(UroToday.com) The 2026 SNMMI annual meeting featured a clinical diagnosis and therapy session and a presentation by Dr. Akshay Bedmutha discussing the safety and efficacy of rechallenge PSMA radioligand therapy in post-taxane metastatic castration resistant prostate cancer (mCRPC).
177Lu-PSMA-617 radioligand therapy has been approved by the FDA to treat post-taxane mCRPC, and more recently, expanded indication to include the taxane-naive patient population, previously treated with an androgen receptor pathway inhibitor (ARPI). The approvals were based upon the results of phase III VISION1 and PSMAfore2 trials, which demonstrated its benefits in terms of survival and objective response rates. But patients eventually progress even after a favorable initial response. At this stage, there are limited treatment options, as these patients have already been deemed non-responders to taxanes and ARPIs. In early reports, rechallenge 177Lu-PSMA-617 radioligand therapy is emerging as a potential approach, given its overall tolerability and favorable toxicity profile. The aim of this study, presented at the SNMMI 2026 annual meeting, was to evaluate the safety and efficacy of rechallenge 177Lu-PSMA-617 radioligand therapy in a post-taxane setting.
Clinical and imaging data of patients who underwent at least two cycles of 177Lu-PSMA-617 radioligand therapy with a favorable response with subsequent biochemical and radiological progression, followed by rechallenge radioligand therapy between 2023 and 2025, were retrospectively reviewed. Endpoints included biochemical (PSA) response, toxicity, PSA progression-free survival, and median overall survival. Radiological responses to initial radioligand therapy were evaluated using the Visual Response Evaluation Criteria in PSMA Imaging (vRECIP) criteria. PSA progression was defined per the PCWG3 criteria as ≥25% and an absolute increase of ≥2 ng/mL confirmed by repeat measurement ≥3 weeks apart. PSA progression-free survival was calculated from the start of rechallenge radioligand therapy. Median overall survival was calculated separately from the first cycle of both initial and rechallenge radioligand therapy to the last patient contact or death. Subjective assessment for xerostomia was performed throughout the course of radioligand therapy.
