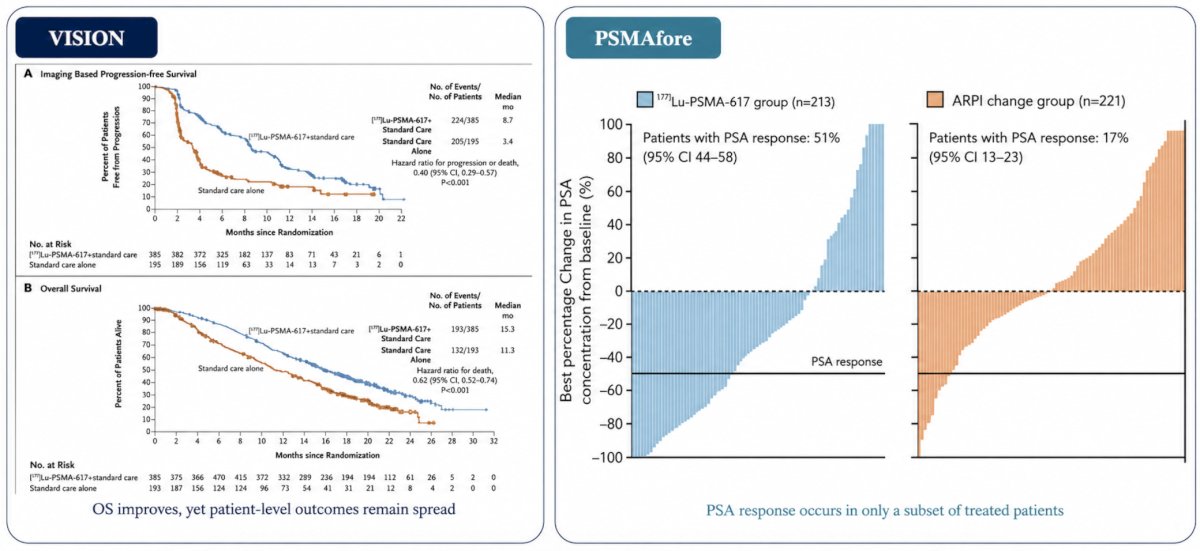
(UroToday.com) The 2026 SNMMI annual meeting featured a clinical diagnosis and therapy session and a presentation by Dr. Wen Sijie discussing metabolic tumor phenotype determining radiation delivery and outcomes in PSMA radiopharmaceutical therapy for advanced prostate cancer. Response to PSMA radiopharmaceutical therapy in metastatic castration-resistant prostate cancer (mCRPC) is heterogeneous: In VISION,1 overall survival was improved with 177Lu-PSMA, yet patient-level outcomes varied, and in PSMAfore,2 PSA response occurred in only a subset of treated patients:
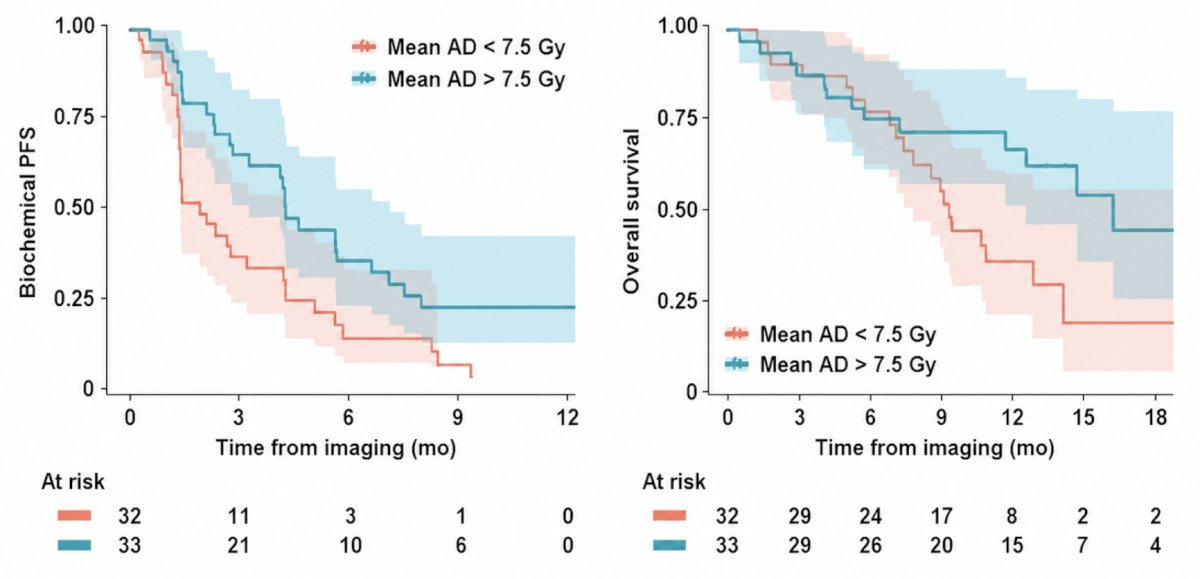
If outcomes vary, the next question is whether lesion phenotype changes the absorbed dose. A higher absorbed dose is associated with longer biochemical progression-free survival and overall survival, but phenotype-specific dose absorption remains unknown:
