(UroToday.com) At the 2021 Society of Nuclear Medicine & Molecular Imaging (SNMMI) Meeting’s Correlative Cross-Sectional and Molecular Imaging session, Dr. Michael Blake discussed CT and MRI appearances of adrenal lesions. The adrenal glands play a critical role in physiology and endocrinology, as well as being critical in oncologic staging. However, there is an increasing dilemma of increasing detection of adrenal ‘incidentalomas’ – non-specific adrenal nodules. The normal anatomy of the adrenal glands includes bilateral, pyramid-shaped caps that sit above the kidneys, and comprising an adrenal body and two limbs.
The incidence of adrenal adenomas is estimated at <2% in younger patients and up to 8% in older adults. They are generally small, well-defined, and homogenous masses of low attenuation. Adenomas may show unusual features such as calcification, hemorrhage or necrosis:

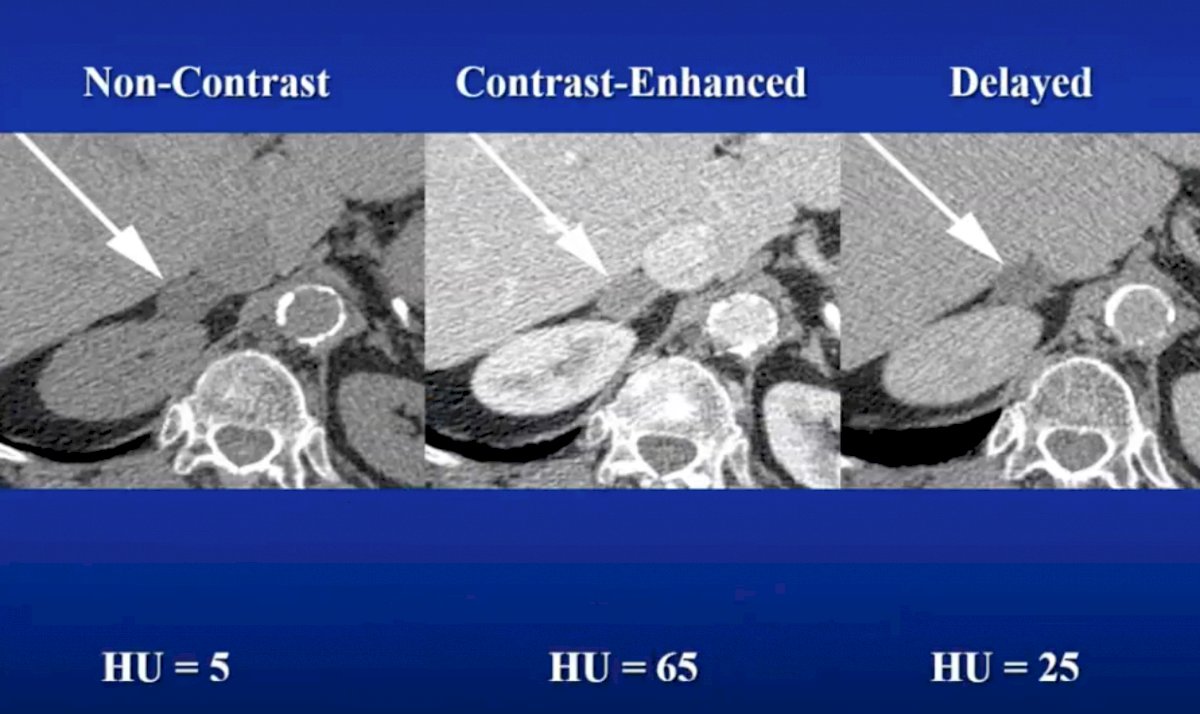
On non-contrast CT imaging, the intracytoplasmic lipid component is important in making the correct diagnosis. An attenuation of < 0 Hounsfield units on unenhanced CT has a specificity of 100% and a sensitivity of 47%. A widely accepted clinically appropriate threshold for an adenoma diagnosis is <10 Hounsfield units, which provides specificity of 96% and encompasses 71% of benign masses.1 Although the 10 Hounsfield unit criteria have been generally accepted, the lower specificity should be gauged with caution and masses in the 2-10 Hounsfield unit range deserve special scrutiny for other characteristics such as homogeneity: irregular borders should be viewed with particular suspicion in any mass (ie. adrenocortical carcinoma, metastases from clear cell RCC). Additionally, an issue is that 30% of adenomas are lipid poor and cannot be characterized on non-contrast CT imaging. Contrast-enhanced CT washout is one method for further characterizing adrenal lesions, specifically the absolute percent washout (APW) and the relative percent washout (RPW):

As follows are the characteristics of a low-density adenoma on CT scan:
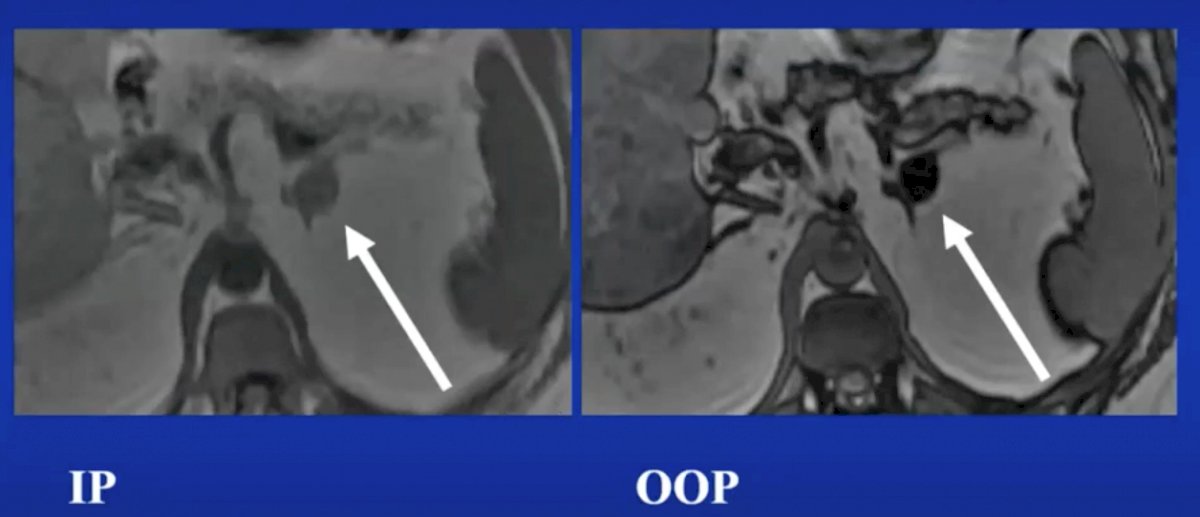
