(UroToday.com) The 2026 SNMMI annual meeting featured a genitourinary radiotherapeutics session and a presentation by Dr. Kambiz Rahbar discussing safety and survival outcomes of radium-223 in patients with metastatic castration-resistant prostate cancer (mCRPC) with prior 177Lu-PSMA radioligand therapy in the LuRa study. 177Lu-PSMA is a beta emitter prolonging survival in patients with PSMA-positive mCRPC previously treated with at least one line of taxane-based chemotherapy and at least one line of androgen receptor pathway inhibitor (ARPI). Radium-223 is an alpha emitter which prolongs survival and improves quality of life in patients with bone predominant mCRPC. However, there is a lack of data on the feasibility of sequencing with Radium-223 after 177Lu-PSMA. This retrospective multicenter study (LuRa) aimed to evaluate the safety and effectiveness of radium-223 in mCRPC patients previously treated with 177Lu-PSMA.
The LuRa study was a multicenter retrospective trial conducted at 4 centers in Germany. Eligible patients had received at least one dose of 177Lu-PSMA followed by at least one dose of radium-223:
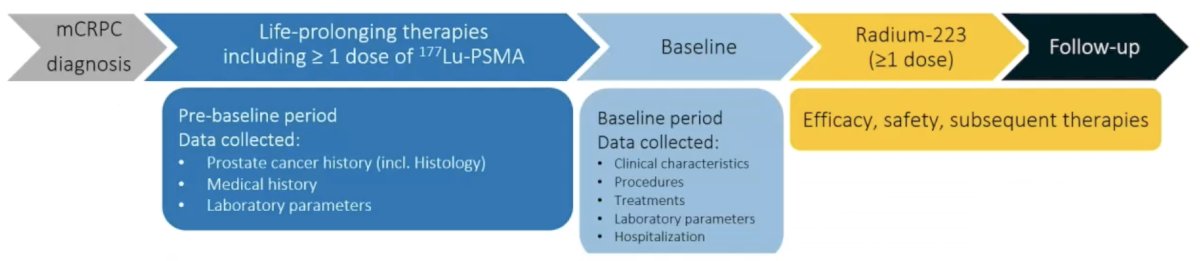