Both lesion absorbed dose and dual-tracer 68Ga-PSMA/18F-FDG PET phenotypes are prognostic, but their interaction is not well defined. Thus, Dr. Sijie and colleagues aimed to determine how metabolic phenotype relates to lesion absorbed dose and whether phenotype-specific dose associates with biochemical response, progression-free survival, and overall survival in patients with mCRPC treated with 177Lu-PSMA.
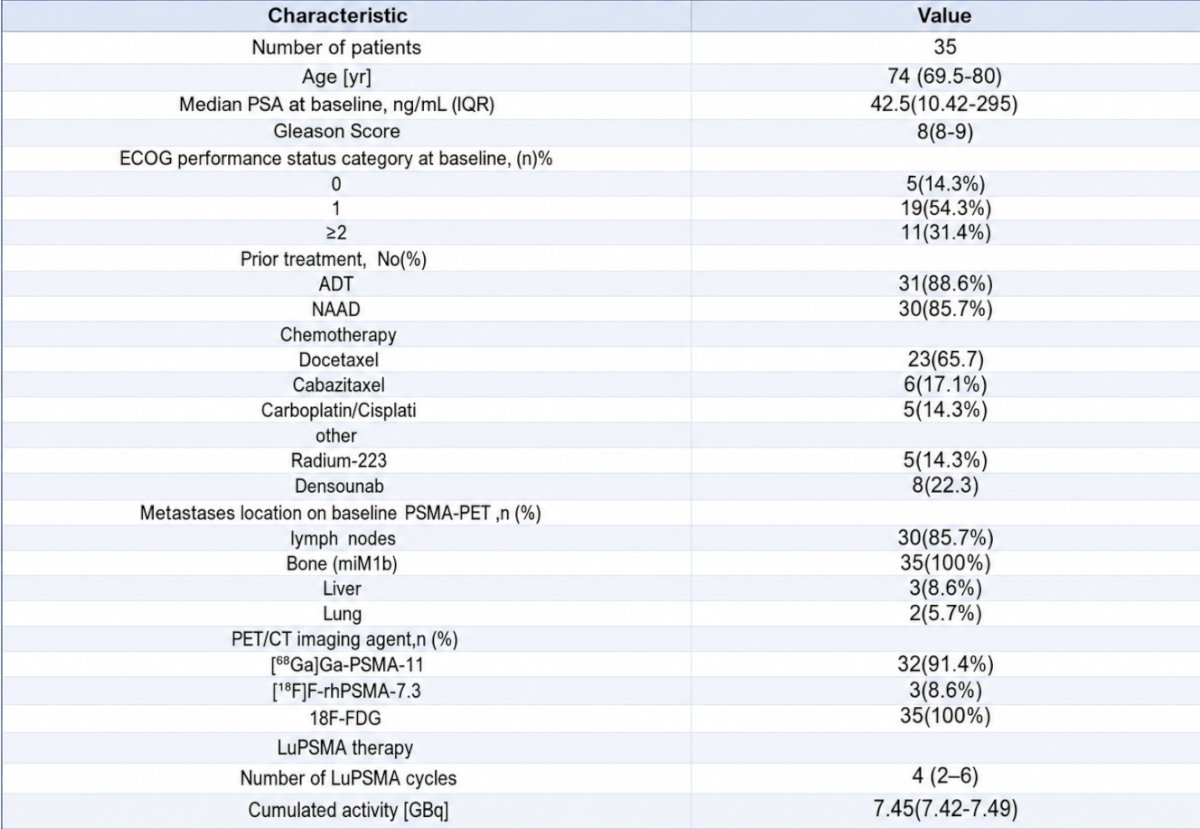
In this retrospective single-center study, 35 patients with mCRPC who received at least two cycles of 177Lu-PSMA and underwent pre-therapy 68Ga-PSMA and 18F-FDG PET/CT + post-therapy SPECT/CT were included. The patient characteristics were as follows:
Lesions were segmented on both PET tracers and classified as PSMA-positive/FDG-negative (PSMA+/FDG−) or PSMA-positive/FDG-positive (PSMA+/FDG+). Within PSMA+/FDG+ disease, lesions were further categorized as PSMA-dominant or FDG-dominant. Voxel-wise absorbed dose maps were derived from SPECT:

Biochemical response was assessed by PSA decline after two cycles. Progression-free survival and overall survival were analyzed using Kaplan-Meier and Cox models.
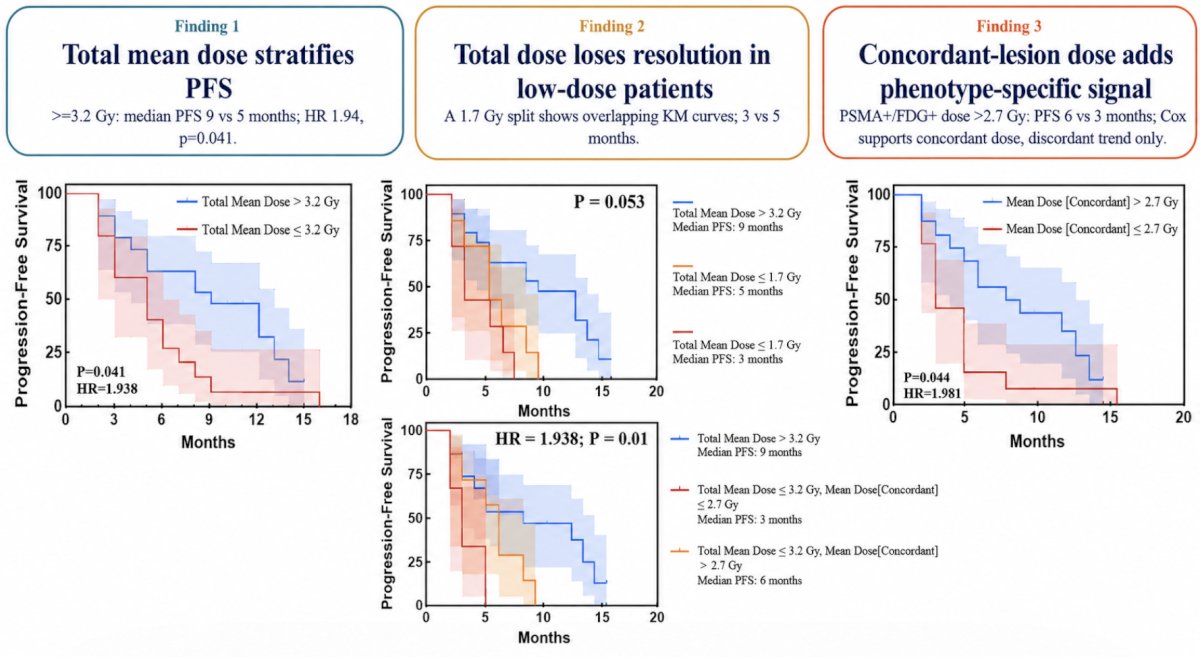
Lesion radiation delivery differed by metabolic phenotype. PSMA+/FDG− lesions received higher absorbed doses than PSMA+/FDG+ (concordant) lesions (median 2.10 versus 1.78 Gy; p < 0.0001). Within PSMA+/FDG+ disease, PSMA-dominant lesions received higher doses than FDG-dominant lesions (median 2.2 versus 1.3 Gy; p<0.0001):

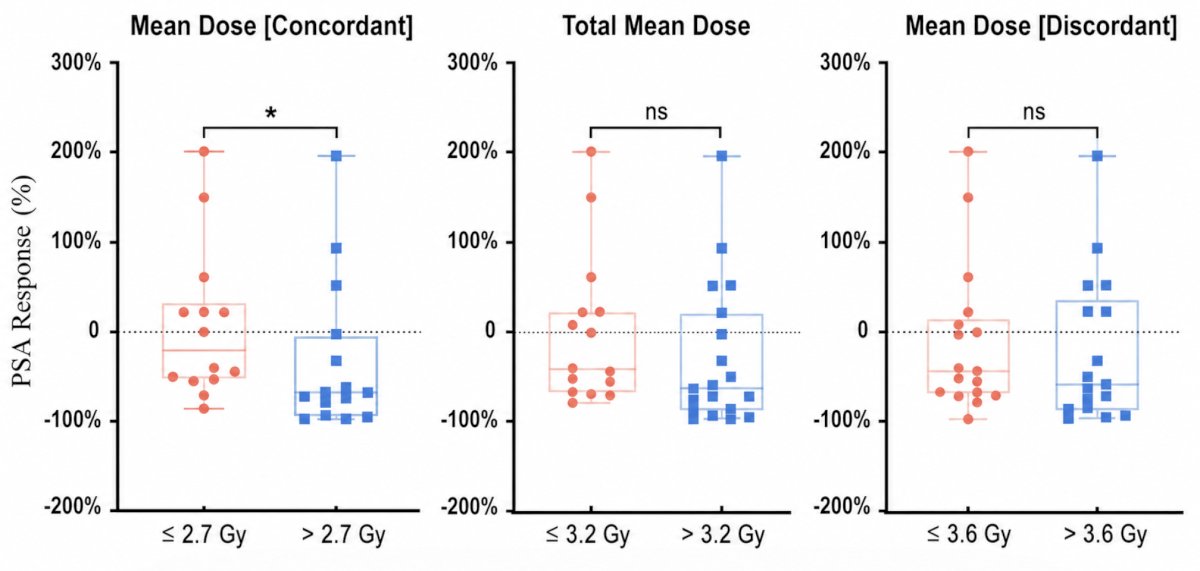
Importantly, biochemical response depended on phenotype-specific dose: only mean absorbed dose to PSMA+/FDG+ lesions stratified PSA change (median PSA decline 67.2% for >2.7 Gy versus 20.0% for ≤2.7 Gy; p = 0.04):
