
Multiparametric MRI is also a valuable tool in risk prognostication of localized prostate cancer. In 2021, Rajwa et al.1 performed a systematic review and meta-analysis of the available data to assess the association of PI-RADS v2 score and risk of biochemical recurrence among patients undergoing primary definitive treatment for prostate cancer. Among patients treated with radical prostatectomy, higher PI-RADS scores were significantly associated with risk of biochemical recurrence (pooled HR 3.06, 95% CI 2.16-4.33). For all studies, the PI-RADS score remained significantly associated with biochemical recurrence (pooled HR, 3.19; 95% CI, 2.28-4.45).
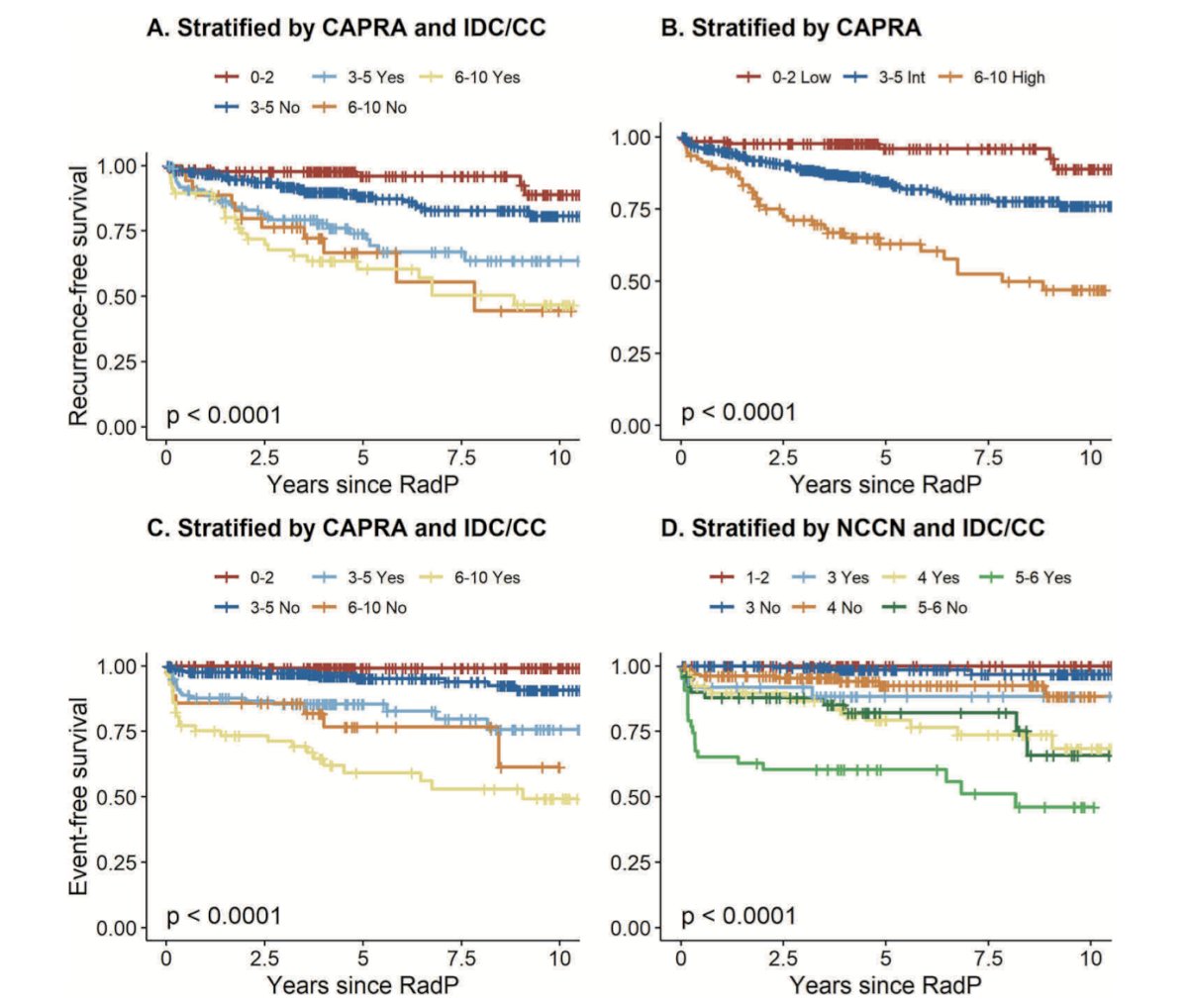
Intraductal carcinoma of the prostate and cribriform differentiation are also biomarkers for biochemical recurrence and event-free survival. This is particularly evident when stratified by CAPRA and NCCN risk groups:
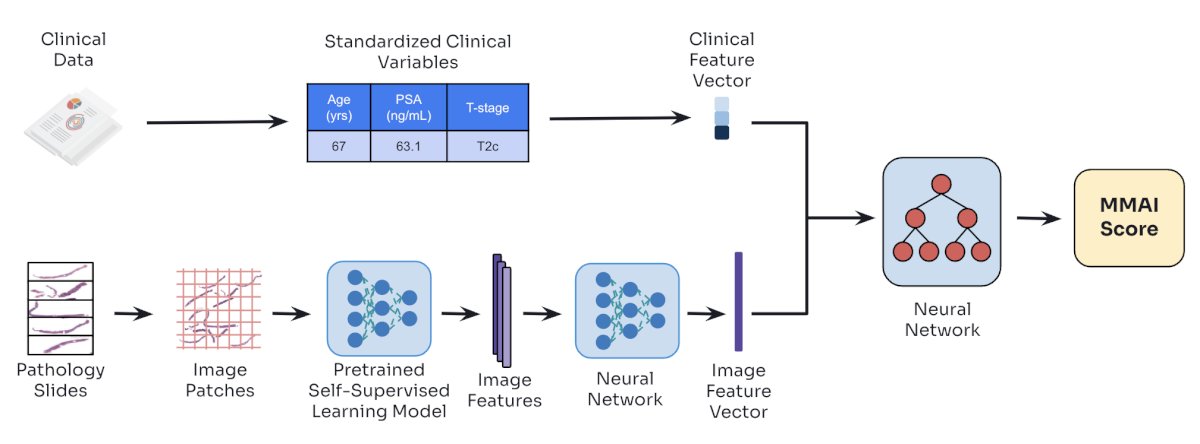
More contemporary biomarkers include the ArteraAI Prostate Test, which uses digital pathology information and MMAI technology to provide a prognostic risk score for an outcome of interest and predicts therapeutic benefit: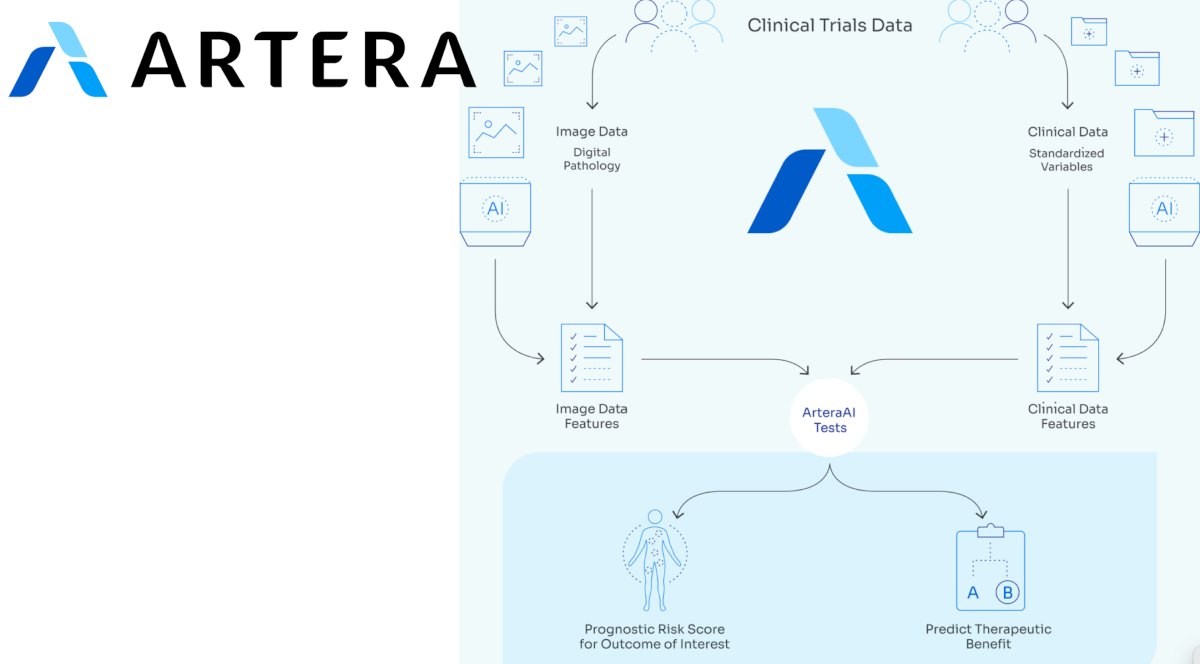
At the 2022 GU ASCO annual meeting, Dr. Spratt and colleagues presented data discussing this first predictive biomarker. For the study, pre-treatment biopsy slides were digitized from five phase III NRG Oncology randomized trials of men receiving radiotherapy with or without androgen deprivation therapy (ADT). The training set to develop the artificial intelligence-derived predictive biomarker included NRG/RTOG 9202, 9413, 9910, and 0126, and was trained to predict distant metastasis. A multimodal deep learning architecture was developed to learn from both clinicopathologic and digital imaging histopathology data and identify differential outcomes by treatment type. After the model was locked, an independent biostatistician performed validation on NRG/RTOG 9408, a phase III randomized trial of radiotherapy +/- 4 months of ADT: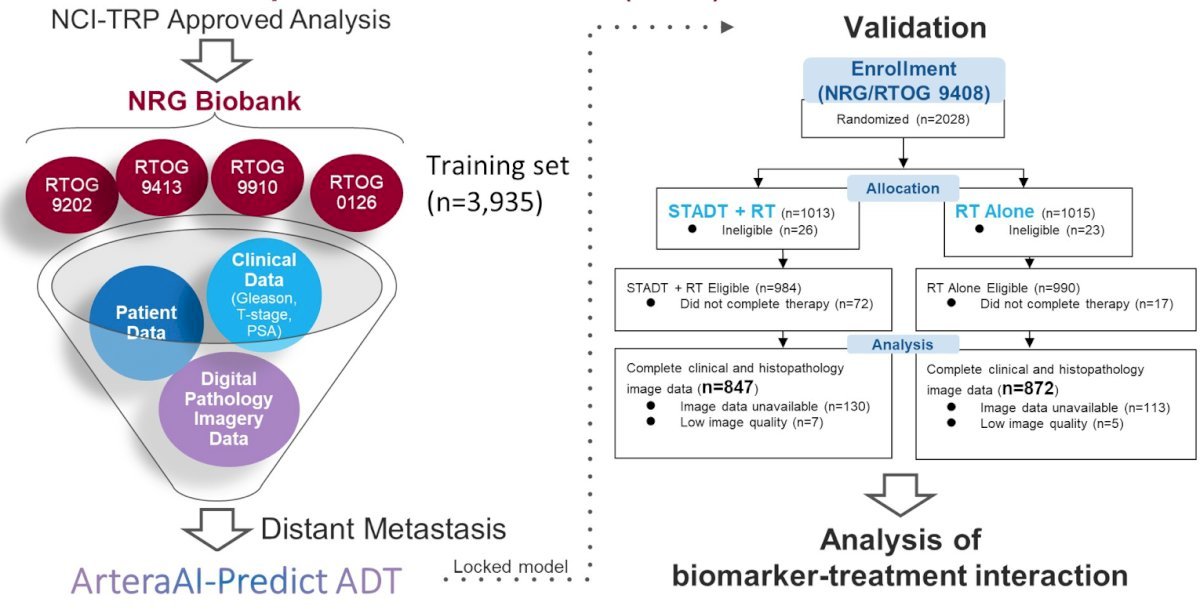
In patients with artificial intelligence-biomarker positive disease (n = 673, 39%), ADT had a greater benefit compared to radiotherapy alone (HR 0.33, 95% CI 0.19 to 0.57). In the biomarker negative subgroup (n = 1046, 61%), the addition of ADT did not improve outcomes over radiotherapy alone (HR 1.00, 95% CI 0.63 to 1.56). The 15-year distant metastasis rate difference between radiotherapy versus radiotherapy + ADT in the biomarker negative group was 0.4% vs biomarker positive group 9.8%:
