(UroToday.com) The 2025 SNMMI annual meeting featured a kidney cancer session and a presentation by Drs. Shadi Esfahani and Timothy McClure discussing CAIX-PET imaging and the shift toward precision diagnostics in kidney cancer.
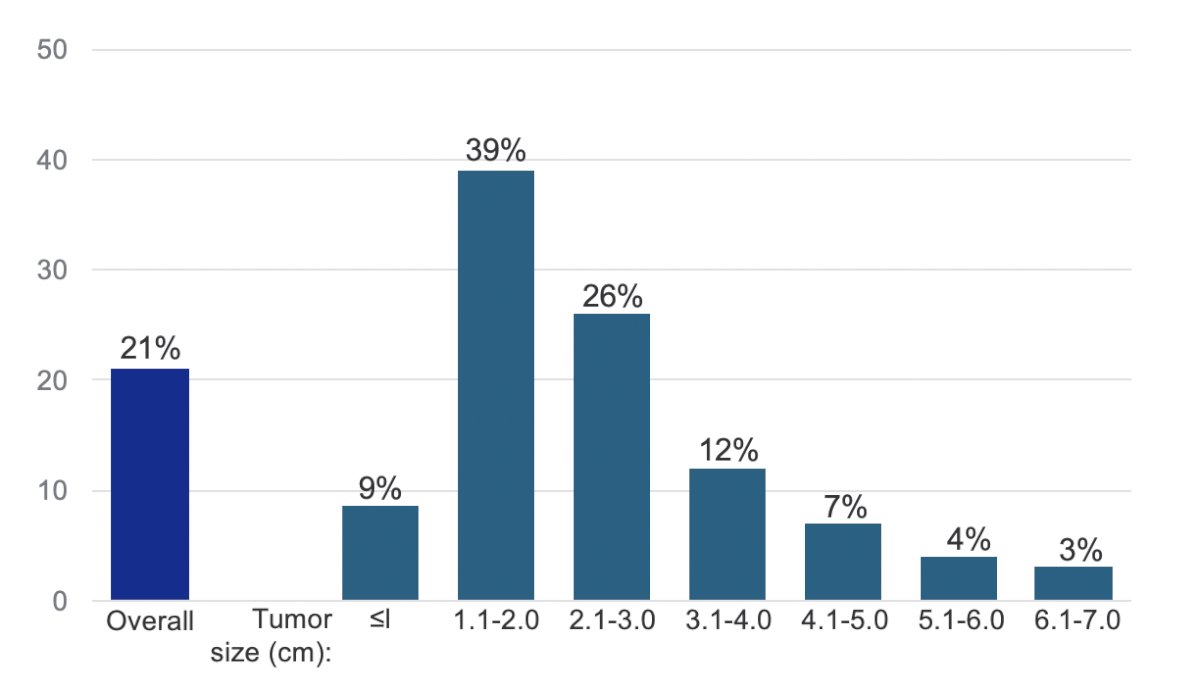
Dr. McClure started the presentation by noting that the management of indeterminate renal masses, which are renal masses that cannot be diagnosed confidently when discovered, is challenging. Moreover, the number of renal masses has increased with the growing use of cross-sectional imaging. In fact, 21% of masses qualify as indeterminate renal masses, which are most common among smaller lesions:1
 Indeterminate renal masses require careful evaluation as nearly 90% of solid masses are malignant, predominantly renal cell carcinomas (RCC), with the majority including clear cell, but also papillary and chromophobe RCC. Notably, the 5-year survival rate with clear cell RCC (all stages) is only 17%, making identification of this subtype an important part of patient management. From a benign standpoint, these masses may be oncocytomas or angiomyolipomas. When an indeterminate renal mass is detected, clinicians and patients generally have 4 choices: biopsy, thermoablation, active surveillance, or partial/radical nephrectomy:
Indeterminate renal masses require careful evaluation as nearly 90% of solid masses are malignant, predominantly renal cell carcinomas (RCC), with the majority including clear cell, but also papillary and chromophobe RCC. Notably, the 5-year survival rate with clear cell RCC (all stages) is only 17%, making identification of this subtype an important part of patient management. From a benign standpoint, these masses may be oncocytomas or angiomyolipomas. When an indeterminate renal mass is detected, clinicians and patients generally have 4 choices: biopsy, thermoablation, active surveillance, or partial/radical nephrectomy: Active surveillance is an option for some patients with indeterminate renal masses, but some of these masses may be later found to be malignant, including cases of clear cell RCC. In a study of 173 localized indeterminate renal masses followed for a median of 2 years at the Fox Chase Cancer Center, 68 required intervention due to tumor growth, patient choice, or other factors.2 Of these 68 indeterminate renal masses, 84% were malignant, including 68% that were clear cell RCC.