Higher overall mean lesion dose was associated with longer progression-free survival (9 versus 5 months; HR 1.94, p = 0.041) and overall survival (21 versus 10 months; HR 3.34, p = 0.008), but among patients with lower overall doses, PSMA+/FDG+ lesion dose remained the sole discriminator of progression-free survival (6 versus 3 months; p = 0.044):
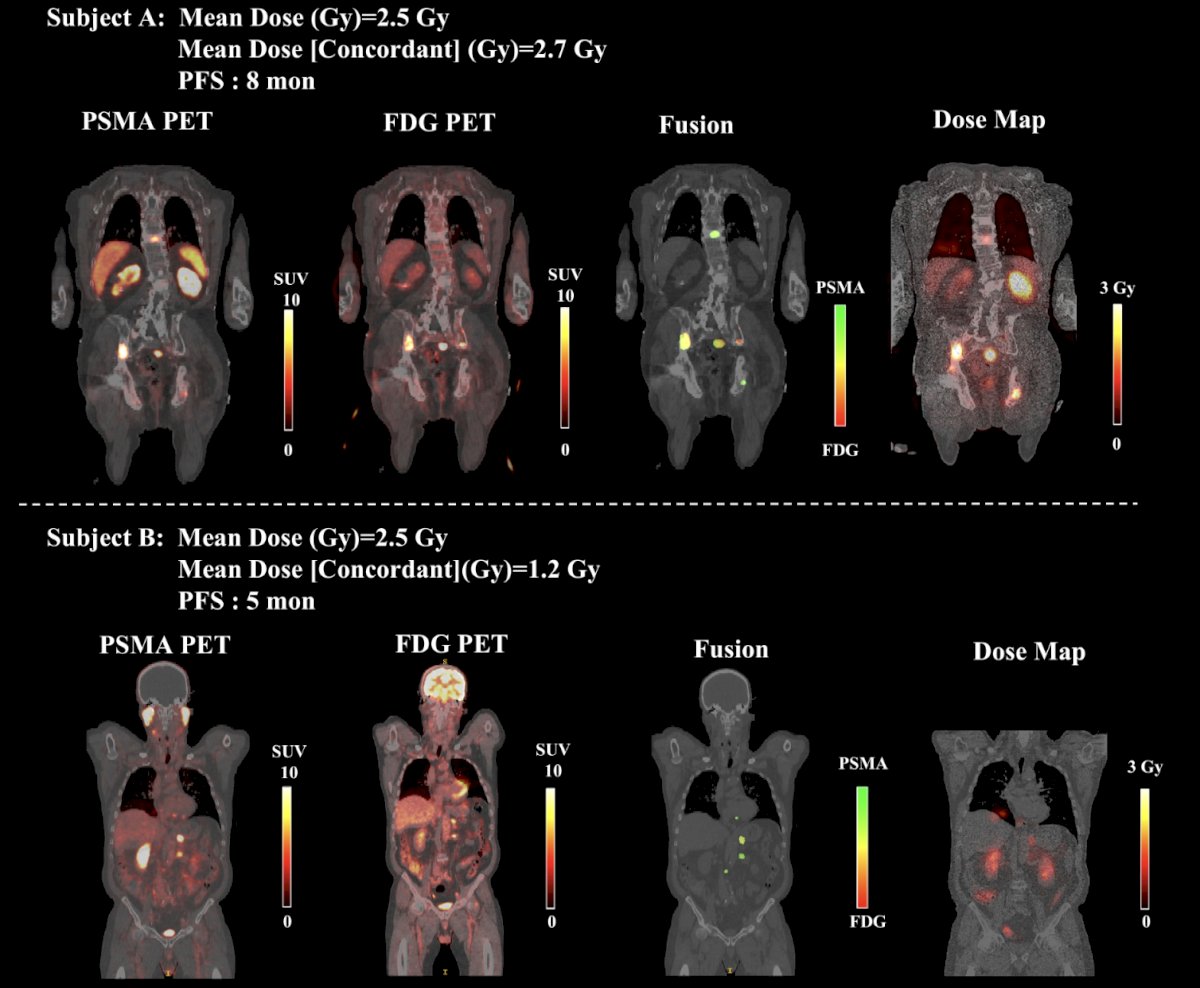
The following figure shows two representative patients with a low overall mean lesion absorbed dose. For each patient, the mean absorbed dose across all lesions and the mean absorbed dose in PSMA+/FDG+ (concordant) lesions are displayed, together with the corresponding progression-free survival interval:
Dr. Sijie noted the following limitations with this study:
- Retrospective, modest-sized cohort, and an exploratory analysis
- Residual confounding remains possible
Dr. Sijie concluded his presentation discussing metabolic tumor phenotype determining radiation delivery and outcomes in PSMA radiopharmaceutical therapy for advanced prostate cancer with the following take-home points:
- Mean absorbed dose to PSMA+/FDG+ lesions was more closely associated with biochemical response and progression-free survival than global mean lesion dose
- Phenotype-specific lesion dosimetry may provide clinically relevant information beyond global dose metrics and warrants prospective validation to refine patient selection and personalize PSMA radiopharmaceutical therapy planning
- Next steps include flagging underdosed or FDG-dominant lesions for escalation or alternative treatment options
Presented by: Wen Sijie, Medical University of Vienna, Vienna, Austria
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Society of Nuclear Medicine and Molecular Imaging (SNMMI) 2026 Annual Meeting, Los Angeles, CA, Sat, May 30 – Tues, Jun 2, 2026.
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.