(UroToday.com) The 2025 Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Meeting held in New Orleans, LA, was host to a session on non-beta emitter PSMA radioligand therapy. Dr. David Pattison discussed the use of Lead-212 (212Pb) for the treatment of advanced prostate cancer.
What potentially makes 212Pb an ‘ideal’ isotope for alpha therapy? As summarized in the table below, 212Pb has a short range of tissue penetration (<0.1 mm) and a high linear energy transfer (LET) that induces double-stranded DNA breaks and high levels of cytotoxicity to target expressing cancer cells, irrespective of cell cycle or oxygenation state. 212Pb has a short half-life (T1/2) of 10.6 hours (compared to 10 days for 225Ac). 212Pb has limited recoil with ~70% of 212Bi retained within 212Pb chelators. 212Pb is produced by generators with 228Th or 224Ra sources, and SPECT imaging is feasible for dosimetry.

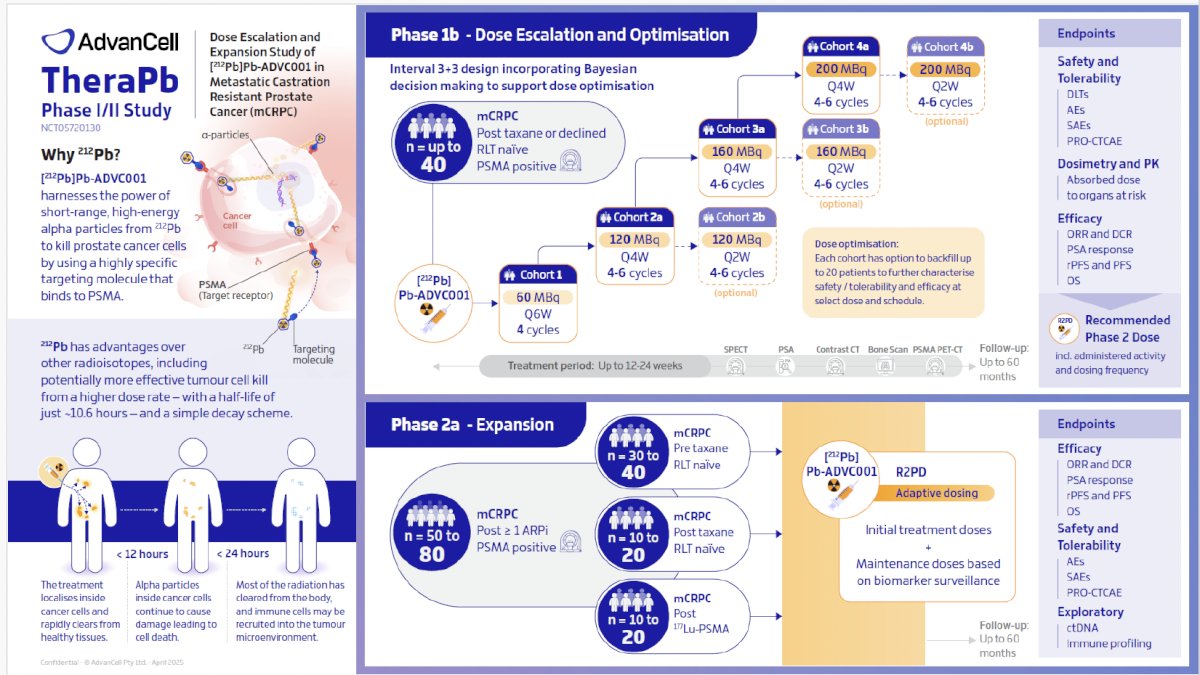
212Pb is being evaluating in numerous phase I/II clinical trials across numerous disease sites, as summarized in the table below. In the prostate cancer disease space, two trials (NCT05720130 [TheraPb]; NCT05725070) are evaluating 212Pb with PSMA as the target cell surface antigen.