Active surveillance is an option for some patients with indeterminate renal masses, but some of these masses may be later found to be malignant, including cases of clear cell RCC. In a study of 173 localized indeterminate renal masses followed for a median of 2 years at the Fox Chase Cancer Center, 68 required intervention due to tumor growth, patient choice, or other factors.2 Of these 68 indeterminate renal masses, 84% were malignant, including 68% that were clear cell RCC.
Dr. McClure notes that approximately 1/3 of nephrectomies are ultimately found to be benign, with smaller renal masses being more likely to be benign than larger masses:3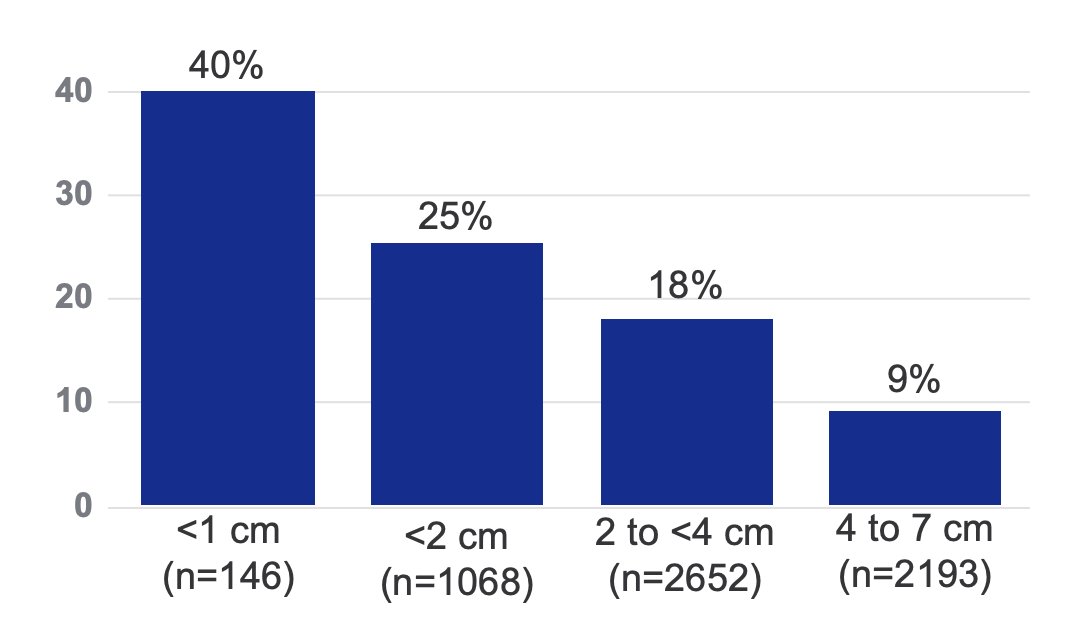
Currently, there is an unmet need for a tool that supports an accurate, reliable, noninvasive diagnosis, characterization, and differentiation of clear cell RCC. An ideal tool would likely minimize overtreatment, as seen with nearly 1/3 of resected small renal masses that are ultimately benign. While renal biopsy is sometimes considered the gold standard for diagnosis, it is invasive and has risk for complications, including hematoma, pneumothorax, and cancer seeding. Additionally, renal biopsy results are non-diagnostic in up to 15% of cases due to insufficient tissue or inaccurate biopsy location.
Urologists are looking for imaging to help define a lesion’s size, stage, and level of aggressiveness. However, current standard-of-care imaging is unable to consistently differentiate between benign and malignant masses. Single center studies in experienced centers demonstrate high sensitivity of contrast-enhanced CT and MRI, but specificity is low:4

Additionally, both sensitivity and specificity of FDG PET in imaging of primary renal masses are low.