175 patients underwent 177Lu-PSMA-617 radioligand therapy from 2023-2025, out of which 12 underwent rechallenge radioligand therapy. All patients met VISION PSMA PET inclusion criteria for initial and rechallenge radioligand therapy. The median age at the time of rechallenge radioligand therapy was 73.5 years (range: 54-88), and initial treatment involved a median of 6 cycles (range: 2-6):
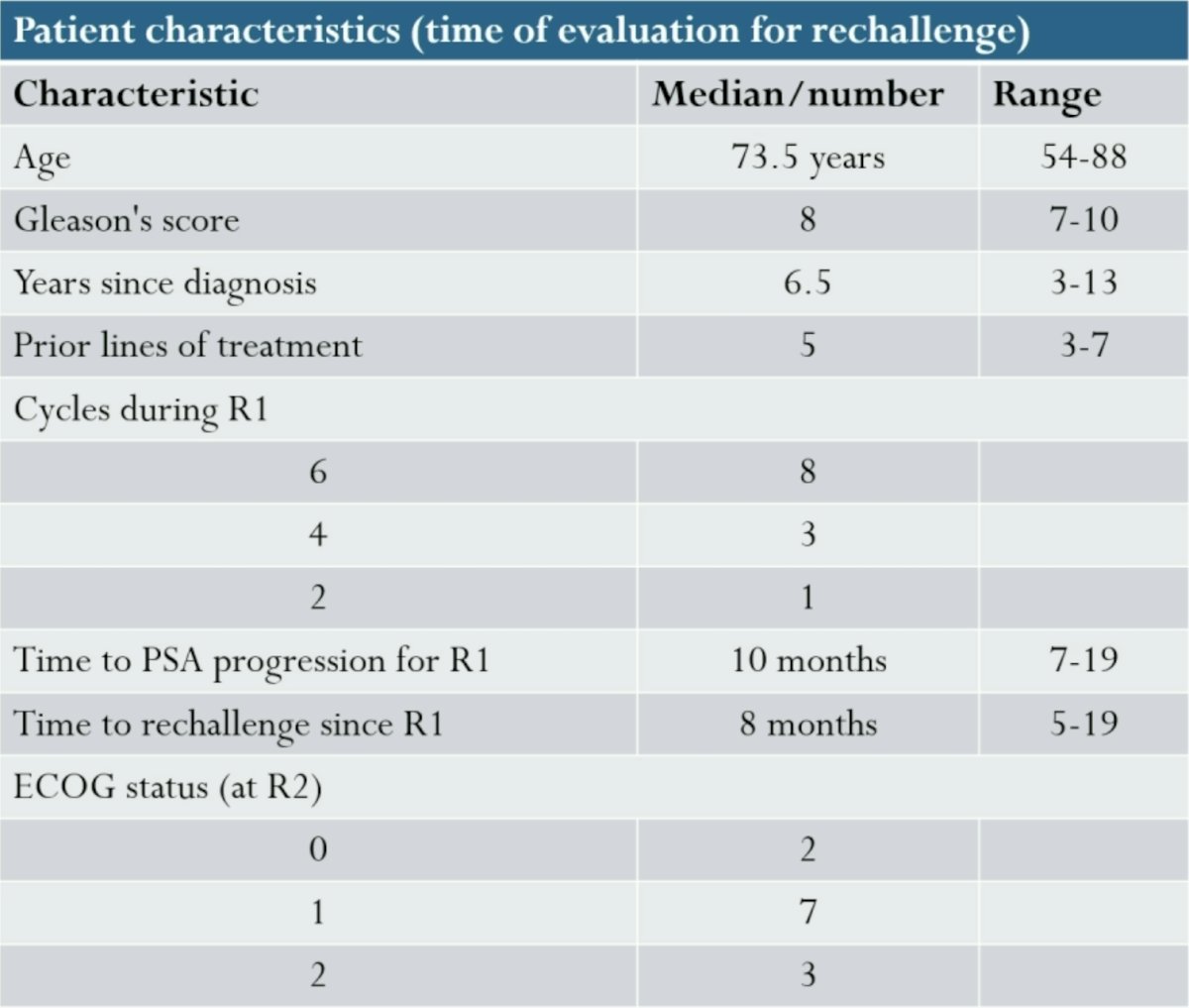
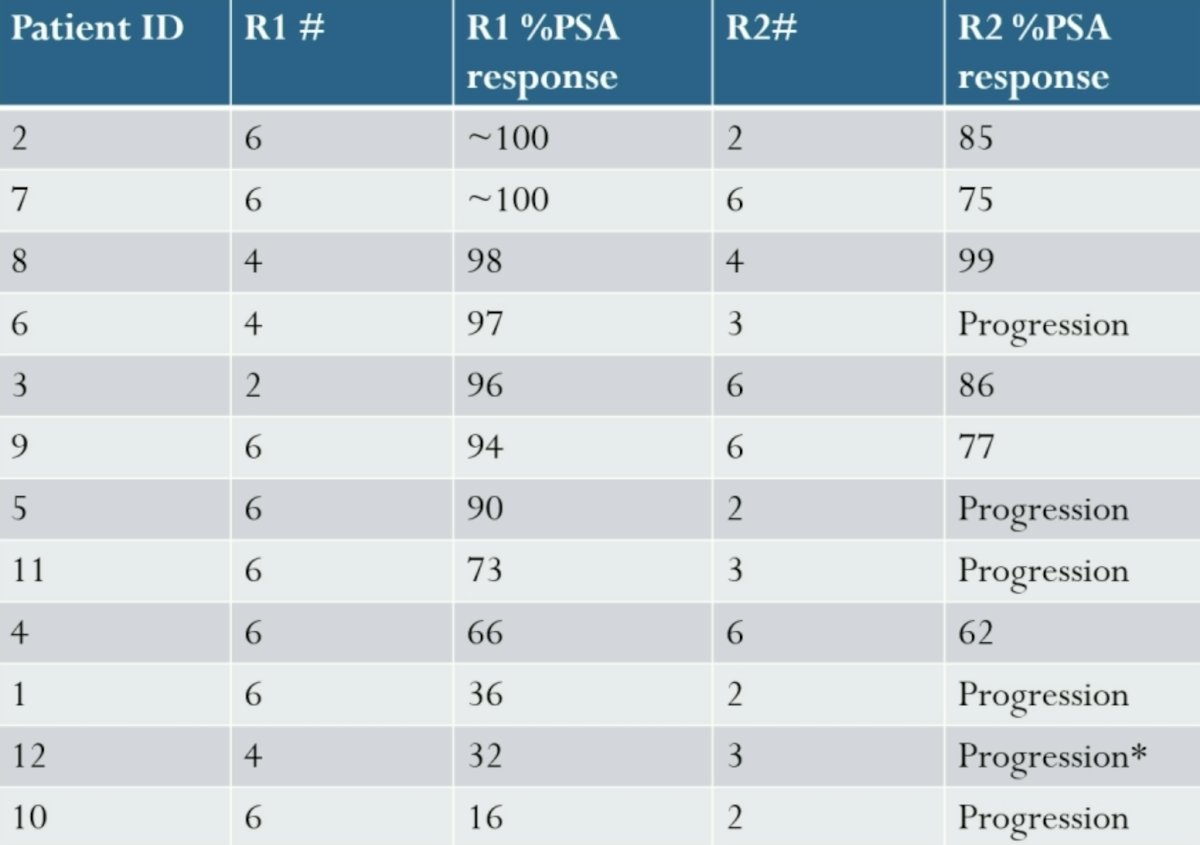
Following initial radioligand therapy, ≥50% decline in PSA (PSA50 response) was observed in 9 patients, out of which 7 patients had ≥90% decline (PSA90 response). There were 11 of 12 patients who demonstrated a favorable imaging response as per RECIP criteria (1 complete response, 10 partial responses). Appropriate response evaluation imaging was not available for 1 patient.
The median time to rechallenge from initial radioligand therapy was 8 months (range: 5-19). Pre-rechallenge PSMA PET imaging showed progressing osseous metastases in all 12 patients, 3 patients had progressing lymph node metastases, and 2 had progressing prostate gland disease. Patients were retreated with a median of 4 cycles (range: 2-6). A PSA50 response was observed in 6/12 patients (50%), out of which 1 patient had a repeat PSA90 response:
The median overall survival from initial radioligand therapy was 29 months, and from rechallenge was 9 months: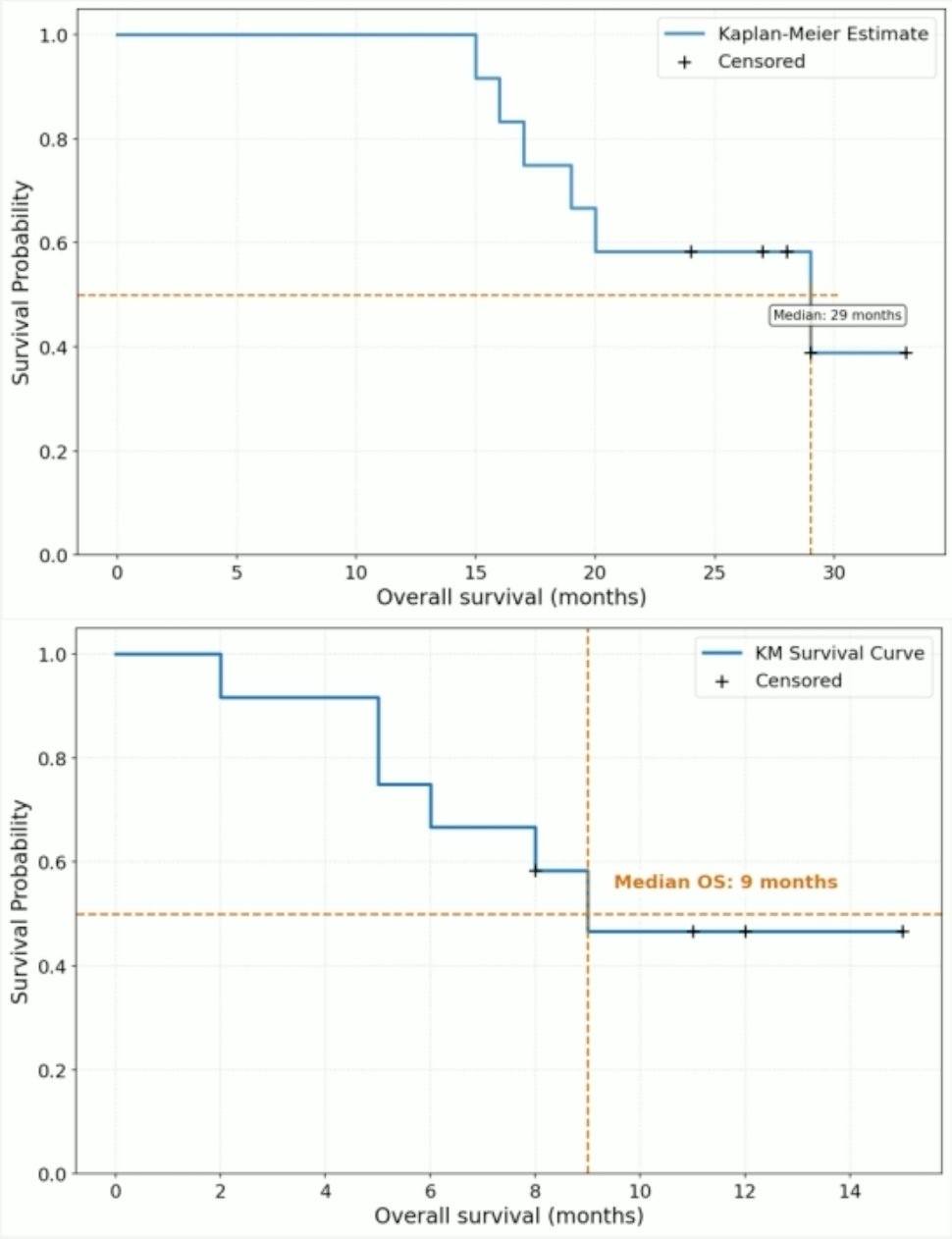
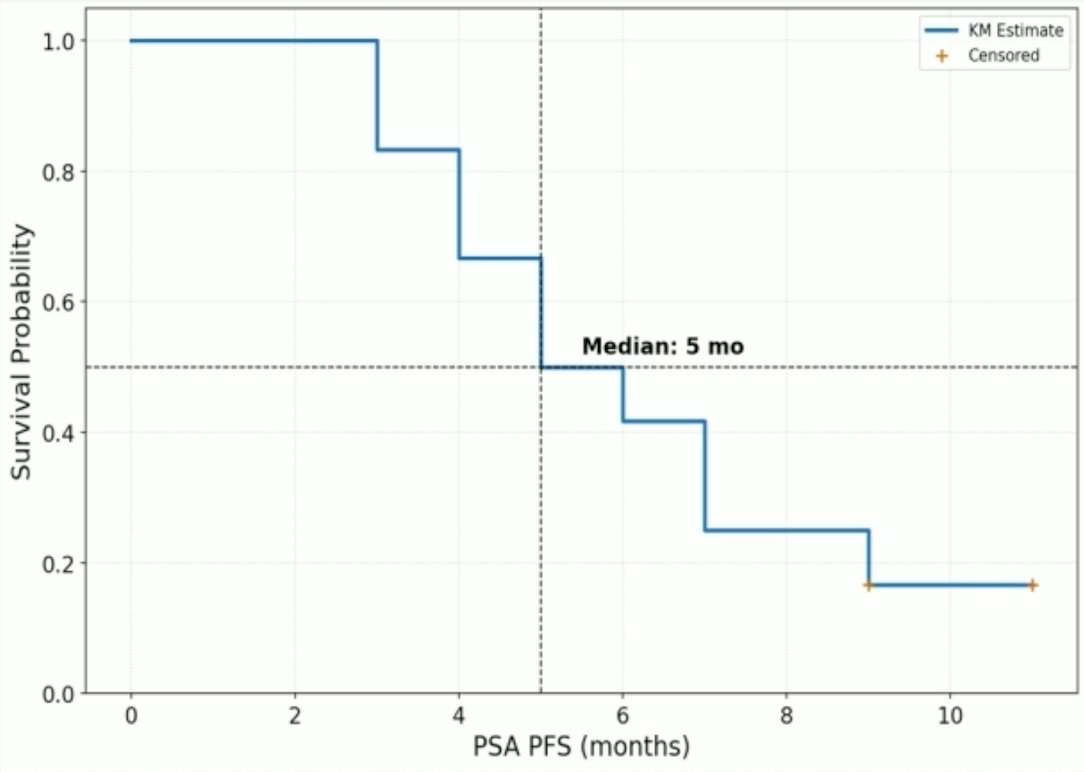
Among the responders with maximum available follow-up, the median PSA progression-free survival was 5 months (range: 2-11):
The Swimmers plot for these patients is highlighted in the following figure:
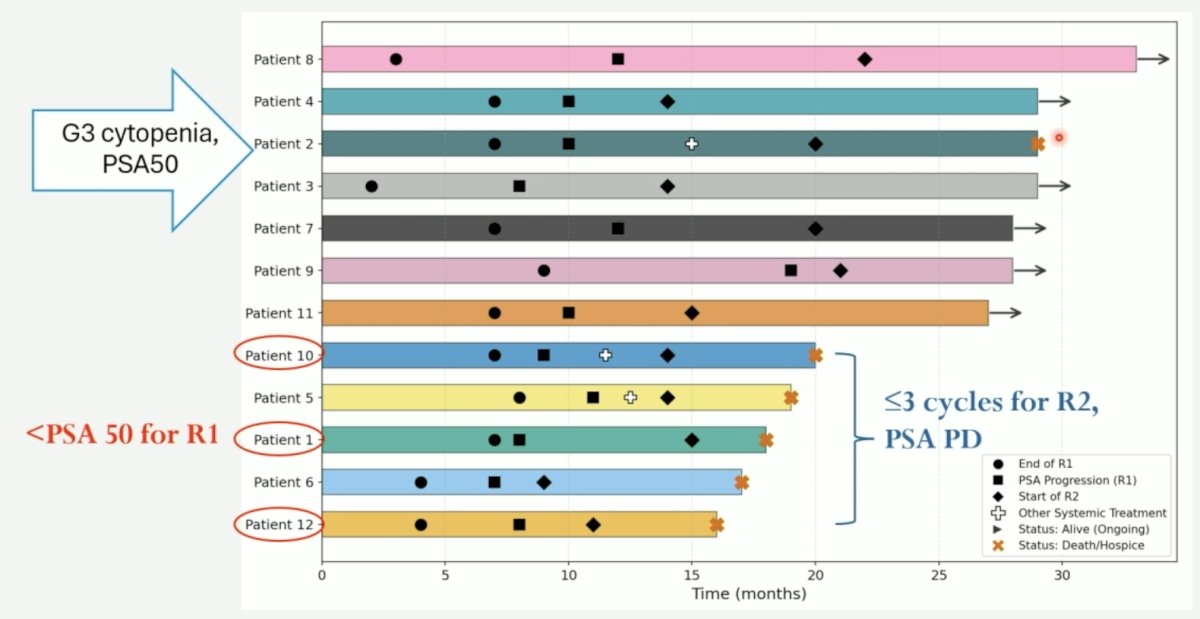
During rechallenge radioligand therapy, 6/12 patients (50%) developed worsening anemia (grade 3 in two patients), 7/12 patients (58.3%) developed thrombocytopenia (grade 3 in one patient, who also had grade 3 anemia), and 7/12 patients (58.3%) developed grade 1 or 2 leukopenia (no grade ≥3). No new or worsening renal or liver toxicity was observed, and no severe grade 3 xerostomia was observed.
Dr. Bedmutha noted several limitations to this study, including:
- Small sample size
- The long-term survival assessment is limited due to the sample size and censored data
- There was no comparative cohort; these patients were not eligible for any other treatment modality at the time of rechallenge
Dr. Bedmutha concluded his presentation discussing the safety and efficacy of rechallenge PSMA radioligand therapy in post-taxane mCRPC with the following take-home points:
- In post-taxane mCRPC, rechallenge with 177Lu-PSMA-617 appears to be a safe and tolerable strategy
- In responders, rechallenge with 177Lu-PSMA-617 can provide an acceptable PSA control
- Patients who had a less than PSA50 response after initial 177Lu-PSMA-617 treatment had a poor response to rechallenge, suggesting resistance and an aggressive phenotype
- A PSA90 response after initial 177Lu-PSMA-617 treatment suggested a favorable response to 177Lu-PSMA-617 rechallenge
- Future directions include:
- The RE-LuPSMA Trial: an ongoing phase II prospective trial, for which results are awaited
- “Are we undertreating?” We need prospective studies evaluating 177Lu-PSMA-617 beyond the standard 6 cycles used in mCRPC
- Studies with larger sample sizes and a comparative cohort (rechallenge versus PARP inhibitors/immunotherapy) are needed
Presented by: Akshay Bedmutha, MD, Assistant Professor, Emory University, Atlanta, GA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Society of Nuclear Medicine and Molecular Imaging (SNMMI) 2026 Annual Meeting, Los Angeles, CA, Sat, May 30 – Tues, Jun 2, 2026.
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.