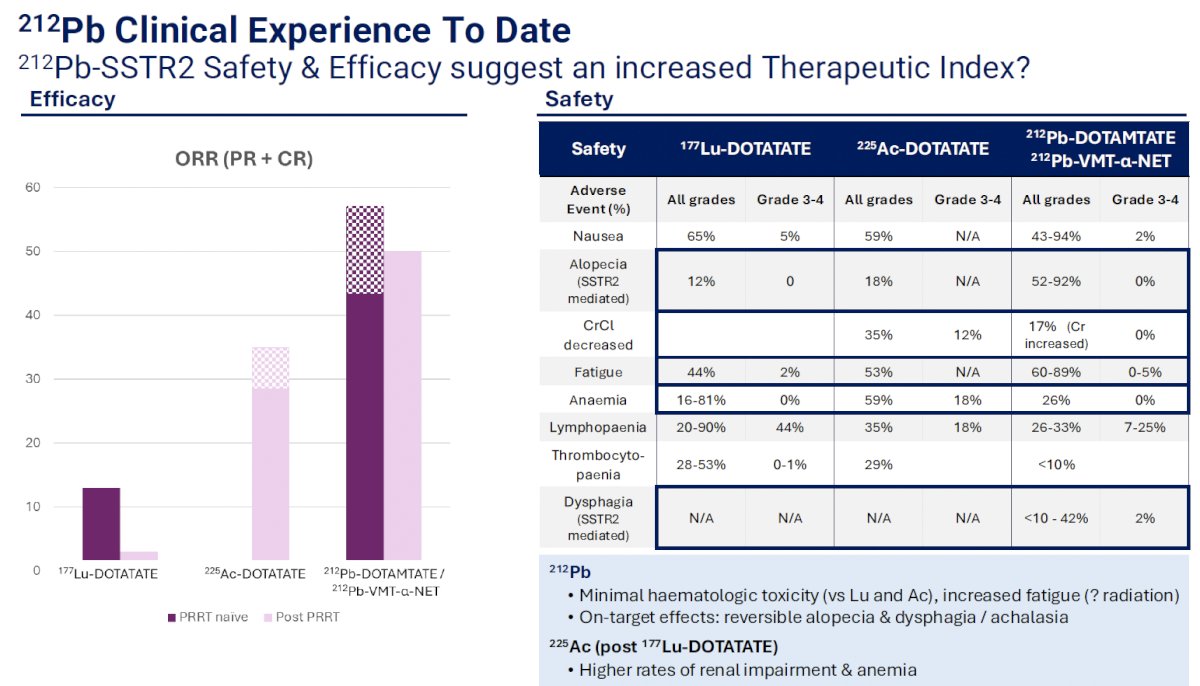
What has the early experience with 212Pb shown to date? The early safety and efficacy results suggest that there is an increased therapeutic index with 212Pb-SSTR2, compared to other alpha or beta emitters. Amongst patients with neuroendocrine tumors, 212Pb-DOTAMTATE and 212Pb-VMT-α-NET have been shown to have superior objective response rates (ORR) compared to 177Lu-DOTATATE and 225Ac-DOTATATE.1 Furthermore, these agents have been shown to have more favorable safety profiles with minimal hematologic toxicity (Grade 3 anemia: 0%), compared to 177Lu and 225Ac, with increased fatigue (all grades: 60-89% versus 44-53%). The on-target effects include reversible alopecia (all grades: 52-92%), dysphagia (all grades: 10-42%), and achalasia.
TheraPb is a prospective, open-label, non-randomized, dose-escalation, dose optimization, and expansion study. This study aims to determine the safety and tolerability of escalating doses of [212Pb]Pb-ADVC001 administered every 6, 4, or 2 weeks during the dose-finding phase (Phase 1b) in participants with PSMA-positive mCRPC who have had exposure to at least one androgen receptor pathway inhibitor (ARPI) and taxane-based chemotherapy at any time in the course of their disease. The dose escalation phase will follow an i3+3 design, with each cohort able to backfill up to 20 participants for further characterization of the safety, tolerability, and preliminary efficacy of dose and schedules.