Carbonic anhydrase IX (CAIX) is a transmembrane glycoprotein involved in oxygen-sensing pathways and a regulator of extracellular pH, which has a low expression in normal tissue but is expressed in ~95% of clear cell RCC: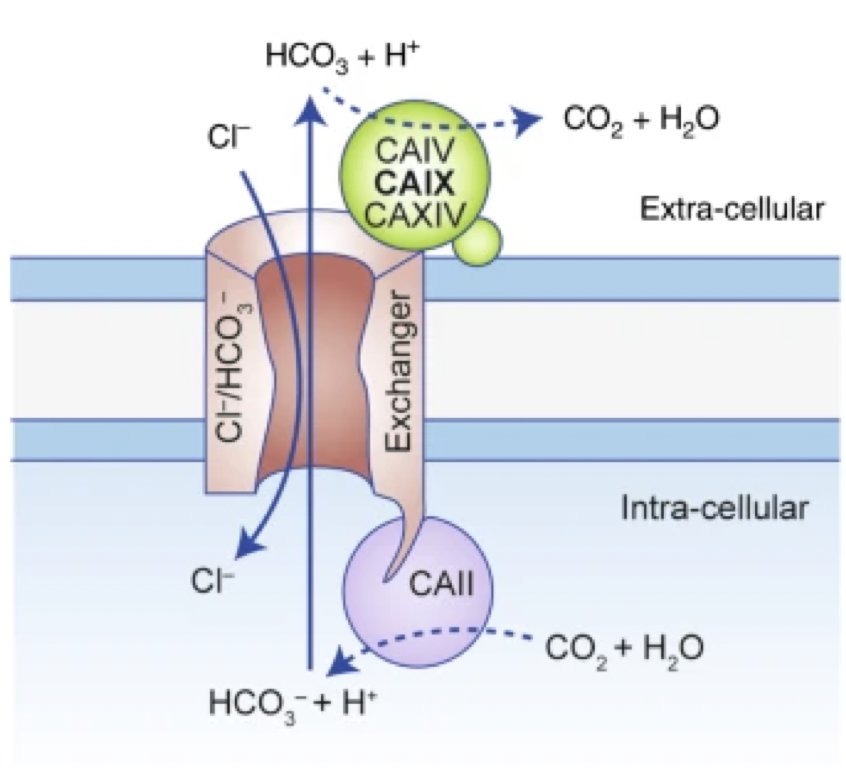
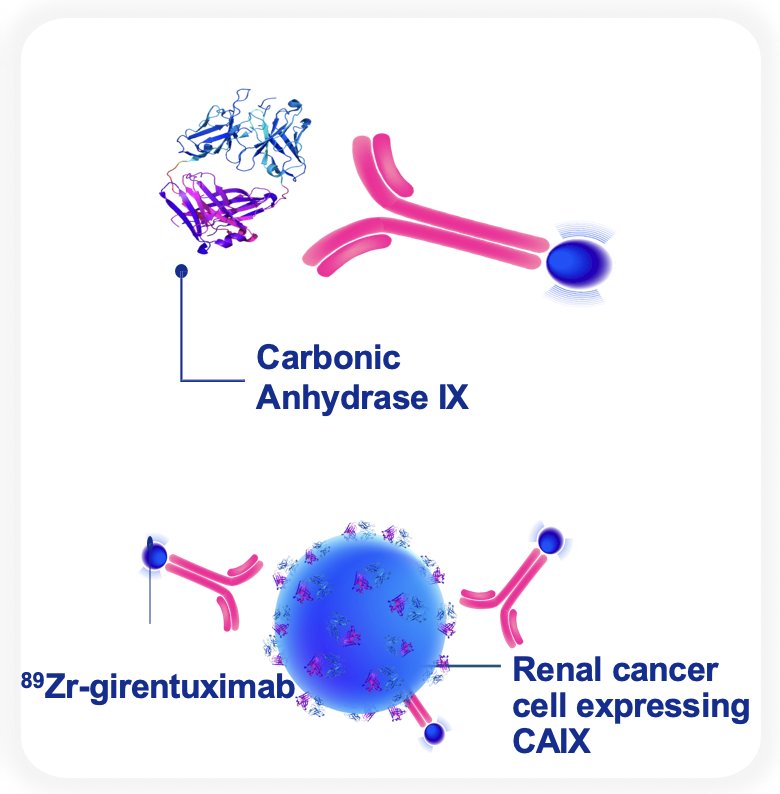
89Zr-labeled girentuximab is an investigational agent targeting CAIX for PET imaging, with hepatobiliary excretion that allows optimal renal visualization. Girentuximab is an IgG1 kappa light chain chimeric monoclonal antibody that binds with high specificity to CAIX and is internalized. The payload, 89Zr, has a half-life of 3.3 days that is well suited for antibody-based imaging, emits a lower-energy positron for improved image resolution, and reduces radiation to the thyroid compared to iodine nuclides:
89Zr-DFO-girentuximab enables excellent visualization and characterization of renal masses:
In the phase 1 ZIRDOSE trial5 (n = 10), 89Zr-DFO-girentuximab demonstrated an ability to identify clear cell RCC in 6/10 patients and was well tolerated. The ZIRDEE trial6 was an exploratory, phase 1/2 study in 30 patients with indeterminate renal mass, including patients with metastases (n = 14). Overall, 36% of patients in ZIRDEE had a major change in management as a result of 89Zr-DFO-girentuximab PET imaging, and 21% avoided repeat biopsy.