At the 2025 ASCO annual meeting, Dr. Nicholas James discussed results of the ArteraAI Prostate test to identify potential benefit from second generation androgen receptor pathway inhibitors in high risk non metastatic prostate cancer patients in the STAMPEDE platform. The objective of this analysis was to explore whether a prognostic AI-derived pathology score could identify a subgroup of clinically high-risk patients more likely to benefit from the addition of abiraterone to standard of care therapy. Eligible patients included those with node-positive disease or node-negative disease with at least two high-risk features: T3/T4 staging, Gleason score 8–10, or PSA ≥ 40 ng/mL. The primary endpoint was metastasis free survival, and a secondary endpoint was prostate cancer-specific mortality. The analysis was conducted with a median follow-up of six years, where a total of 781 patients in Arm A (standard of care ADT ± radiotherapy) and 555 patients in Arms G/J (standard of care + abiraterone ± enzalutamide) were included: 
Prognostic MMAI scores were developed using H&E-stained biopsy whole slide images alongside clinical variables such as age, PSA, and T-stage:
Dr. James reported that the MMAI score is prognostic even within clinically high-risk prostate cancer populations. Applying established clinical prognostic cut-offs, 89% (n = 1,189) of M0 patients in the cohort were classified as MMAI high-risk, demonstrating the model's ability to further stratify risk within an already high-risk population: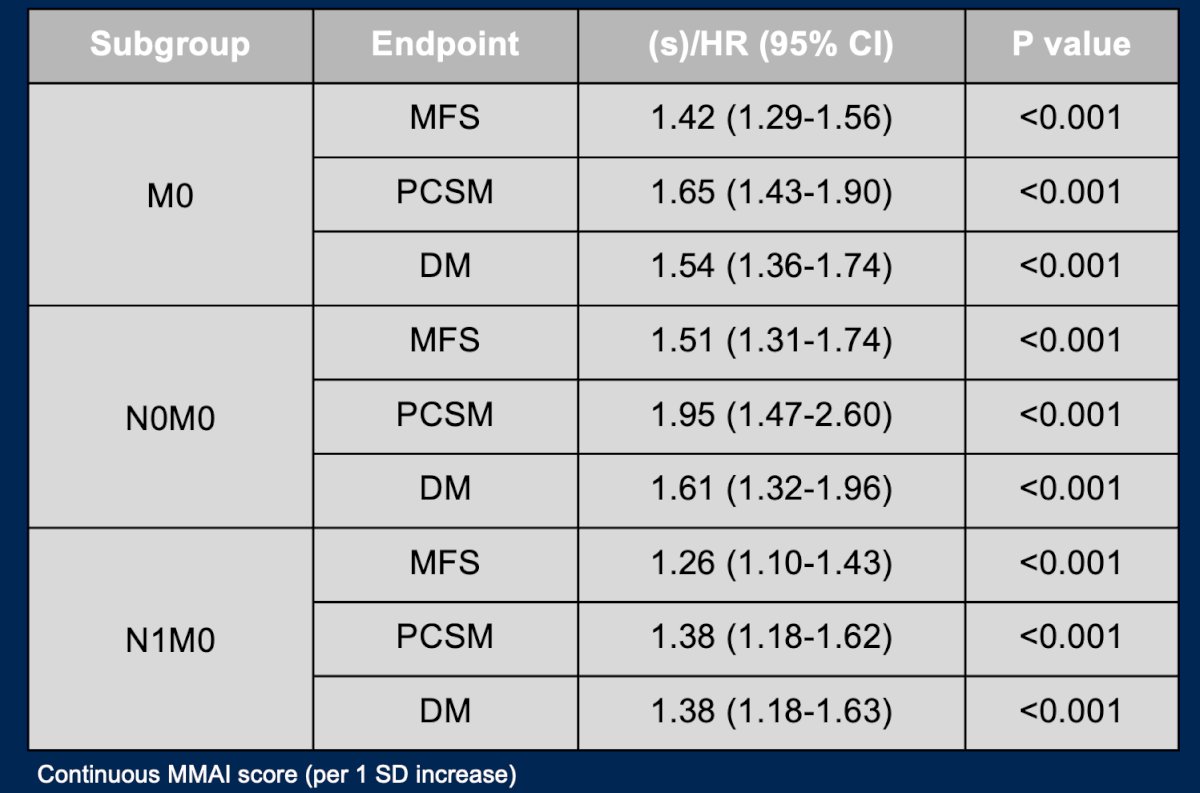
Moreover, an alternative MMAI cut-point was identified through an exploratory grid search using prognostic risk scores, aiming to optimize treatment benefit from abiraterone. This analysis stratified patients into two groups: the upper quartile versus the lower three quartiles of the MMAI score distribution. This data-driven threshold demonstrated significant discrimination in metastasis-free survival, with patients in the upper quartile showing a greater benefit from the addition of abiraterone:
M0 patients with MMAI scores in the upper quartile of risk were significantly more likely to benefit from the addition of abiraterone, with a hazard ratio for metastasis-free survival of 0.48 (95% CI 0.33–0.71). Notably, the interaction between MMAI risk score and treatment effect was statistically significant (interaction p = 0.01), supporting the potential role of MMAI as a predictive biomarker to guide selective treatment intensification with abiraterone in high-risk prostate cancer: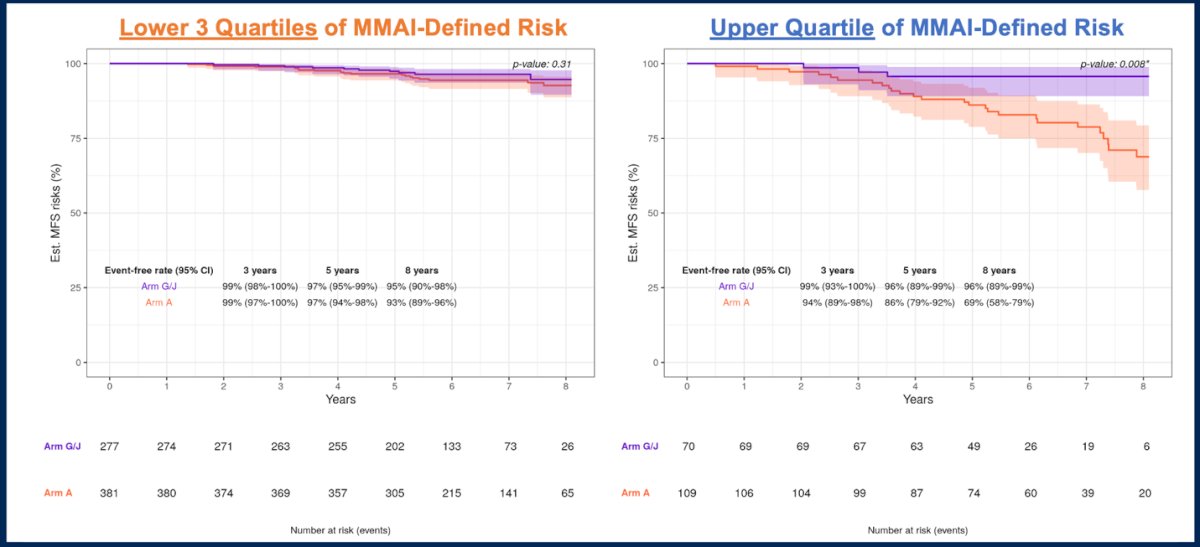
In terms of metastasis-free survival, distant metastasis, and prostate cancer-specific mortality, patients in the upper quartile of MMAI-defined risk derived the greatest benefit from the addition of abiraterone. The treatment by MMAI interaction p-value was significant for both metastasis-free survival and prostate cancer-specific mortality, indicating a meaningful predictive effect. Notably, the absolute risk reduction in metastasis-free survival with abiraterone was 17% in the upper quartile compared to 2% in the lower three quartiles, highlighting the potential of MMAI scores to guide more personalized treatment intensification: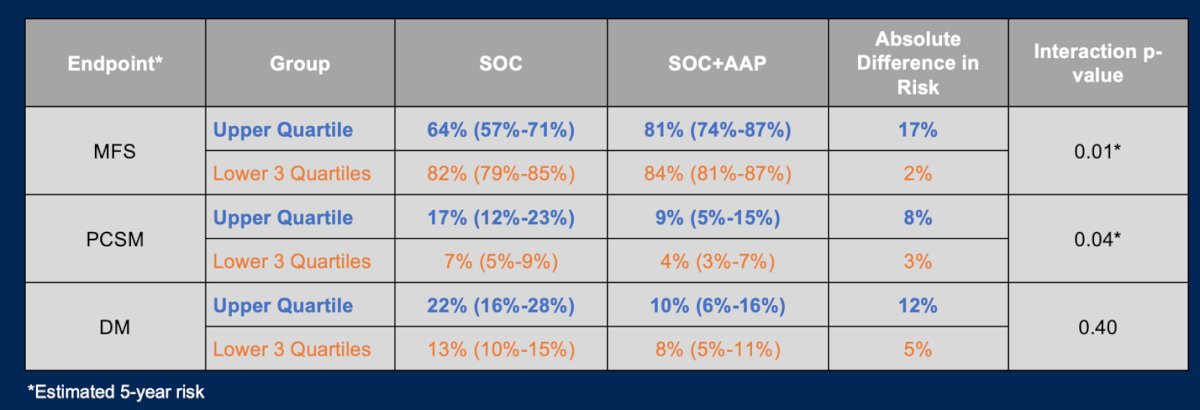