Primary endpoints included adverse event incidence, grade 3–4 hematologic toxicities, and laboratory abnormalities. Secondary endpoints were overall survival, time to next treatment or death, and changes in serum PSA.
Data from 67 patients were analyzed. Prior to radium-223 therapy, 28.4% had received at least five life-prolonging therapies, and all had received at least one cycle of 177Lu-PSMA. A median of 3 (range: 1 - 6) radium-223 injections was administered. The following table summarizes the patient characteristics:
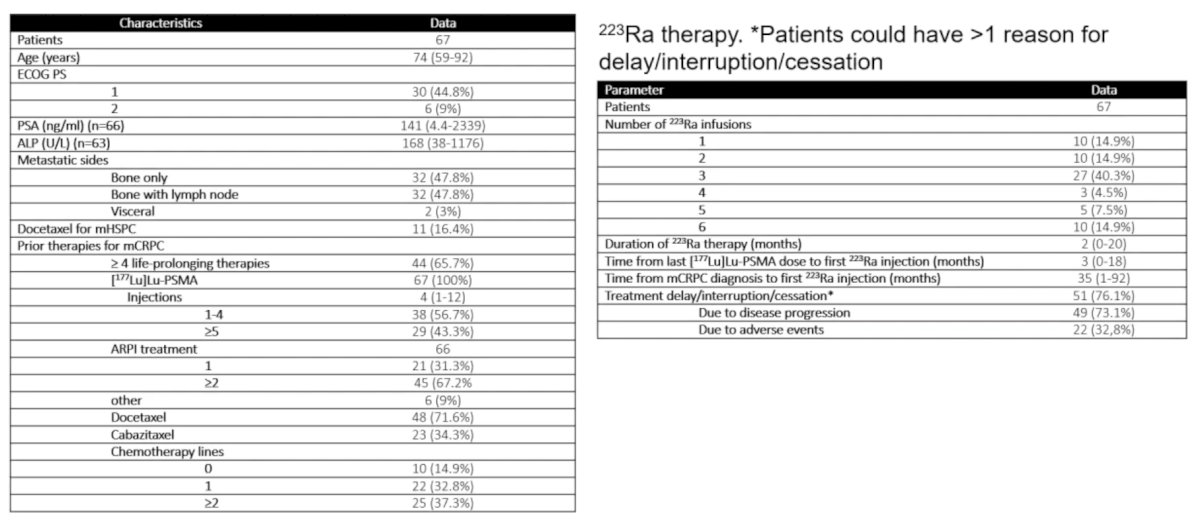
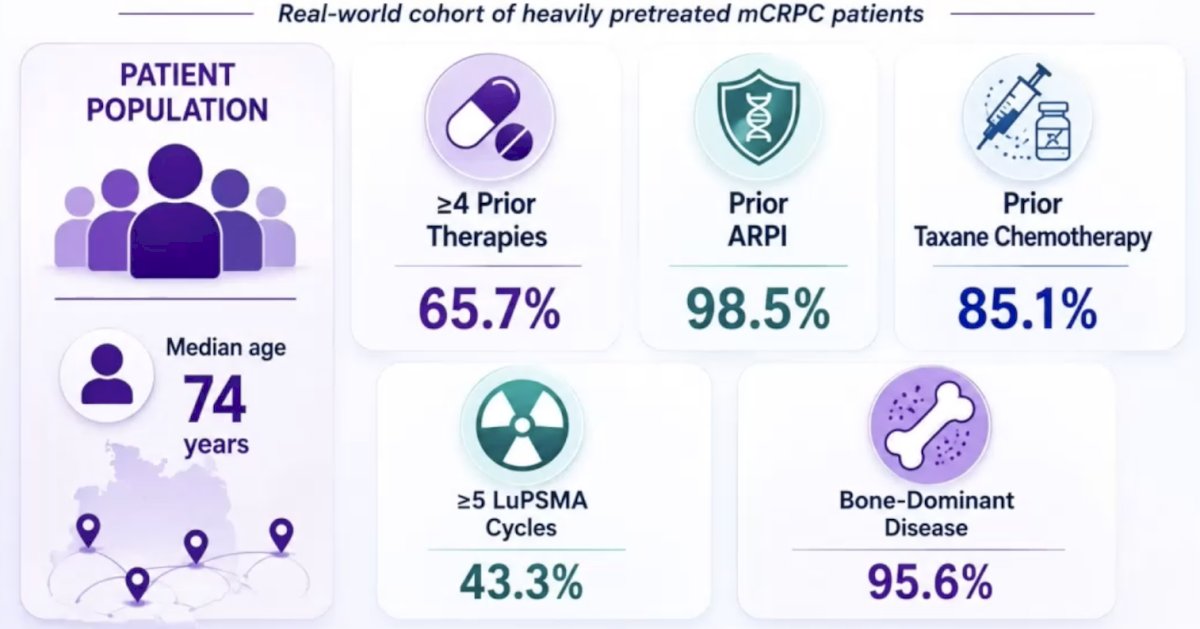
The median patient age was 74 years, 65.7% had >= 4 prior therapies, 98.5% had received a prior ARPI, and 85.1% had received prior taxane chemotherapy:
Any grade treatment emergent adverse events occurred in 74.6%, and grade 3-4 adverse events in 34.3%. The most frequent grade 3–4 observed toxicity was anemia (28.4%) and thrombocytopenia (10.5%):
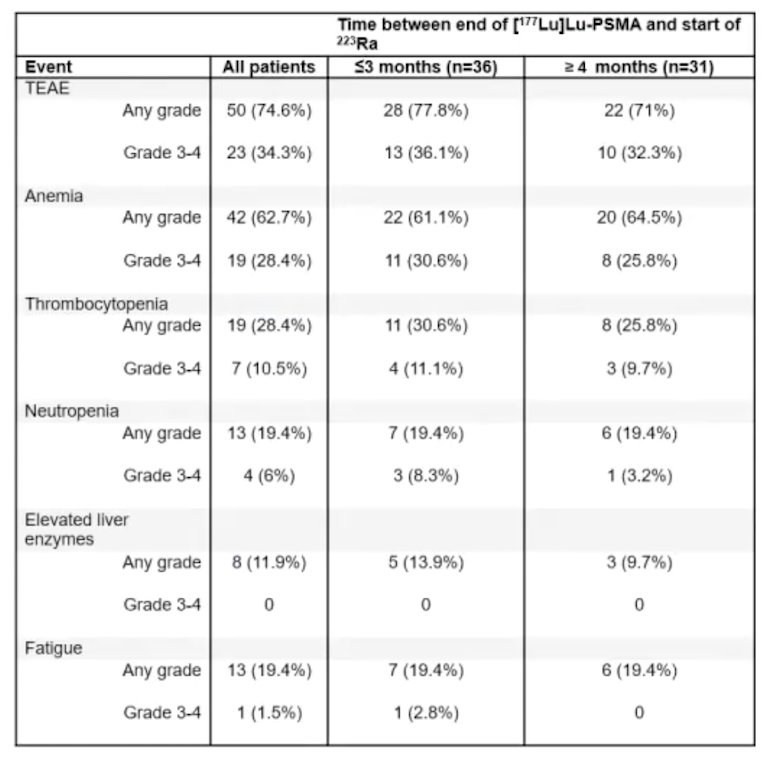
Safety and overall survival were similar regardless of time interval between 177Lu-PSMA and radium-223 or prior chemotherapy sequence: grade 3-4 treatment emergent adverse events <=3 months (36.1%) versus > 3 months (32.3%); grade 3-4 anemia <=3 months (30.6%) versus > 3 months (25.8%); grade 3-4 thrombocytopenia <=3 months (11.1%) versus > 3 months (9.7%):