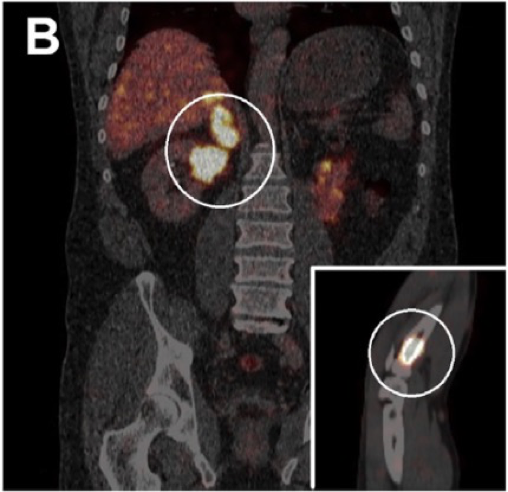 The IMPACT-RCC study7 evaluated visualization of clear cell RCC lesions in 42 patients with metastatic disease (n = 449 lesions). Patients in this study had a lesion size cutoff of 1 cm (lymph nodes up to 1.5 cm), with ultimately 56% of lesions visualized on CT, 59% visualized on 18FDG-PET/CT, and 70% visualized on 89Zr-girentuximab PET:
The IMPACT-RCC study7 evaluated visualization of clear cell RCC lesions in 42 patients with metastatic disease (n = 449 lesions). Patients in this study had a lesion size cutoff of 1 cm (lymph nodes up to 1.5 cm), with ultimately 56% of lesions visualized on CT, 59% visualized on 18FDG-PET/CT, and 70% visualized on 89Zr-girentuximab PET:
![The IMPACT-RCC study [7] evaluated visualization of clear cell RCC lesions in 42 patients with metastatic disease (n = 449 lesions). Patients in this study had a lesion size cutoff of 1 cm (lymph nodes up to 1.5 cm), with ultimately 56% of lesions visualized on CT, 59% visualized on 18FDG-PET/CT, and 70% visualized on 89Zr-girentuximab PET:](/images/com-doc-importer/221-snmmi-2025/snmmi-2025-illuminating-renal-cancer-caix-pet-imaging-and-the-shift-toward-precision-diagnostics/image-8.jpg)
To summarize his portion of the talk, Dr. McClure highlighted the following points:
- 89Zr-girentuximab targets CAIX expressed on 95% of clear cell RCC with high sensitivity, specificity, and positive predictive value
- Diagnostic performance was similarly high in patients with smaller lesions, ≤4 cm (cT1a) or ≤2 cm
- 89Zr-girentuximab is based on a differentiated monoclonal antibody approach, lending to relatively longer circulation and retention that allows for clear images of renal masses