Dr. Chavarriaga also briefly mentioned utilization of the Decipher 22-gene genomic classifier assay, which has been tested in multiple studies, resulting in a specific table in the NCCN guidelines highlighting its use in NCCN intermediate risk, NCCN high risk, and post-radical prostatectomy biochemical recurrence patients: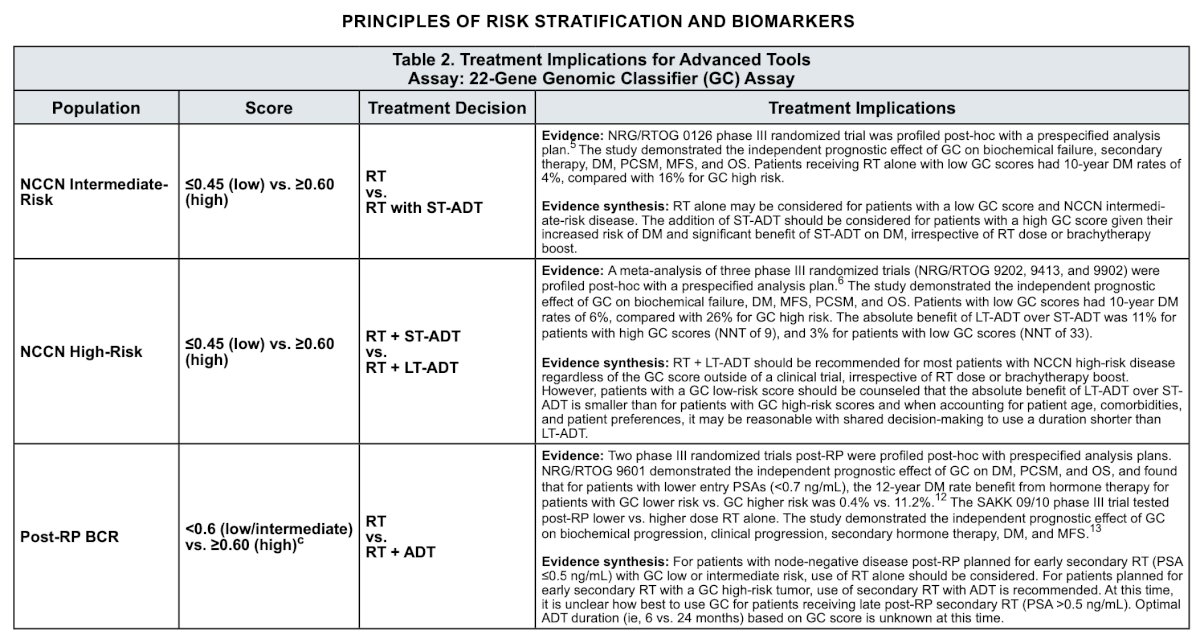
Next, Dr. Chavarriaga discussed the use of molecular imaging as a potential biomarker. At the 2025 ASCO annual meeting, Dr. Wolfgang Fendler presented results of a validated three-tier risk stratification model, PSMA-PET PROMISE version 2 (PPP2), in a large international multi-center registry study assessing prostate cancer-specific survival. In the development cohort, predictors for PPP2 were assessed, and visual and quantitative nomograms were generated using Cox regression models with least absolute shrinkage and selection operator penalty for overall survival: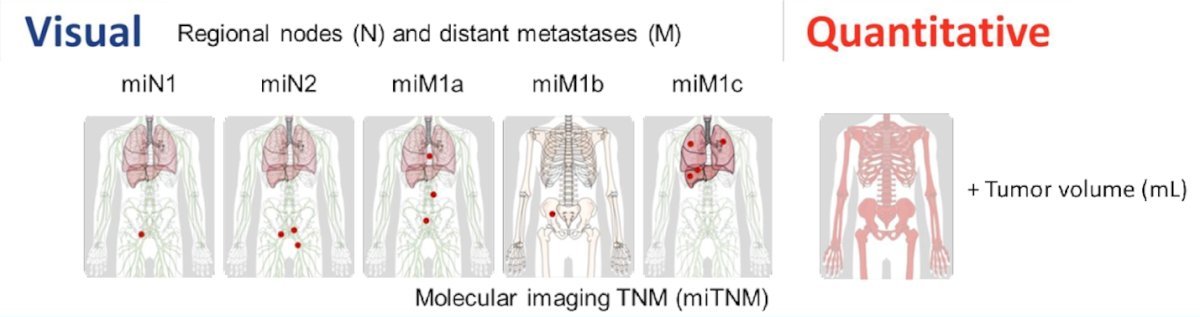
When stratified into three risk groups (low, intermediate, high), both PPP2 nomograms outperformed the NCCN risk classification (n = 1,034) with an AUC of 0.84 versus 0.76 (p <0.0001). Similarly, both PPP2 nomograms outperformed the EAU biochemical recurrence risk classification (p-value for the visual PPP2 nomogram 0.016 and the quantitative PPP2 nomogram 0.00050) as illustrated in the following table: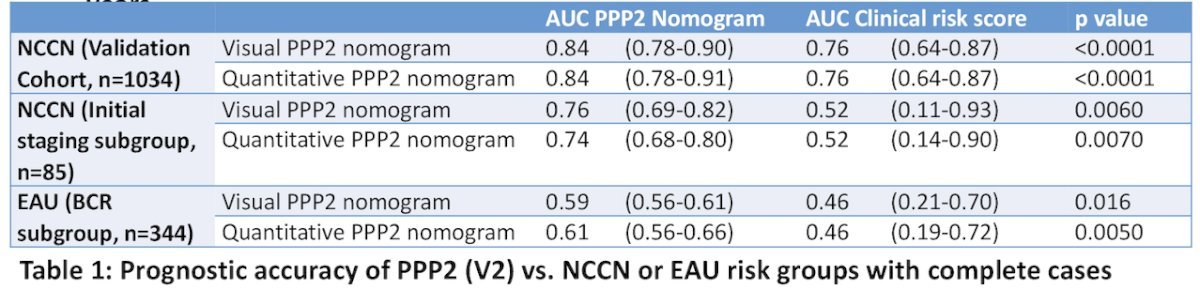
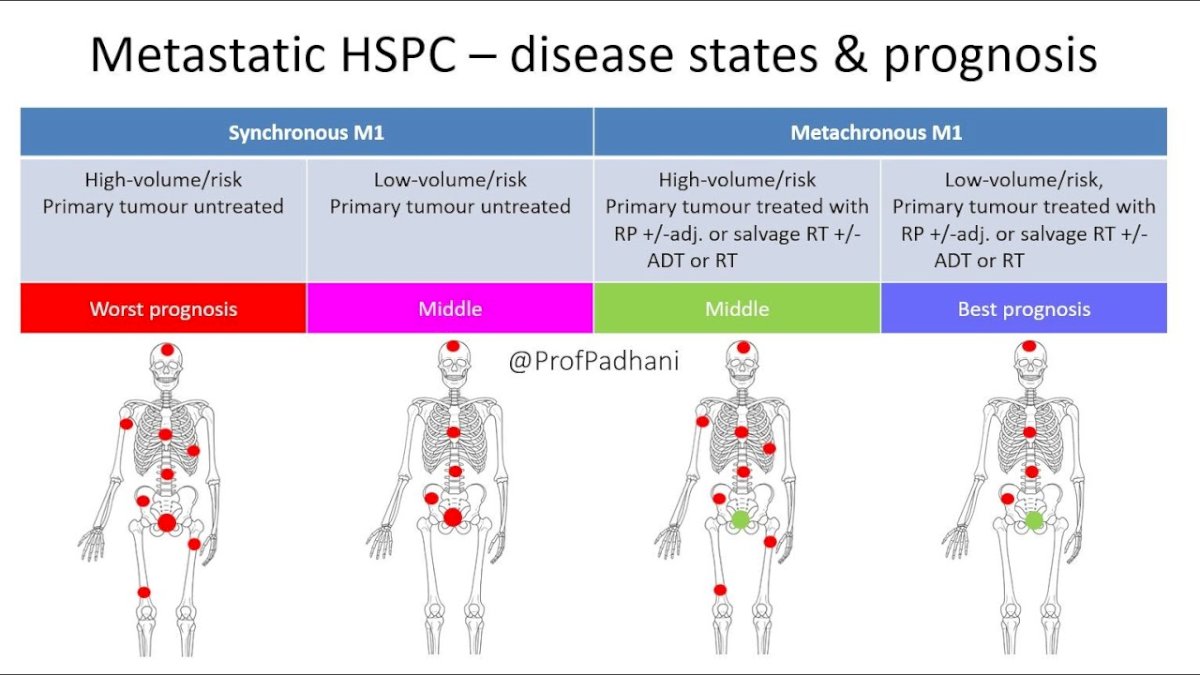
Dr. Chavarriaga then discussed biomarkers in the mHSPC setting, for which there is heterogeneity in outcomes depending on disease presentation and volume/risk of disease:
Currently, a typical paradigm for treatment of mHSPC may look as follows:
- Synchronous low volume: ADT + androgen receptor pathway inhibitor + local treatment
- Metachronous low volume: ADT + androgen receptor pathway inhibitor
- High volume: ADT + androgen receptor pathway inhibitor +/- docetaxel
How low should our goal be for PSA response after initiating therapy for mHSPC patients? At ASCO 2025, Dr. Michael Ong presented data from the IRONMAN Registry assessing the prognostic significance of a PSA > 0.2 ng/mL after 6-12 months of treatment intensification with an androgen receptor pathway inhibitor. The IRONMAN Registry is a prospective, international cohort that includes over 4,600 patients with mHSPC and castration-resistant prostate cancer (CRPC). The registry spans 123 active sites across 15 countries and captures comprehensive, real-world data, including patient demographics, blood samples, clinical outcomes, and patient- and physician-reported questionnaires. The initial analysis used a PSA threshold of <0.2 ng/mL; however, based on feedback and the availability of ultrasensitive PSA testing at select centers, the analysis was revised to also examine a lower cutoff of <0.02 ng/mL. Recognizing the variability in access to ultrasensitive assays across sites, the investigators conducted a revised analysis using an intermediate threshold of PSA <0.1 ng/mL to enhance generalizability:
This analysis included patients with mHSPC who were treated with ADT plus an androgen receptor pathway inhibitor, with or without docetaxel, and had available PSA data for at least 12 months. Patients were stratified into three PSA groups at both 6 and 12 months after ADT initiation: <0.1 ng/mL, 0.10–0.19 ng/mL, and ≥0.2 ng/mL. A total of 4,586 patients were in the IRONMAN registry, and 1,219 were included in the analysis. Geographically, the majority were from North America (56%), comprising 40% from the United States and 16% from Canada, followed by Europe (41%). Less than 1% of patients were enrolled from South America, Central America, and Africa: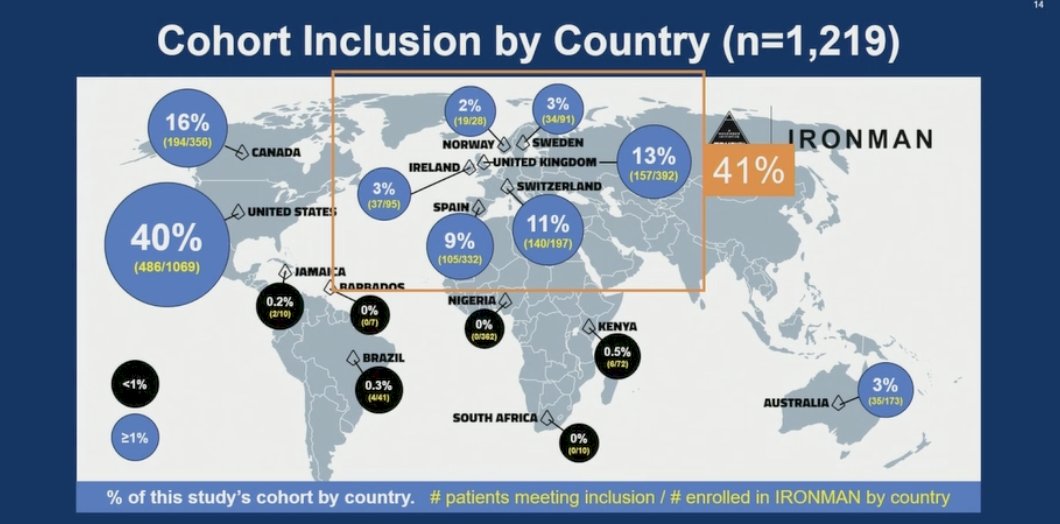
At 6 months, 52% of patients had a PSA <0.2 ng/mL, while 48% had a PSA ≥0.2. By 12 months, 68% of the overall cohort had achieved PSA <0.2 ng/mL, indicating that a notable proportion of patients with suboptimal early PSA responses improved by the 12-month landmark. Specifically, some patients initially in the ≥0.2 ng/mL group showed continued decline (only 32% had a PSA ≥ 0.2 ng/mL at 12 months), highlighting the dynamic nature of PSA responses and the potential utility of 12-month PSA in refining prognostication: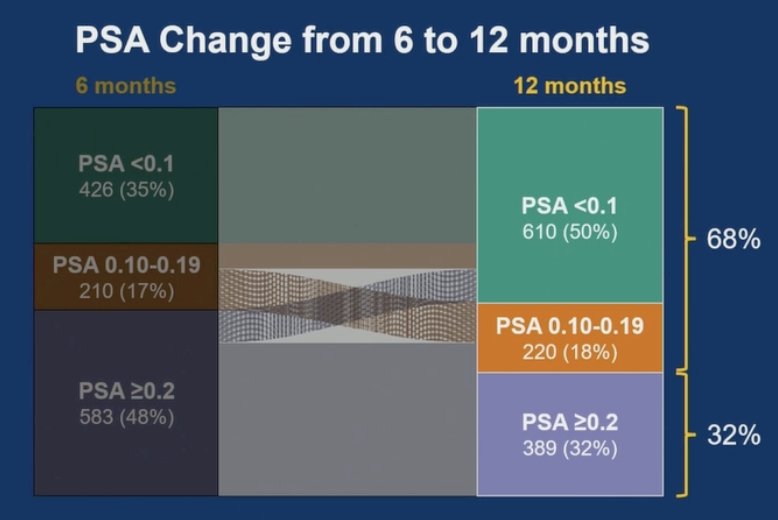
In a 12-month landmark analysis, PSA levels at 12 months were strongly associated with both overall survival and progression-free survival in patients with mHSPC treated with ADT + androgen receptor pathway inhibitor. Patients with PSA <0.1 ng/mL at 12 months had the most favorable outcomes, with an 84% 3-year overall survival rate and 80% 3-year progression-free survival. Those with PSA 0.10–0.19 ng/mL had slightly worse outcomes (79% overall survival and 62% progression-free survival at 3 years), while patients with PSA ≥0.2 ng/mL had markedly poorer prognoses, with a 3-year overall survival of 45% and progression-free survival of 41%. Median survival was 29 months, and median progression free survival was 23 months:
The data further support that PSA at 12 months is prognostic regardless of androgen receptor pathway inhibitor class, or whether patients received doublet or triplet therapy. Across treatment intensities and androgen receptor pathway inhibitor types, patients with lower PSA levels consistently experienced better survival and progression-free outcomes:
Additionally, multivariable Cox regression analysis demonstrated that 12-month PSA is a strong independent prognostic factor. Specifically, patients with PSA ≥0.2 ng/mL at 12 months had nearly a fivefold increased risk of death compared to those with PSA <0.1 ng/mL (HR 4.85; 95% CI 3.36–7.01):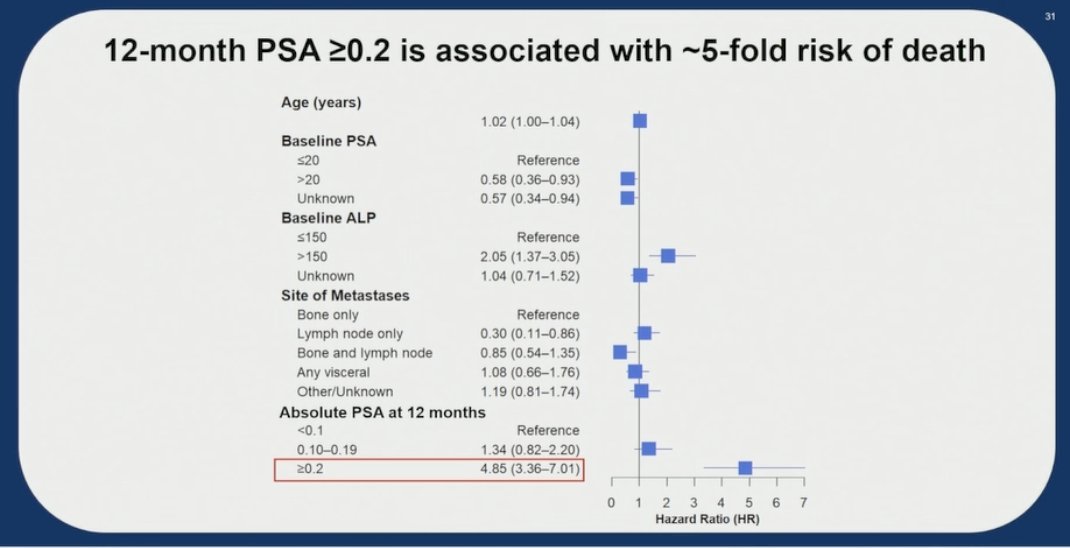