The expansion phase (Phase 2a) aims to assess the efficacy, safety, and tolerability of [212Pb]Pb-ADVC001 at the recommended Phase 2 dose in three groups of participants with PSMA-positive mCRPC:
- Group 1: Participants who have had exposure to at least one ARPI and have not received a taxane for the treatment of mCRPC
- Group 2: Participants who have had exposure to at least one ARPI and received taxane-based chemotherapy for the treatment of mCRPC
- Group 3: Participants who have had exposure to 177Lu-PSMA
If data from Phase 1b demonstrates multiple dosing regimens are reasonably equivalent in terms of safety, tolerability and anti-tumor activity, the Phase 2a expansion study may include adaptive randomization to identify an optimized dose and schedule. The trial is currently enrolling at two clinical sites in Australia.2
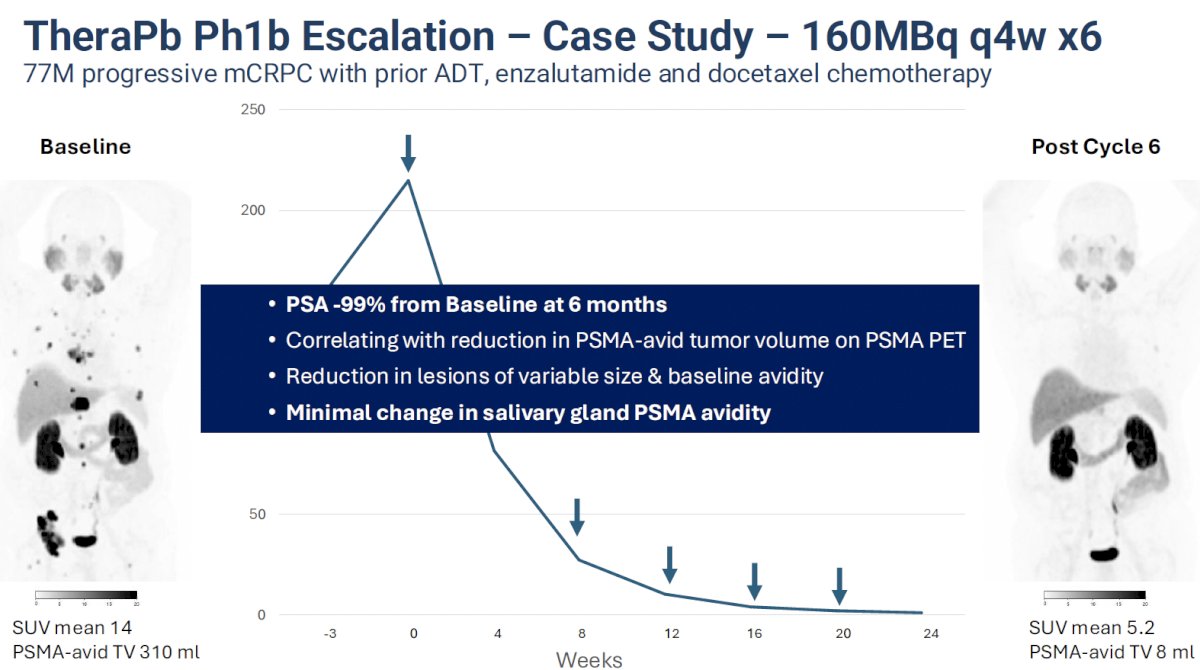
Dr. Pattison presented a case study of a 77-year-old male with progressive mCRPC who had disease progression following prior therapy with ADT, enzalutamide, and docetaxel. In the phase 1b escalation portion of the trial, he received a dose of 160 MBq every 4 weeks x 6 cycles. His PSA dropped by 99% from baseline to 6 months, and this was correlated with a reduction in PSMA-avid tumor volume on his interval PSMA PET scan. There was a reduction in lesions of variable size and baseline avidity. Notably, there was minimal change in salivary gland PSMA avidity.
