(UroToday.com) The 2026 SNMMI annual meeting featured a genitourinary diagnosis and imaging session, including a presentation by Dr. Surekha Yadav discussing longitudinal outcomes of PSMA PET/CT-detected bone oligometastases. PSMA PET detects bone metastases with higher sensitivity than conventional imaging, yet the long-term outcomes of patients with bone-only oligometastatic disease identified at initial staging remain poorly characterized. Thus, Dr. Yadav and colleagues evaluated upstaging rates, treatment patterns, and longitudinal outcomes in patients with 1–5 bone-only metastases on initial staging PSMA PET/CT.
Utilizing the PSMA PROGRESS database, the investigators retrospectively selected patients from two academic centers who had five or fewer osseous metastases on PSMA PET initial staging. Patients were stratified into three cohorts: no distant metastases (n = 984), single osseous lesion (n = 27), and 2–5 osseous lesions (n = 9). Conventional imaging (CT, MRI, bone scan) was reviewed to determine upstaging rates from clinical M0 to M1. Time to biochemical recurrence, castration resistant prostate cancer (CRPC), a composite endpoint of biochemical recurrence or CRPC, and overall survival were calculated. Kaplan Meier survival analysis with log-rank testing and Cox proportional hazards regression were performed over a median follow-up of 25 (IQR 10-65) months. Treatment patterns, including systemic intensification (ADT with androgen receptor pathway inhibitor or chemotherapy) and metastasis-directed therapy, were recorded. Patient demographics and baseline characteristics are shown in the following table:
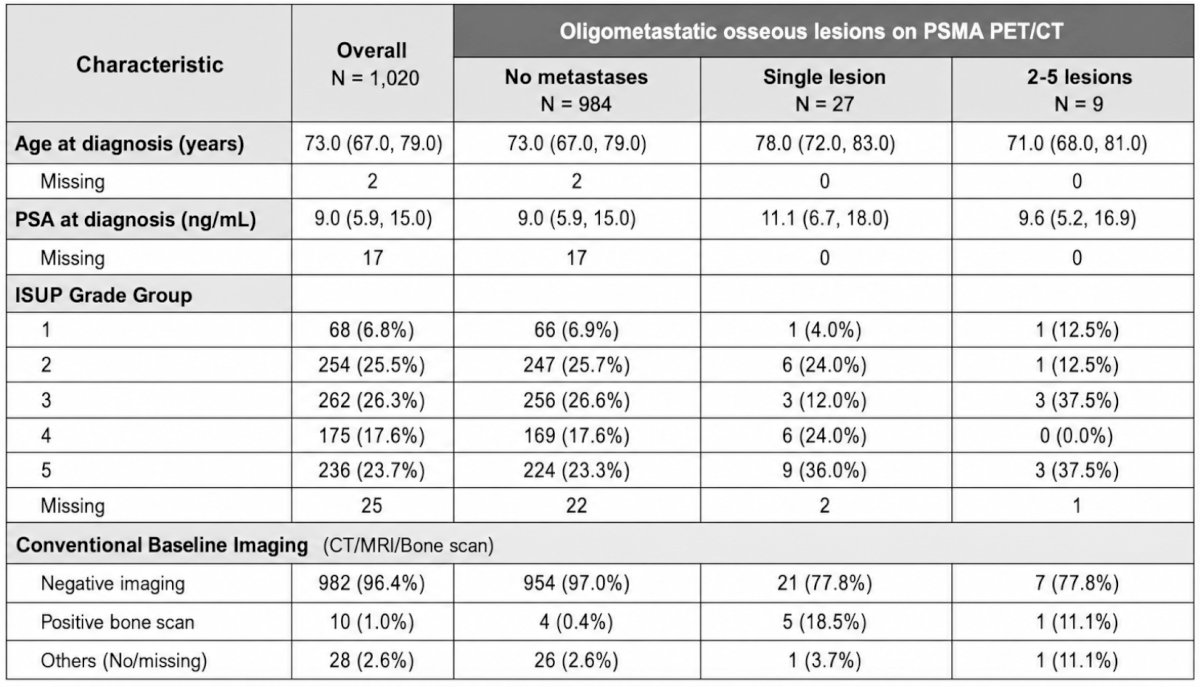
PSMA PET identified 1-5 osseous lesions in 36/1,020 patients (3.5%). Of the 36 patients with oligometastatic disease, 35 had both conventional imaging and PSMA PET performed at baseline. Of these, 28 (77.8%) had negative conventional imaging, yielding an overall upstaging rate of 82.9% from clinical M0 to M1. Upstaging occurred in 21/26 (80.8%) of single lesion and 7/9 (88.9%) of 2–5 lesion patients. ISUP Grade Group 5 was present in 36.4% of patients with 1–5 bone lesions compared to 23.3% of patients with PSMA PET M0 disease. On Cox regression, patients with 1–5 osseous lesions demonstrated significantly worse outcomes compared to those with PSMA PET/CT M0 disease: HR 5.42 for CRPC (95% CI 3.12–9.45; p < 0.001) and HR 3.81 for death (95% CI 1.68–8.61; p = 0.013). Kaplan-Meier analysis across all three cohorts confirmed significantly inferior CRPC-free survival (log-rank p < 0.0001) and overall survival (log-rank p = 0.013) in patients with osseous lesions:
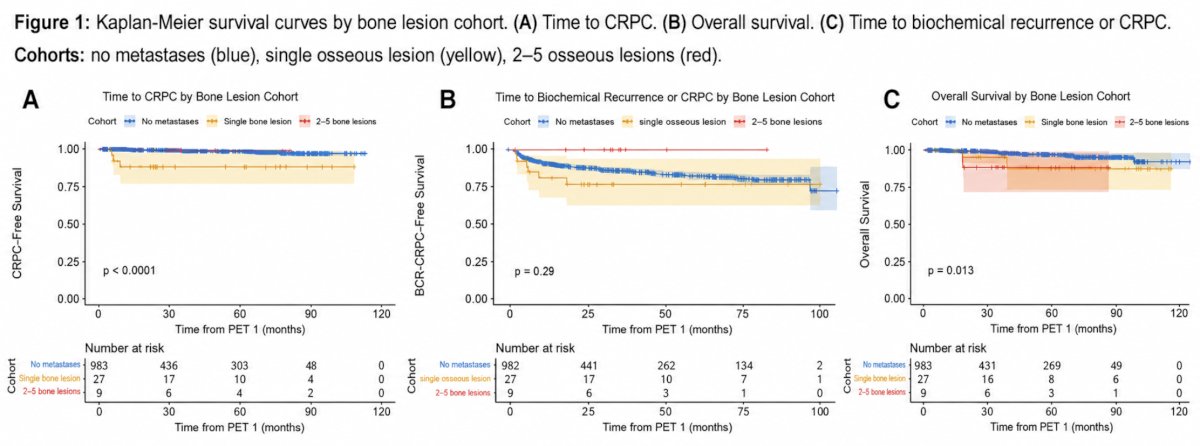
All oligometastatic patients (36/36, 100%) received systemic intensification compared to 646/984 (65.7%) of patients with M0 disease. Metastasis-directed therapy during the hormone-sensitive phase was administered to 13/27 (48.0%) of single-lesion and 2/9 (22.2%) of 2–5 lesion patients. On subgroup analysis, patients with a single osseous lesion progressed to CRPC faster than those with 2–5 lesions (p < 0.0001). However, the composite endpoint of biochemical recurrence or CRPC showed no significant difference across cohorts (log-rank p = 0.29). This discordance indicates that patients with 2–5 osseous lesions frequently bypassed biochemical recurrence, transitioning directly to CRPC under sustained systemic therapy, whereas single-lesion patients followed a conventional biochemical recurrence to CRPC trajectory. Despite 48.0% of single-lesion patients receiving metastasis-directed therapy during the hormone-sensitive phase, their faster progression to CRPC suggests a therapeutic gap wherein limited visible disease may prompt less durable systemic regimens compared to higher-burden oligometastatic disease.
Dr. Yadav concluded this presentation discussing longitudinal outcomes of PSMA PET/CT-detected bone oligometastases with the following take-home points:
- PSMA PET/CT upstages over 80% of patients with osseous oligometastatic prostate cancer from clinical M0 to M1
- These patients harbor aggressive histology and demonstrate significantly elevated risk of CRPC and death despite therapeutic intensification
- The faster progression to CRPC in single lesion patients, despite higher rates of metastasis-directed therapy, suggests that very limited visible disease may be undertreated systemically
Presented by: Surekha Yadav, MBBS, University of California San Francisco, San Francisco, California
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Society of Nuclear Medicine and Molecular Imaging (SNMMI) 2026 Annual Meeting, Los Angeles, CA, Sat, May 30 – Tues, Jun 2, 2026.