- 89Zr-girentuximab may guide clinical decision-making and may offer potential for use in the settings of staging and recurrence/restaging
Dr. Esfahani then discussed the practical aspects of reading 89Zr-DFO-girentuximab scans. She started her portion of the presentation by noting that 89Zr-DFO-girentuximab scans improve in clarity with time as the antibody localizes to the tumor site:
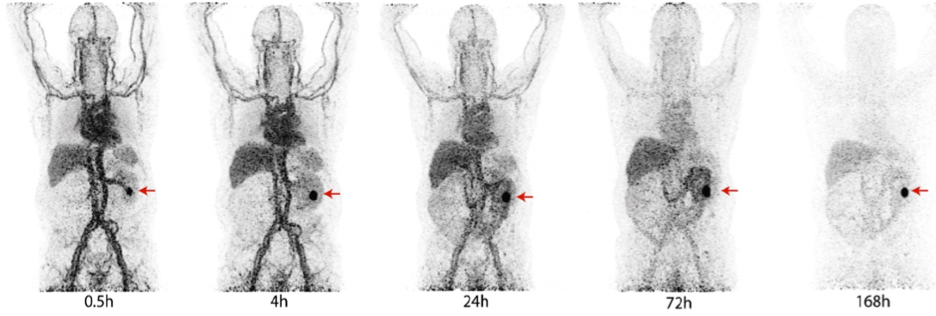
The ZIRCON trial was a prospective, open-label, multicenter, phase 3 trial that demonstrated the high diagnostic performance and favorable safety and tolerability profile of 89Zr-DFO-girentuximab PET.8 Patients with an indeterminate renal mass ≤7 cm (cT1) suspicious for clear cell RCC and who were scheduled for partial or radical nephrectomy received a single dose of 37 MBq (±10%) 89Zr-DFO-girentuximab intravenously followed by abdominal PET/CT imaging 5 ± 2 days later:
![The ZIRCON trial was a prospective, open-label, multicenter, phase 3 trial that demonstrated the high diagnostic performance and favorable safety and tolerability profile of 89Zr-DFO-girentuximab PET [8]. Patients with an indeterminate renal mass ≤7 cm (cT1) suspicious for clear cell RCC and who were scheduled for partial or radical nephrectomy received a single dose of 37 MBq (±10%) 89Zr-DFO-girentuximab intravenously followed by abdominal PET/CT imaging 5 ± 2 days later:](/images/com-doc-importer/221-snmmi-2025/snmmi-2025-illuminating-renal-cancer-caix-pet-imaging-and-the-shift-toward-precision-diagnostics/image-10.jpg)
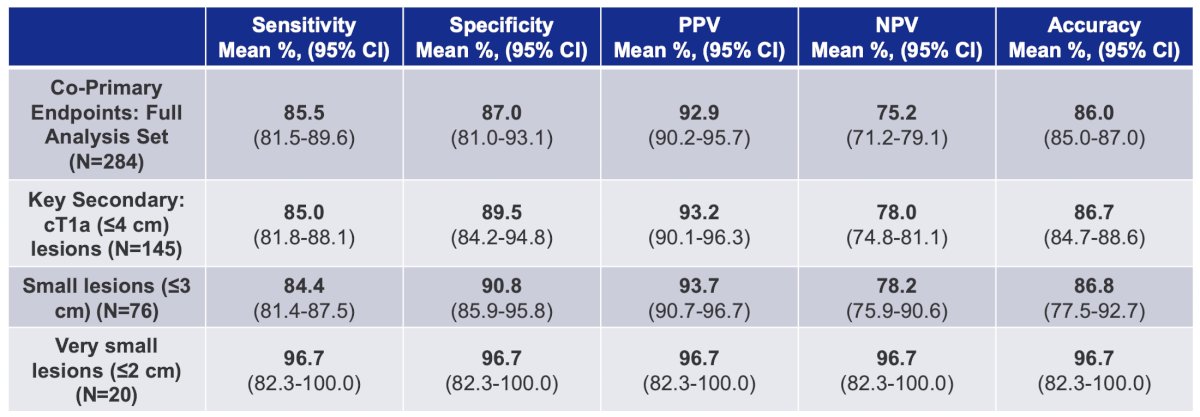