Based on these findings, two important trials are currently enrolling. The first is TRIPLE-SWITCH, which was launched to assess escalation for patients with mHSPC and PSA ≥0.2 ng/mL after 6–12 months of ADT + androgen receptor pathway inhibitor. Patients are randomized 1:1 to continue standard of care or receive docetaxel added to ADT + androgen receptor pathway inhibitor. The primary objective is overall survival, with secondary endpoints including PSA responses, progression-free survival, and ctDNA correlatives: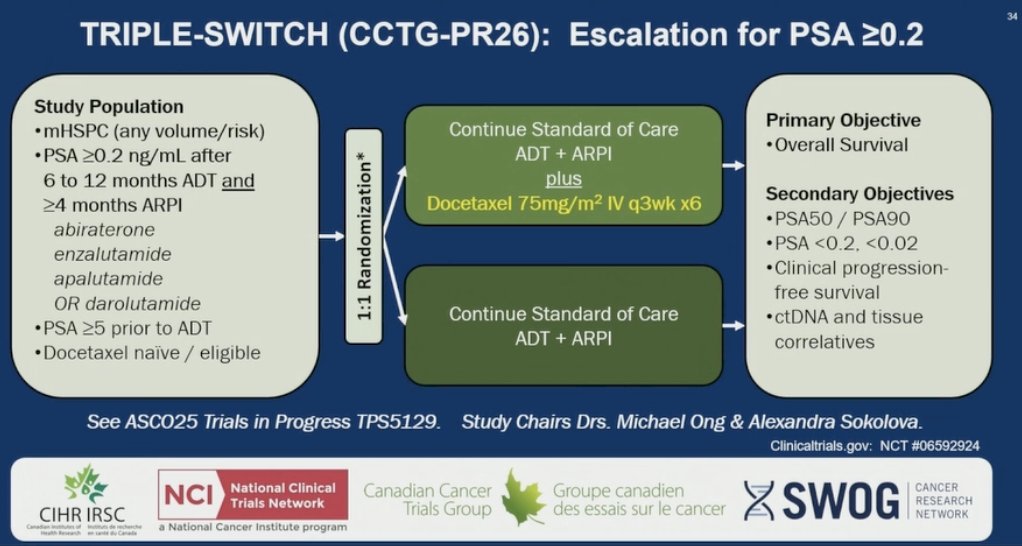
The second trial is DE-ESCALATE (EORTC 2238), a pragmatic, phase 3 randomized study evaluating intermittent ADT in patients with mHSPC who have achieved a PSA ≤0.2 ng/mL after 6–12 months of ADT + androgen receptor pathway inhibitor. Patients are randomized 2:1 to intermittent versus continuous androgen receptor pathway inhibitor-based therapy, stratified by country, treatment regimen, and PSA levels (≤0.1 vs >0.1–≤0.2 ng/mL). Treatment is paused at 6 months if PSA remains suppressed, with re-initiation at the investigator’s discretion upon PSA progression: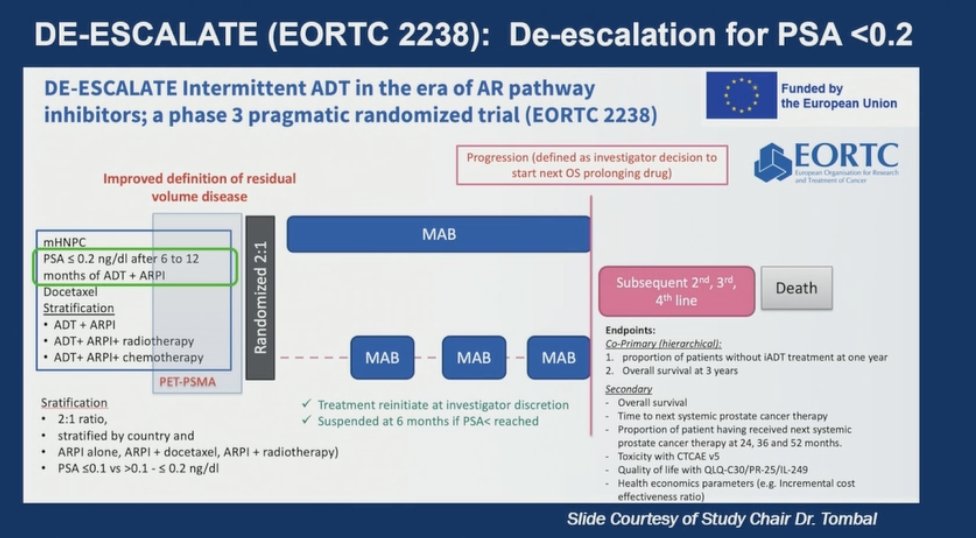
Does time to ultra-low PSA matter? At the 2024 ASCO annual meeting, Dr. Ben Maughan presented data from the OASIS Project assessing rapid and deep PSA responses to apalutamide + ADT in men with mHSPC. This analysis included 183 patients with mHSPC who initiated apalutamide + ADT treatment and had monthly PSA testing. The mean age was 73 years, median baseline PSA 4.8 ng/mL (IQR 0.8, 20.7), and the mean duration of follow-up was 18 months: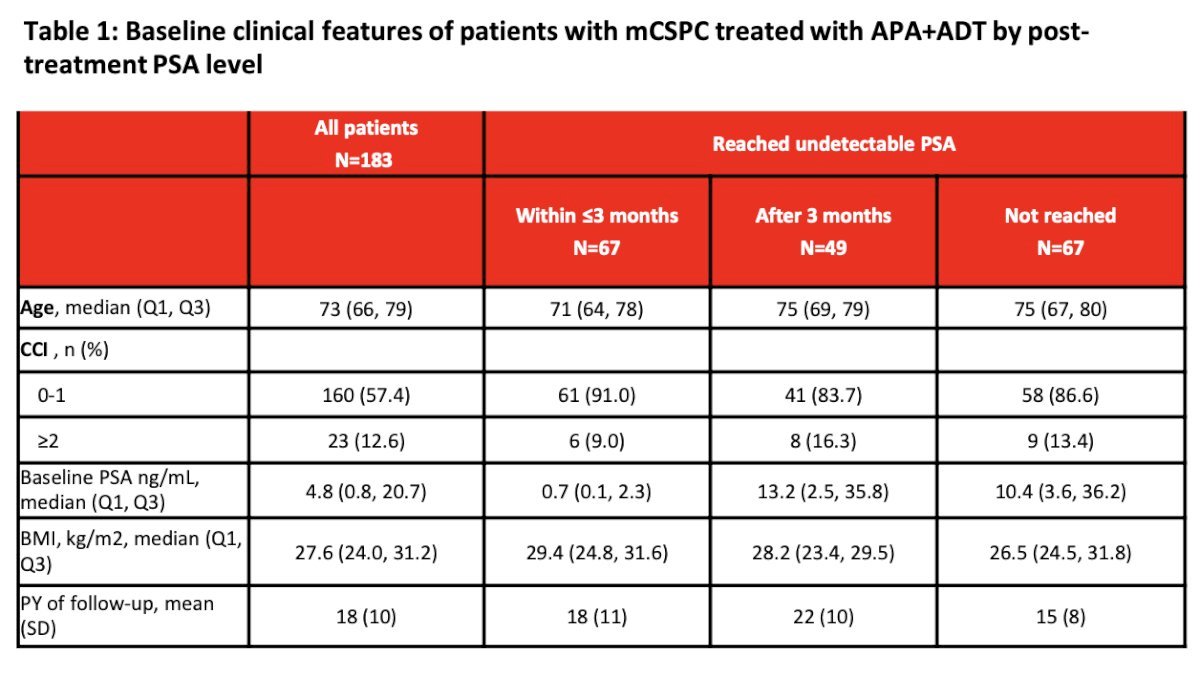
The majority of patients (68%) experienced a PSA reduction of at least 50% within 3 months after initiating treatment, with 37% reaching an undetectable PSA level (≤0.2 ng/mL). The median time to achieving an undetectable PSA was 2.1 (IQR 1.1, 3.0) months in the group with responses within 3 months and 4.7 (IQR 3.0, 24.6) months in the group with responses after 3 months. Of note, survival rates increase not only when PSA responses occur more rapidly (within ≤3 months) but also when they achieve deep PSA reductions (undetectable versus PSA50):
The Kaplan-Meier curves below depict overall survival stratified by time to undetectable PSA and time to PSA50 response, categorized as ≤3 months or >3 months. The adjusted HR for overall survival when an undetectable PSA was achieved within ≤3 Months were 0.15 (95% CI 0.05-0.47). Similarly, the adjusted HR for overall survival was 0.27 (95% CI 0.12-0.65) when the undetectable PSA response was achieved after >3 months: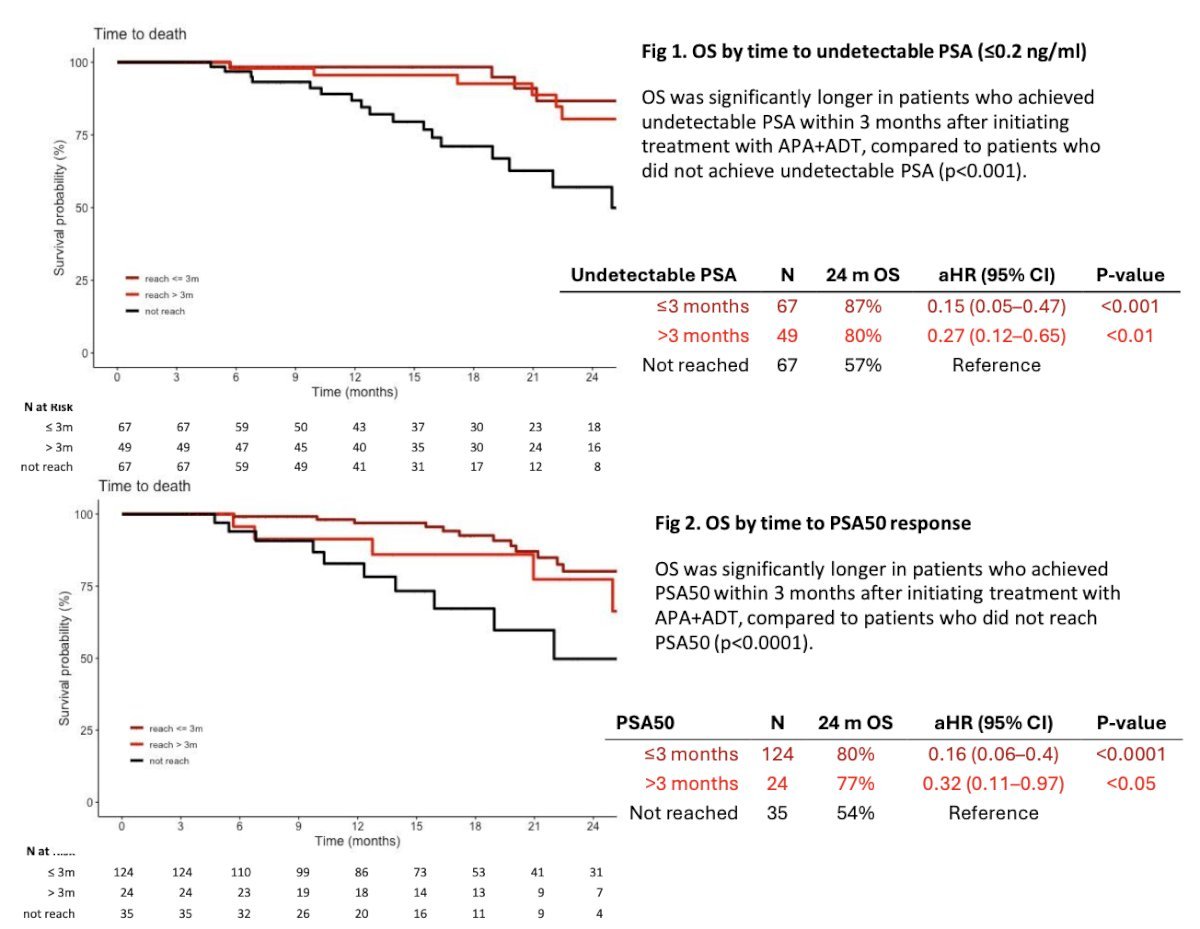
With regards to genetic markers, specifically tumor suppressor genes, Dr. Chavarriaga discussed a study from Gebrael et al.2 which assessed the association of baseline tumor genomic markers on survival in patients with mHSPC treated with ADT intensification. This study included 276 patients, and on multivariable analysis, TP53 (HR 1.71, 95% CI 1.17-2.49), RB1 (HR 2.32, 95% CI 1.28-4.18), PTEN (HR 1.74, 95% CI 1.12-2.7), and BRCA2 (HR 2.64, 95% CI 1.42-4.92) were associated with significantly shorter progression free survival, while TP53 (HR 1.63, 95% CI 1.00-2.64), RB1 (HR 4.5, 95% CI 2.32-8.70), and PTEN (HR 2.4, 95% CI 1.38-4.2) were associated with significantly worse overall survival:
![With regards to genetic markers, specifically tumor suppressor genes, Dr. Chavarriaga discussed a study from Gebrael et al. [2], which assessed the association of baseline tumor genomic markers on survival in patients with mHSPC treated with ADT intensificiation. This study included 276 patients, and on multivariable analysis, TP53 (HR 1.71, 95% CI 1.17-2.49), RB1 (HR 2.32, 95% CI 1.28-4.18), PTEN (HR 1.74, 95% CI 1.12-2.7), and BRCA2 (HR 2.64, 95% CI 1.42-4.92) were associated with significantly shorter progression free survival, while TP53 (HR 1.63, 95% CI 1.00-2.64), RB1 (HR 4.5, 95% CI 2.32-8.70), and PTEN (HR 2.4, 95% CI 1.38-4.2) were associated with significantly worse overall survival:](/images/com-doc-importer/223-scu-2025/scu-2025-tumor-markers-in-prostate-cancer-2025-update/image-27.jpg)
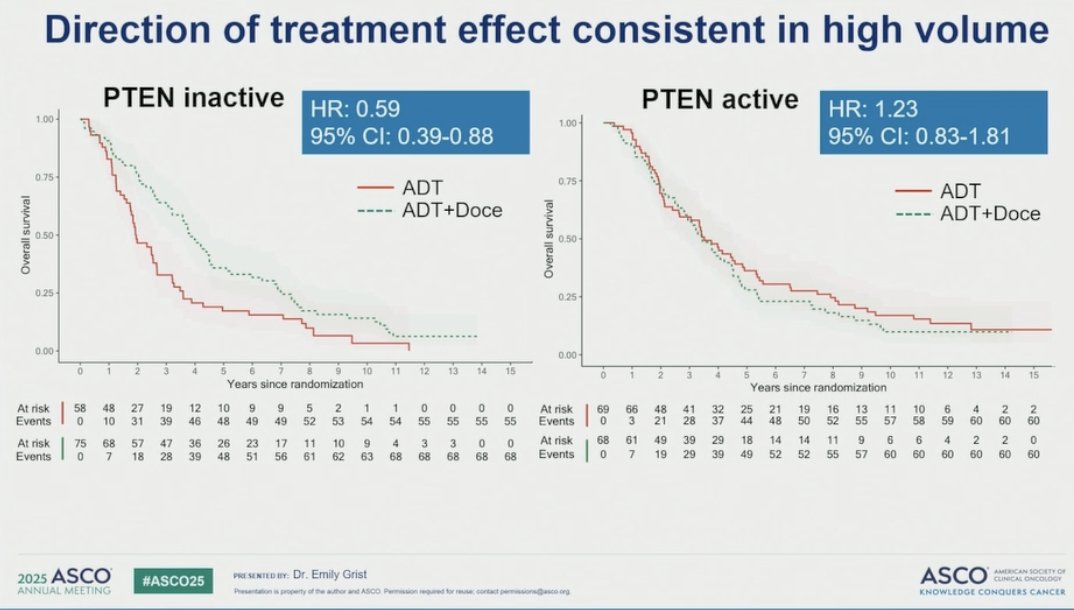
At ASCO 2025, Dr. Emily Grist presented an ancillary study of the STAMPEDE trials evaluating if transcriptome classification of PTEN inactivation predicts survival benefit from docetaxel at the start of ADT for metastatic prostate cancer. This study leveraged the multi-arm multi-stage STAMPEDE platform, which included 3,909 patients randomized to ADT, ADT + docetaxel, or ADT + abiraterone. The aim was to link tumor multi-gene expression signatures to 14-year prospective overall survival data, in order to identify biomarkers with prognostic and predictive value: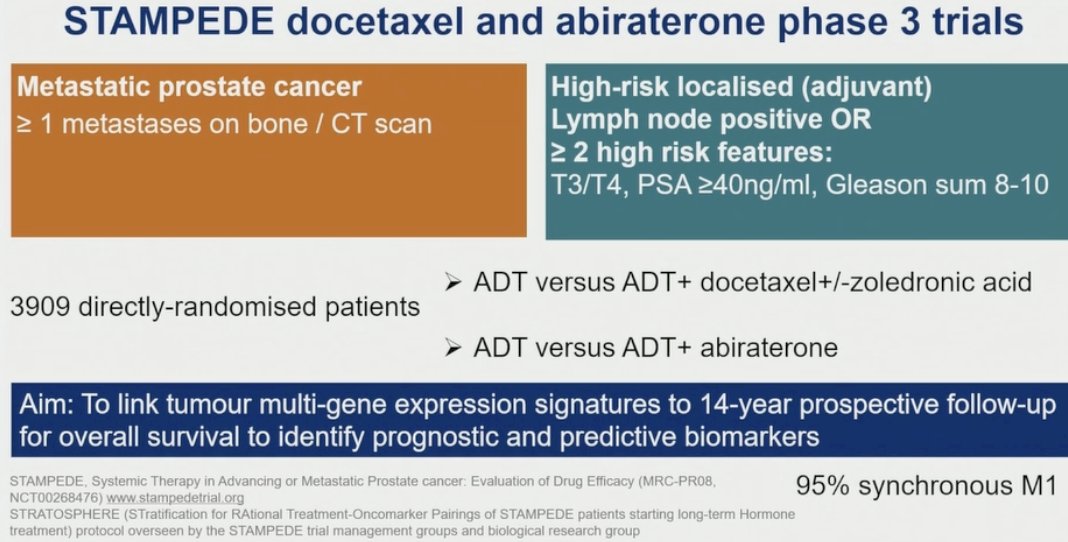
This study found that PTEN inactivity was associated with shorter overall survival in patients treated with ADT + abiraterone, suggesting resistance in this setting. In contrast, this association was not seen in the ADT + docetaxel group, where the hazard ratio was <1, indicating that PTEN-inactive tumors may remain sensitive to docetaxel-based therapy: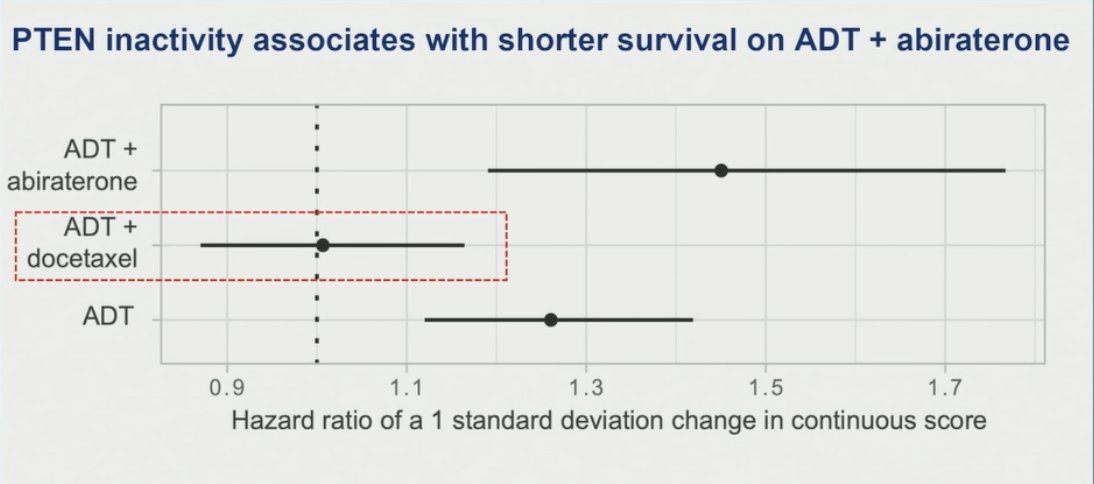
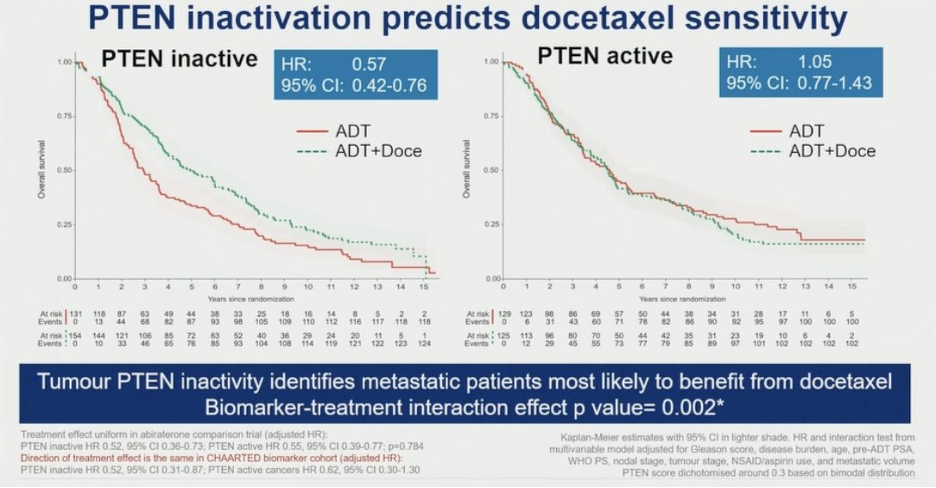
Among patients with PTEN-inactive tumors, the addition of docetaxel to ADT was associated with a 43% improvement in overall survival compared to ADT alone, indicating a clinically meaningful benefit. Conversely, in patients with PTEN-active tumors, there was no survival advantage with docetaxel (HR 1.05; 95% CI 0.77–1.43). These findings provide strong evidence that PTEN transcriptomic inactivity may serve as a predictive biomarker for identifying metastatic prostate cancer patients most likely to benefit from treatment intensification with docetaxel (biomarker-treatment interaction p = 0.002)