In 2023, the first human 212Pb SPECT/CT images were published. They were acquired after administration of 60 MBq of 212Pb-ADVC001 to a 73-year-old mCRPC patient. Imaging was performed at 1.5, 5, 20, and 28 hours after infusion. Two simultaneous triple-energy window acquisitions were obtained using a Siemens Intevo Bold (high-energy collimators at 30 s per view for 120 views per rotation at 2 bed positions with noncircular orbits; total time, 60 min). Each energy window was reconstructed independently, and the resulting images were summed with removal of Compton-based orbit artifacts.
Representative 212Pb SPECT/CT images showed rapid tumor uptake of 212Pb-ADVC001, highly concordant with tumor burden delineated on the pretreatment 18F-DCFPyl PET/CT images. Images acquired after 20 hours showed persistent tumor uptake despite low counts due to 212Pb decay.3

What is the radiation safety profile of 212Pb?
- Patient dose rates:
- Comparable to Lu-177 PSMA
- Less than I-131 NaI ablation
- Approximately 50% is rapidly cleared (Tbio= 2 hours)
- Short Tphys: 10.6 hours
- Staff exposure:
- Mirion DMC3000 EPDs
- 5 – 15μSv per 200MBq cycle for NMTs
- Comparable to a day in PET dept
- Public exposure
- Discharge at 3 hours with dose rate <25μSv
- Discharge advice
- Up to 3 days increased hygiene
- Up to 2 days close contact restrictions
- Results in <100mSv to any family member
What are the molecular mechanisms triggered by 212Pb-PSMA in prostate cancer cells?
- Targeted cell death: The radiopharmaceutical binds receptors on cancer cells and releases α particles, resulting in double-stranded DNA breaks, cell membrane and organelle disruption in bound cell and neighboring cells
- Bystander effect: Dying cancer cells release damage-associated molecular patterns (DAMPs), causing nearby cells to die as well
- Immune activation: Dying cancer cells release neoantigens, which are taken up by antigen-presenting cells (APCs). APCs activate T cells, which further attack cancer cells and can convert into memory T cells, providing durable and widespread systemic response.

Dr. Pattison’s take home messages were as follows:
- The physical characteristics of 212Pb are highly favorable for radioligand therapy
- The ability to image 212Pb and derive biodistribution and dosimetry is beneficial
- There is encouraging 212Pb-SSTR2 safety data and anti-tumor activity to date
- There is emerging clinical data with PSMA and other targets
- The TheraPb phase 1b mCRPC data will be presented later this year
- The staff dose and patient discharge is favorable and manageable in a routine clinical setting
- The immunogenic profile of 212Pb is being investigated and may be favorable for combination therapies
- Solutions for scaled production are in development by several companies to supply large trials and commercial indications
Presented by: David A. Pattison, MBBS, MPH, FRACP, Royal Brisbane & Women's Hospital, Brisbane, Australia.
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Meeting, New Orleans, LA, June 21st – 24th, 2025
References:
- Strosberg J, El-Haddad G, Wolin E, et al. Phase 3 trial of 177Lu-Dotatate for midgut neuroendocrine tumors. N Engl J Med. 2017;376(2):125–35.
- Zhou C, Sartor O, Gulley JL, et al. Phase Ib/IIa dose escalation and expansion study of [²¹²Pb]Pb-ADVC001 in metastatic castration-resistant prostate cancer: TheraPb–phase I/II study. J Clin Oncol. 2024;42(16_suppl):TPS193.
- Kratochwil C, Schlenkhoff C, Schirbel A, et al. First-in-human 212Pb-PSMA–targeted α-therapy SPECT/CT imaging in a patient with metastatic castration-resistant prostate cancer. J Nucl Med. 2023;64(1):100–2.