The co-primary endpoints were sensitivity and specificity of 89Zr-DFO-girentuximab PET/CT versus central histology (surgical resection) in the detection of clear cell RCC. The ZIRCON trial included 300 patients dosed and 284 included in the primary analysis. Overall, 145 patients had lesions ≤4 cm (cT1a), and 20 patients had lesions ≤2 cm, with 182 patients (63%) having clear cell RCC on central histological review:

For the co-primary endpoint, sensitivity was 85% (95% CI 81.5-89.6), and specificity was 87.0% (95% CI 81.0-93.1). The following table highlights the efficacy outcomes across the co-primary endpoint, key secondary endpoint of cT1a lesions, small lesions (<= 3 cm), and very small lesions (<= 2 cm):
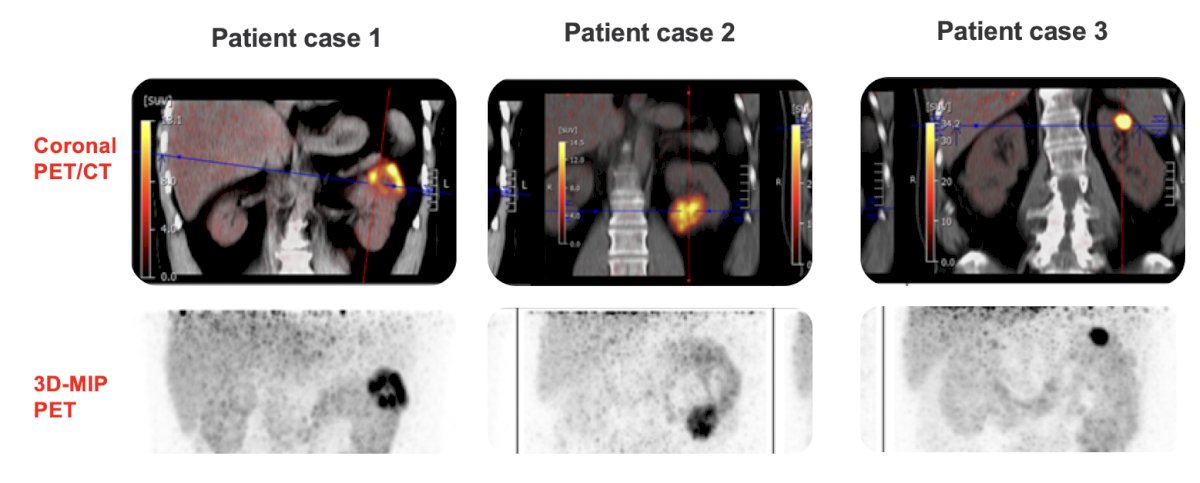
With regards to reading the 89Zr-girentuximab PET scan, Dr. Esfahani notes that the scan is positive or negative for clear cell RCC based on visual examination only. The lesion will be classified as positive if both of the following criteria are met:
- Radioactivity in the scan is clearly visible, and
- Radioactivity in the lesion is clearly greater than in normal tissue (for example, the ipsilateral or contralateral kidney)
If either of these criteria are not met, the scan is negative. Dr. Esfahani notes that patients with PET-positive clear cell RCC (true positives) had the highest SUV and tumor to background ratio. To finish her presentation, Dr. Esfahani discussed several clinical cases. The first case was a 39 year old male patient with a 1.2 cm lesion found in the right kidney. The 89Zr-girentuximab PET scan showed a lesion SUVmax of 34, with central pathology after partial nephrectomy confirming a T1a clear cell RCC:

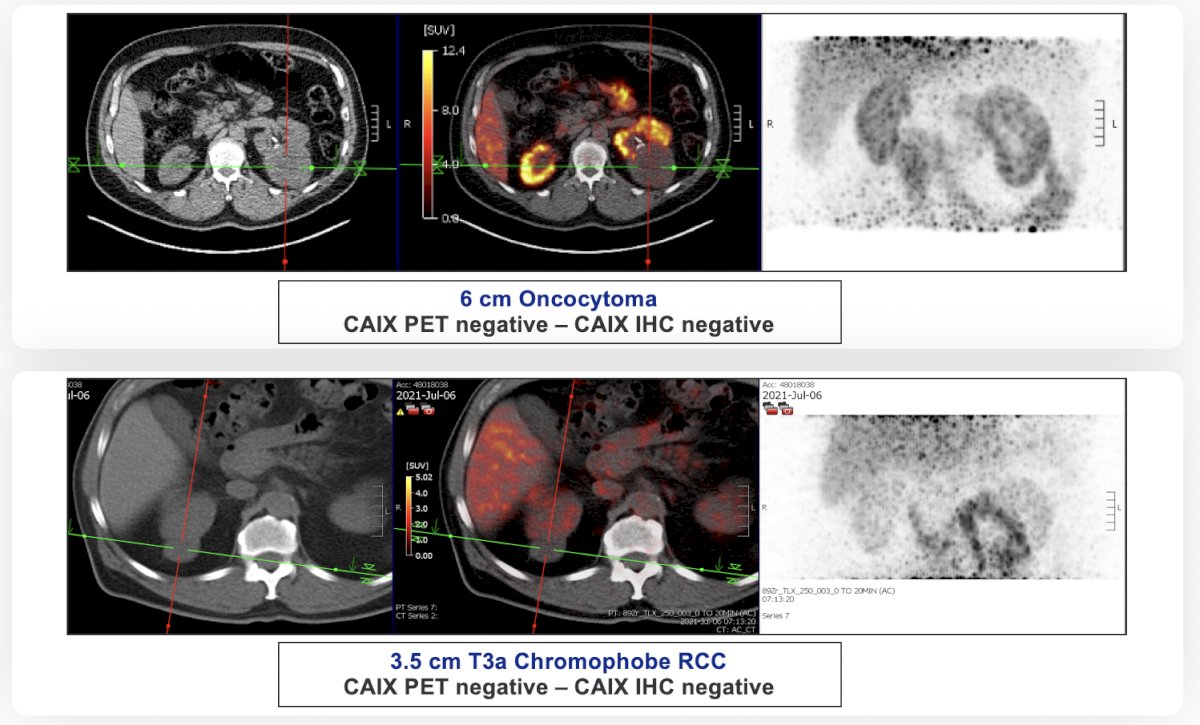