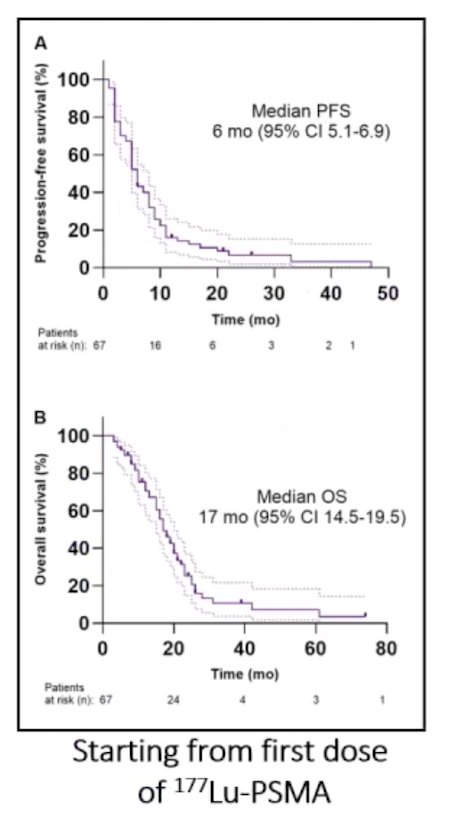
Starting from the first dose of 177Lu-PSMA radioligand therapy, the median progression-free survival was 6 months (95% CI 5.1-6.9), and the median overall survival was 17 months (95% CI 14.5-19.5):
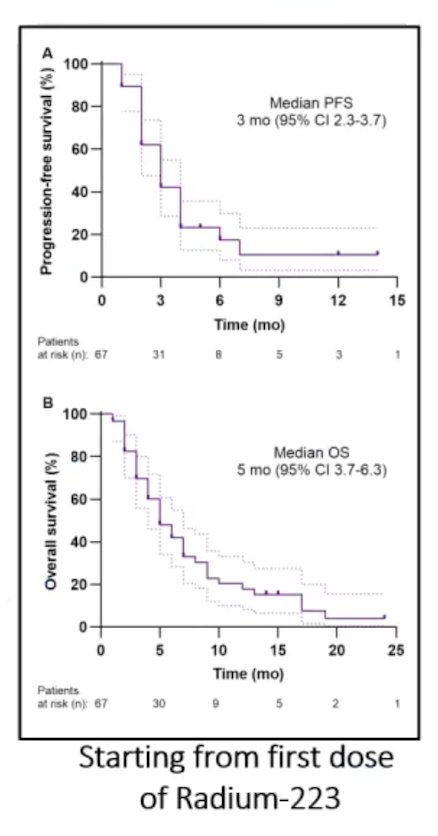
Starting from the first dose of radium-223, the median progression-free survival was 3 months (95% CI 2.3-3.7), and the median overall survival was 5 months (95% CI 3.7-6.3):
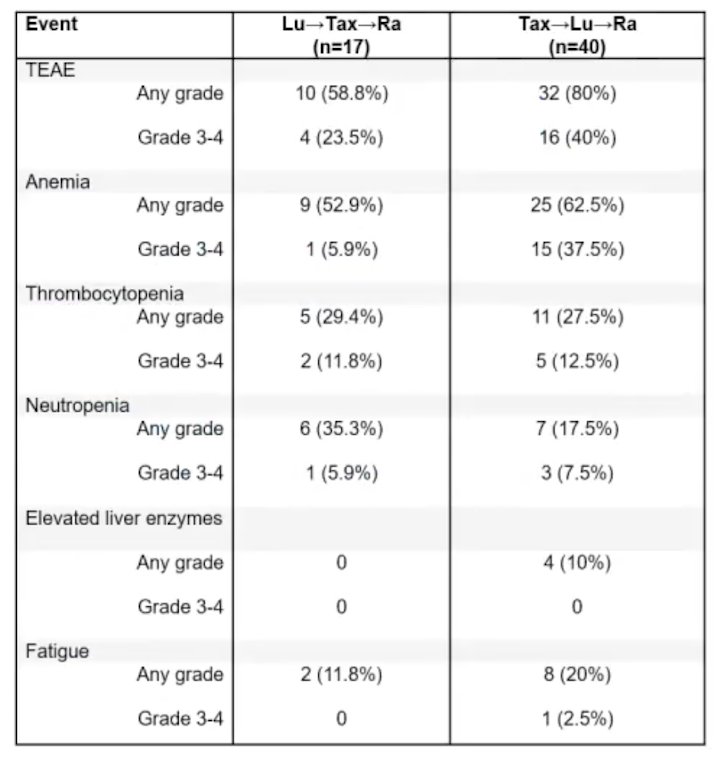
For patients receiving 177Lu-PSMA followed by taxane chemotherapy followed by radium-223, the any-grade adverse event rate was 58.8%, and the grade 3-4 adverse event rate was 23.5%. For patients receiving taxane chemotherapy followed by 177Lu-PSMA followed by radium-223, the any grade adverse event rate was 80%, and grades 3-4 adverse event rate was 40%:
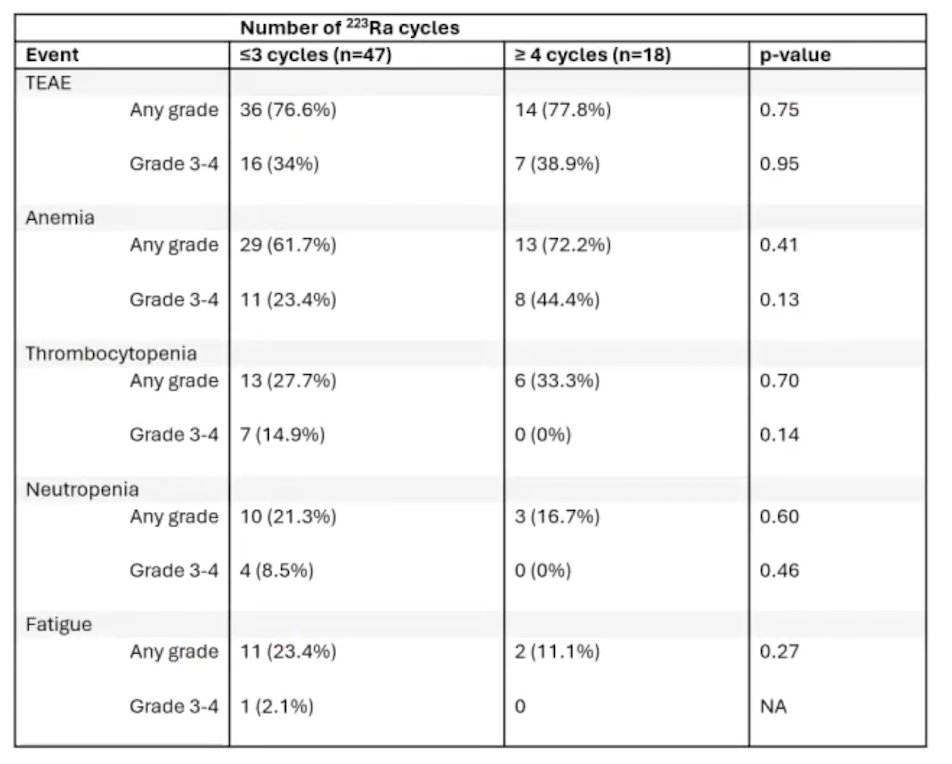
Additionally, based on cycles of radium-223 received, there was no difference in treatment emergent adverse events, anemia, thrombocytopenia, neutropenia, and fatigue of any grade and grade 3-4:
Dr. Rahbar concluded this presentation discussing safety and survival outcomes of radium-223 in patients with mCRPC with prior 177Lu-PSMA radioligand therapy in the LuRa study, with the following take-home points:
- Sequential LuPSMA → radium-223 is feasible: real-world data demonstrate successful delivery of sequential therapy
- There was an acceptable safety profile in heavily pretreated mCRPC: toxicity rates were consistent with prior reports of radium-223 in mCRPC
- The treatment interval had minimal impact on toxicity: shorter or longer intervals did not increase the risk of grade 3–4 adverse events
- Flexible sequencing appears clinically reasonable: there were no meaningful differences in survival or toxicity between sequencing strategies
- These findings support further prospective evaluation: provides a strong rationale for prospective studies to optimize sequencing and timing
Presented by: Kambiz Rahbar, MD, University Hospital Muenster, Muenster, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Society of Nuclear Medicine and Molecular Imaging (SNMMI) 2026 Annual Meeting, Los Angeles, CA, Sat, May 30 – Tues, Jun 2, 2026.