In a subsequent exploratory analysis, tumors were stratified into four groups based on Decipher and PTEN status. The subgroup with high Decipher scores and PTEN inactivity emerged as the most docetaxel-sensitive, despite the lack of overlapping genes between the two classifiers. Within this group, the addition of docetaxel to ADT significantly reduced the hazard of death by 45%, suggesting that this biomarker combination may help identify patients most likely to benefit from treatment intensification: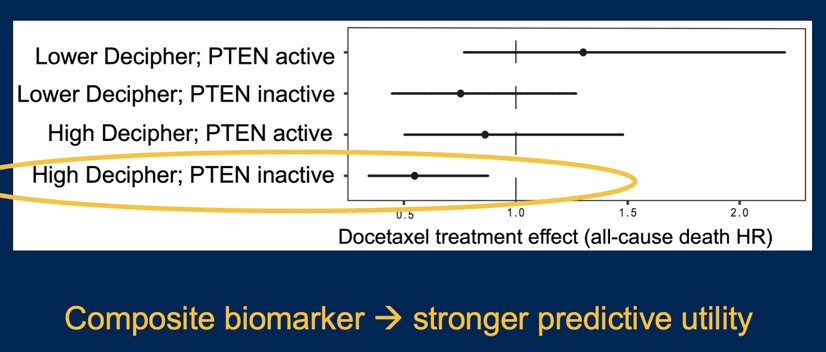
Notably, the direction of treatment effect favoring docetaxel in PTEN-inactive tumors was consistent across both low-volume and high-volume disease subgroups. Regardless of disease burden, PTEN transcriptomic inactivation was consistently predictive of survival benefit with the addition of docetaxel: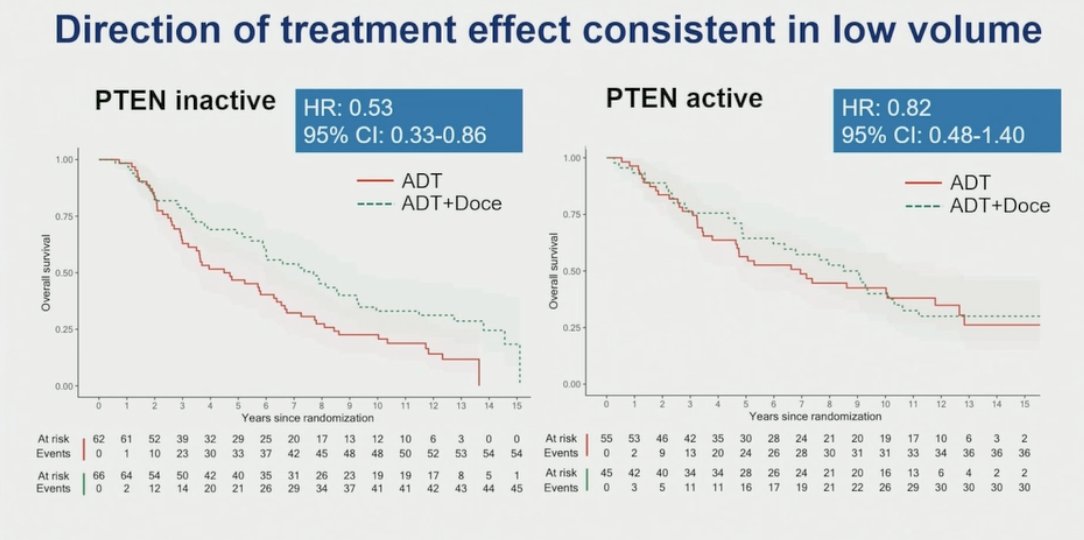
With regards to HRR mutations as a biomarker, Dr. Chavarriaga discussed the AMPLITUDE trial (presented at ASCO 2025), which was a randomized, double-blind, placebo-controlled phase 3 study evaluating the efficacy of fixed daily niraparib (200 mg) in combination with abiraterone acetate + prednisone (1000 mg + 5 mg) and continuous ADT in patients with mHSPC harboring at least one HRR mutation in one of the following genes: BRCA1, BRCA2, BRIP1, CDK12, CHEK2, FANCA, PALB2, RAD51B, RAD54L. A total of 696 patients with ECOG performance status 0–2 were randomized 1:1 to receive either niraparib + abiraterone acetate + prednisone + ADT or placebo + abiraterone acetate + prednisone + ADT. The primary endpoint was radiographic progression-free survival by investigator assessment, with key secondary endpoints including time to symptomatic progression, overall survival, and safety: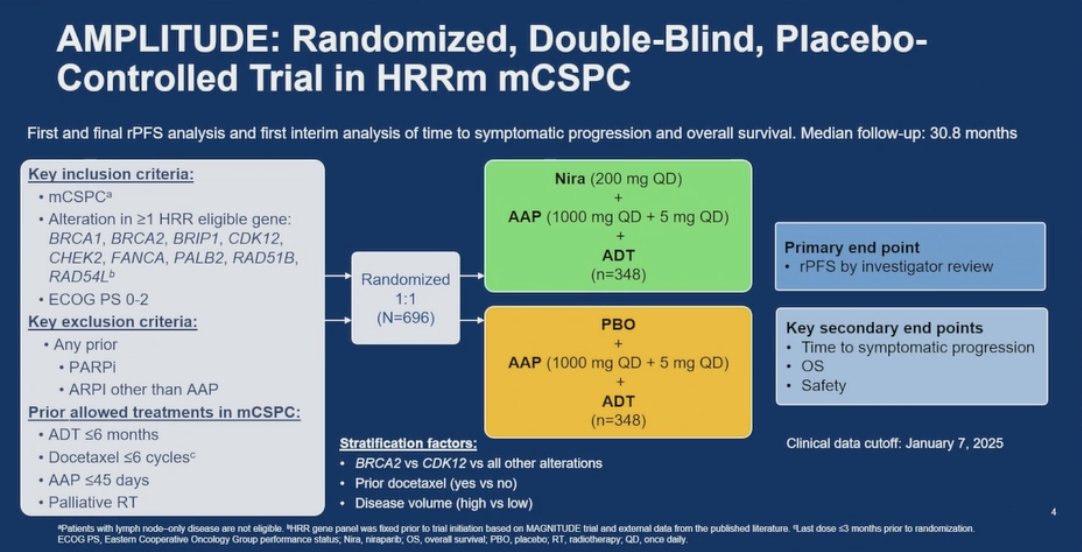
Baseline characteristics in AMPLITUDE were well balanced between treatment arms, as well the characteristics of patients in the BRCA mutation subgroup being consistent with those observed in the overall HRR mutation population: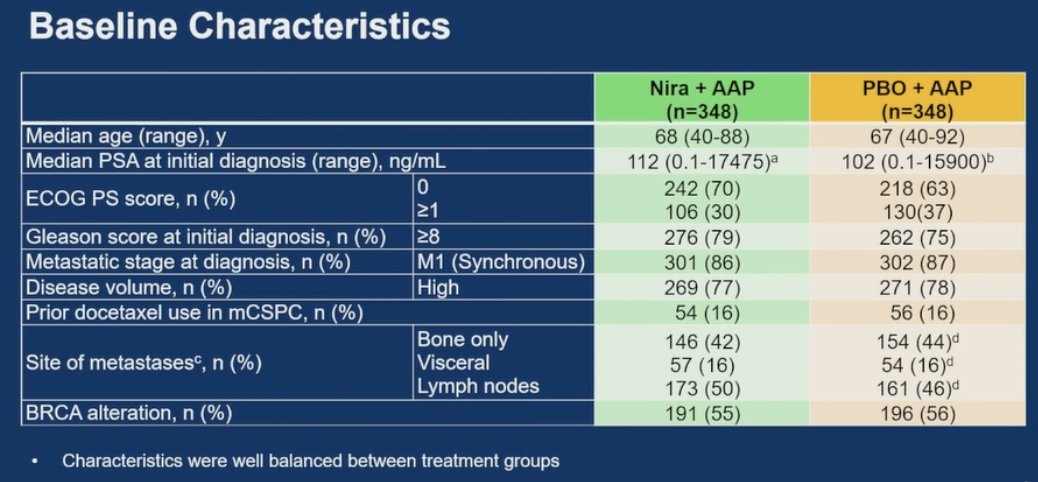
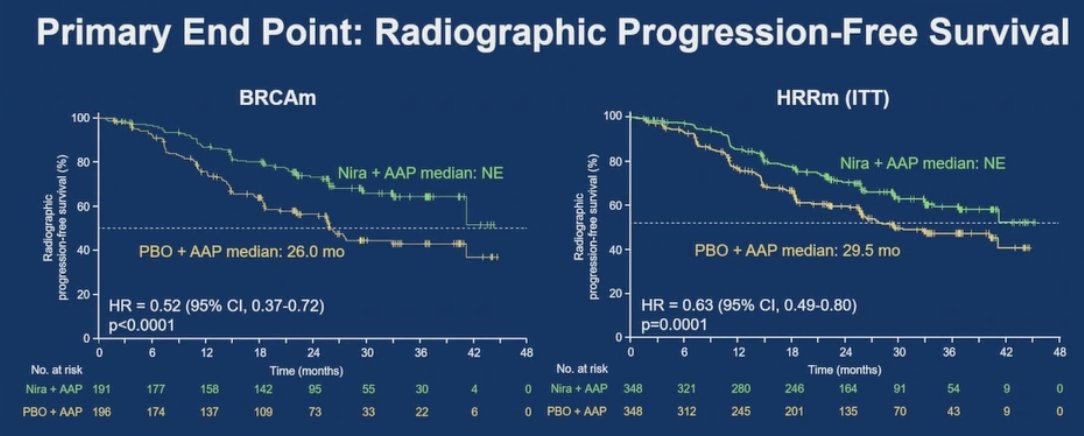
AMPLITUDE met its primary endpoint, demonstrating that the combination of niraparib and abiraterone acetate + prednisone significantly reduced the risk of radiographic progression or death by 48% in the BRCA mutation group (HR 0.52; 95% CI, 0.37–0.72) and by 37% in the broader HRR mutation population (HR 0.63; 95% CI, 0.49–0.80):
In the prespecified subgroup analysis, the radiographic progression free survival benefit from niraparib + abiraterone acetate + prednisone was consistent across all subgroups:
Finally, Dr. Chavarriaga discussed artificial intelligence as a biomarker in the mHSPC disease space. Presented at ASCO 2024, Dr. Mark Markowski presented the prognostic validation of the ArteraAI Prostate test in patients with mHSPC from the CHAARTED trial. In this study, the baseline characteristics stratified by those with and without available digital pathology was as follows:
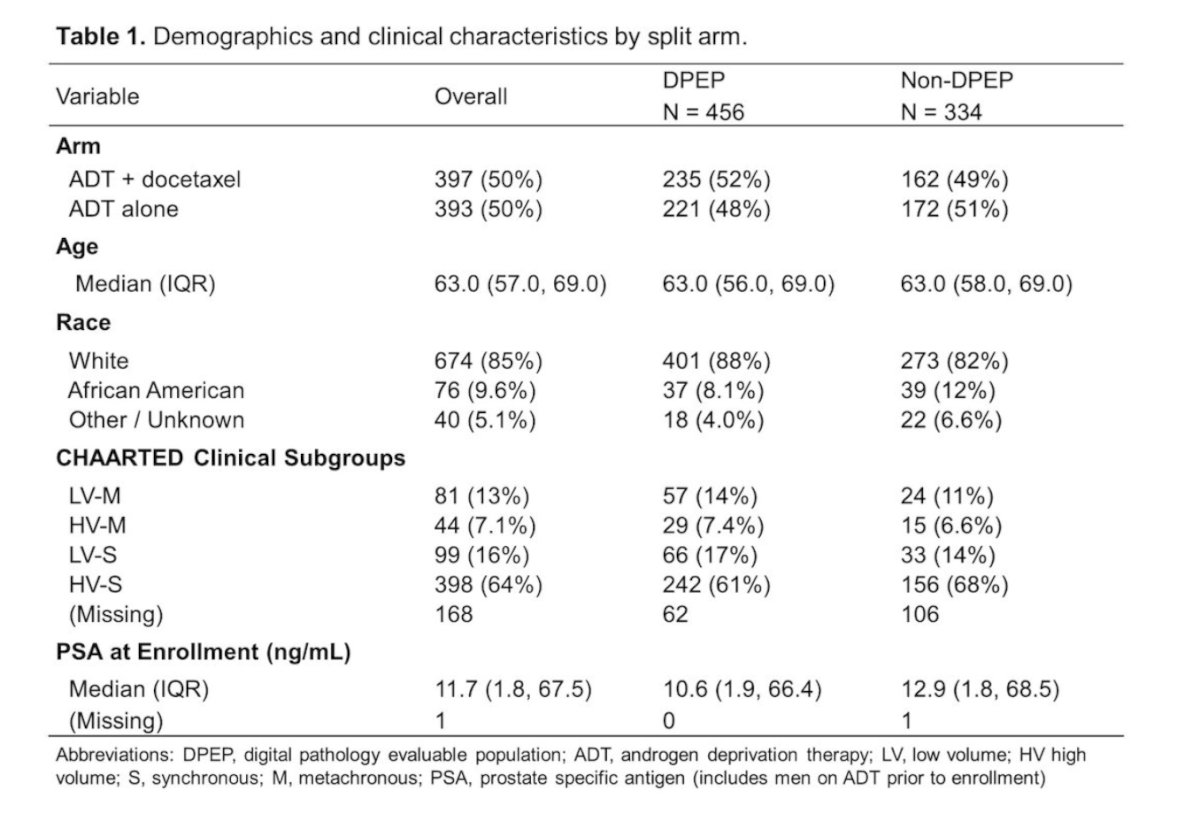
Of the included patients, 370 (81.1%) were classified as MMAI-high and 86 (18.9%) as MMAI-intermediate/low risk. Data were available from 394/456 patients for classification into the following four subgroups:
- LV-M (N=57) MMAI-high 56.1%
- HV-M (N=29) MMAI-high 69%
- LV-S (N=66) MMAI-high 86.4%
- HV-S (N=242) MMAI-high 92.6%
The median follow-up of the censored patients was 4.1 (IQR 3.3-5.0) years and the estimated 5-year overall survival across MMAI high, intermediate, and low groups was 39%, 58%, and 83%, respectively (log-rank p < 0.001). MMAI score was prognostic for overall survival (HR 1.5, 95% Cl 1.33-1.73 per standard deviation increase) on univariable analysis:
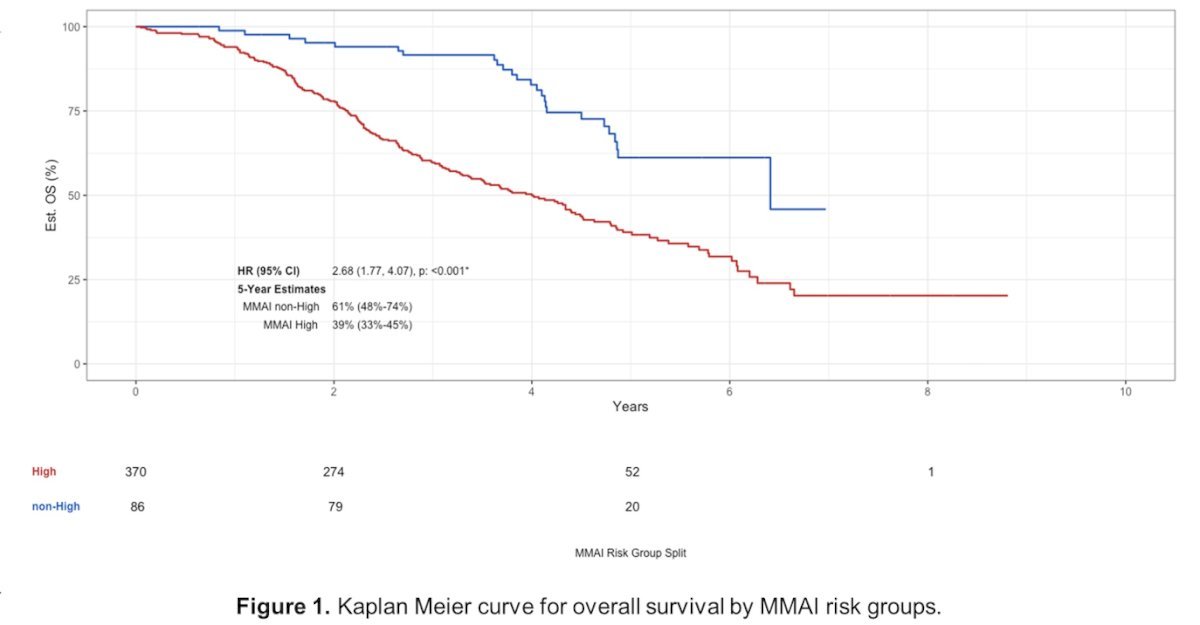
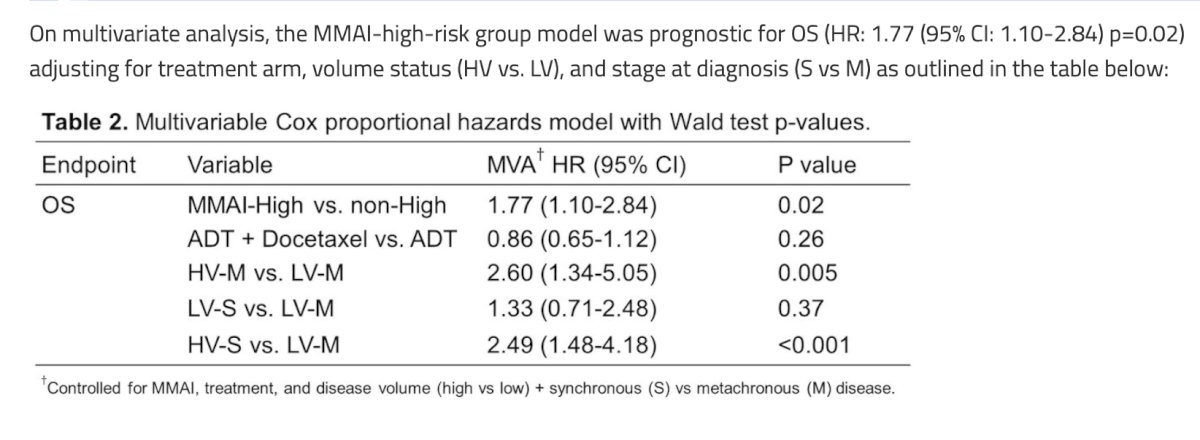
On multivariate analysis, the MMAI-high-risk group model was prognostic for overall survival (HR 1.77, 95% CI 1.10-2.84) adjusting for treatment arm, volume status (high volume versus low volume), and stage at diagnosis (synchronous versus metachronous):
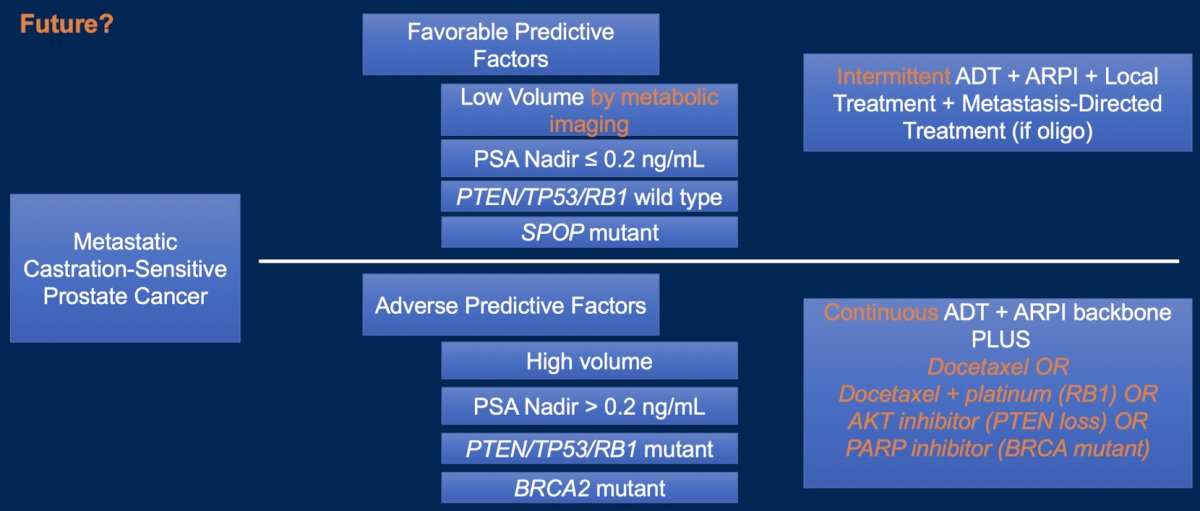
Dr. Chavarriaga highlighted the following potential future tailored approach to treatment of mHSPC:
Dr. Chavarriaga concluded his presentation discussing an update of tumor markers in prostate cancer with the following take home points, emphasizing that not all prostate cancer patients are the same:
- In localized and locally advanced prostate cancer, biomarkers include:
- Multiparametric MRI
- MMAI models
- Decipher genomic classifier
- Identification of intraductal carcinoma and/or cribriform morphology
- In mHSPC, biomarkers include:
- PTEN mutations - favor treatment with docetaxel
- HRR mutations (ie. BRCA2) – favor PARP inhibitors + androgen receptor pathway inhibitors
- If a patient achieves an ultra-low PSA, can we de-intensify treatment?
- MMAI models may guide treatment intensification: doublet versus triplet
- We are entering a new era of diagnostic-therapeutic integration: surgery, targeted therapy, biomarkers, and radiopharmaceuticals to improve outcomes in prostate cancer
Presented by: Julian Chavarriaga, MD, Urologo Oncologo Fundacion CTIC – Clinica del Country, Bogota, Colombia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Sociedad Colombiana de Urologia (SCU) Annual Meeting, Cartagena, Colombia, Wed, Aug 20 – Sat, Aug 23, 2025.
References:
- Rajwa P, Mori K, Huebner NA, et al. The prognostic association of prostate MRI PI-RADS v2 assessment category and risk of biochemical recurrence after definitive local therapy for prostate cancer: A systematic review and meta-analysis. J Urol. 2021 Sep;206(3):507-516.
- Gebrael G, Sayegh N, Chehade CH, et al. Genomic biomarkers of survival in patients with metastatic hormone-sensitive prostate cancer undergoing intensified androgen deprivation therapy. Prostate Cancer Prostatic Dis. 2025 Jan 31 [Epub ahead of print].