Two examples of negative cases included negative 89Zr-girentuximab PET imaging suspecting a benign lesion or non-clear cell RCC, with one patient having a 6 cm oncocytoma, and the other patient have a T3a chromophobe RCC:
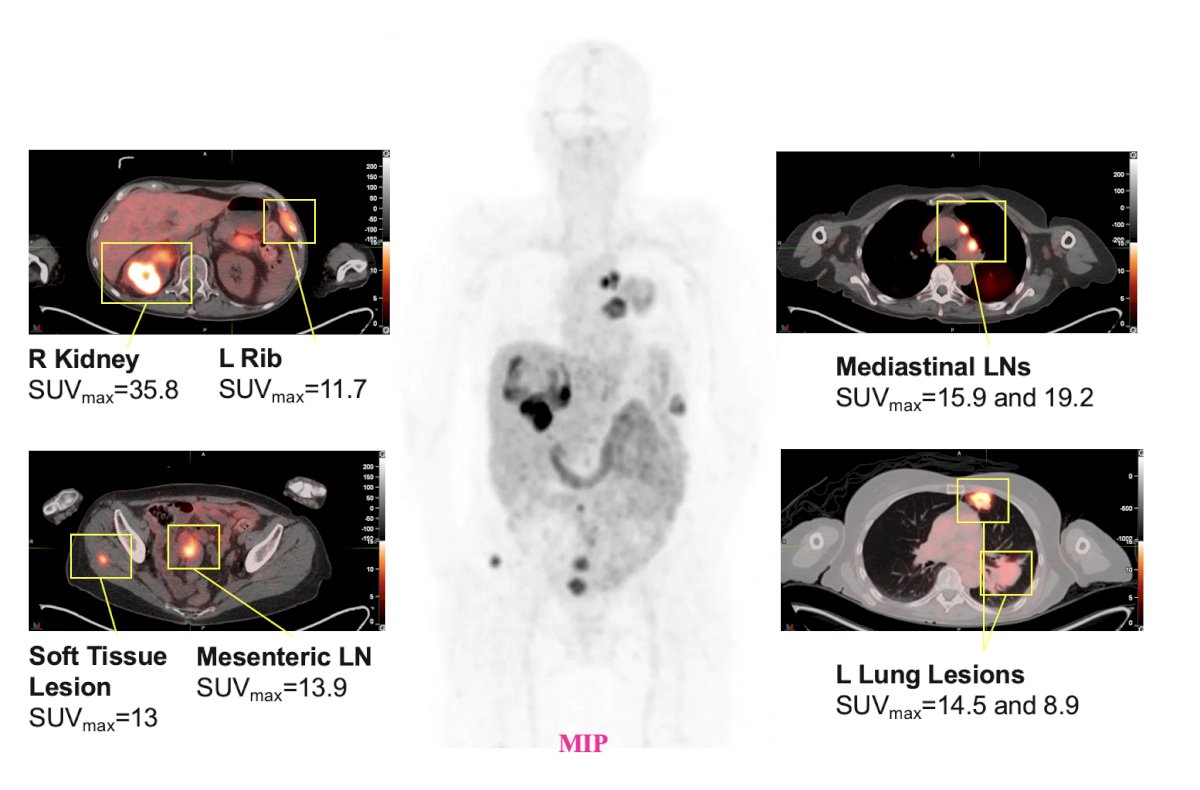
Another case was of a 68 year old female patient with metastatic RCC (clear cell and rhabdoid features), with a 89Zr-girentuximab PET scan showing a right kidney mass SUVmax 35.8, a left rib lesion SUVmax 11.7, mediastinal lymph nodes (SUVmax 15.9 and 19.2), soft tissue lesion SUVmax 13, mesenteric lymph node SUV max 13.9, and lung lesions (SUVmax 14.5 and 8.9):
Dr. Esfahani concluded her portion of the presentation with the following take home points:
- 89Zr-DFO-girentuximab PET/CT scanning provides clear images that enable characterization of clear cell RCC in patients with renal cancer with high sensitivity and specificity
- Performance is excellent even in small lesions, which may facilitate earlier diagnosis of clear cell RCC
- CAIX-directed PET scanning may offer practice-changing ability to characterize clear cell RCC and improve patient care
- For nuclear medicine physicians who want to be able to offer these scans, it is important to consider whether their site license includes 89Zr
- Sites without 89Zr on their radioactive materials license may wish to considering starting the process of adding it, as varying amounts of time may be required depending on the state and current licensure
Presented by:
- Shadi Esfahani, Massachusetts General Hospital, Boston, MA
- Timothy McClure, Weill Cornell Medicine, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Society of Nuclear Medicine and Molecular Imaging (SNMMI) 2025 Annual Meeting, New Orleans, LA, Sat, Jun 21 – Tues, Jun 24, 2025.
References:
- Butaney M, Wilder S, Patel AK, et al. Initial management of indeterminate renal lesions in a Statewide Collaborative: A MUSIC-KIDNEY Analysis. J Urol. 2023;210(1):79-87.
- Crispen PL, Viterbo R, Boorjian SA, et al. Natural history, growth kinetics, and outcomes of untreated clinically localized renal tumors under active surveillance. Cancer. 2009;115(13):2844-2852.
- Johnson DC, Vukina J, Smith AB, et al. Preoperatively misclassified, surgically removed benign renal masses. A systematic review of surgical series and United States population level burden estimate. J Urol. 2015;193(1):30-35.
- Kim J, Lee JS, Jo Y, et al. Superiority of magnetic resonance imaging in small renal mass diagnosis where image reports mismatches between computed tomography and magnetic resonance imaging. Investig Clin Urol. 2023;64(2):148-153.
- Merkx RI, Lobeek D, Konijnenberg M, et al. Phase I study to assess safety, biodistribution, and radiation dosimetry for 89Zr-girentuximab in patients with renal cell carincoma. Eur J Nucl Med Mol Imaging. 2021;48(10):3277-3285.
- Hekman MC, Rijpekema M, Aarntzen EH, et al. Positron Emission Tomography/Computed Tomography with 89Zr-girentuximab can aid in Diagnostic Dilemmas of Clear Cell Renal Cell Carcinoma Suspicion. Eur Urol. 2018;74(3):257-260.
- Verhoeff SR, van Es SC, Boon E, et al. Lesions detection by [89Zr]Zr-DFO-girentuximab and [18F]FDG-PET/CT in patients with newly diagnosed metastatic renal cell carcinoma. Eur J Nuclear Med Mol Imag. 2019;46(9):1931–1939.
- Shuch B, Pantuck AJ, Bernhard JC, et al. [89Zr]Zr-girentuximab for PET-CT imaging of clear-cell renal cell carcinoma: A prospective, open-label, multicentre, phase 3 trial. Lancet Oncol. 2024 Oct;25(10):1277-1287.