MRI can also be useful in delineating characteristics of adrenal adenomas, utilizing an overlap of T1 and T2 intensities. Washout is not routinely used, but is technically feasible, however chemical shift is more often utilized in that lipid protons resonate at slower frequency than water, so that the spins go in and out of phase over time. The theory behind compressed-sensing MRI is that lipid and water protons process at different frequencies in a given magnetic field, and the signal from these protons can either be additive or subtractive, depending on the time to echo chosen. Compressed-sensing MRI uses the decrease in signal on out-of-phase images to identify intracellular lipid. It has been demonstrated that qualitative evaluation of this drop-off on the MR image is sufficient to diagnose a lipid rich adenoma, but certain experts prefer to use a quantitative method to demonstrate the fractional signal drop-off from the in-phase to the out-of-phase image. A signal drop-off of 16.5% is generally considered to indicate a lipid-rich adenoma. An important caveat is that adrenal cortical carcinoma, pheochromocytoma, and clear cell renal cell carcinoma metastasis can all sometimes show signal loss on out-of-phase images. Compressed-sensing MRI can characterize some additional adenomas when CT imaging is in the indeterminate range of 10-20 Hounsfield units.
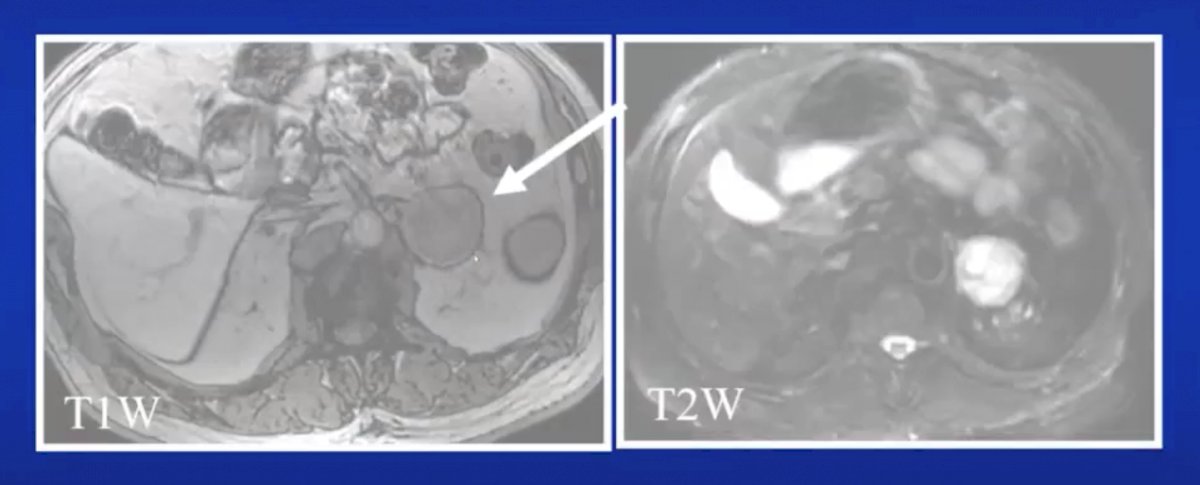
Pheochromocytomas historically made up 10% of adrenal masses, however, Dr. Blake notes that this rule no longer holds true as they are typically more common in situations where there are multiple and bilateral adrenal masses, as well as in situations where there is a familial syndrome (ie. MEN, neurofibromatosis, von Hippel Lindau disease). Pheochromocytomas can be multifocal and/or coexist with paragangliomas in 30-70% of cases, and are bilateral in 20-40% of cases. The most impressive results to date for diagnosing pheochromocytomas have been with 6-[18F] fluorodopamine PET scanning and carbon 11 hydroxyephedrine PET scanning. Interestingly, the incidence of pheochromocytoma in the hypertensive population is 0.1% to 0.6% and the incidence in the general population is 0.05%. A Hounsfield unit cutoff of 130 is used to identify pheochromocytoma, with a sensitivity of 38% and specificity of 100%. It is more important to have high sensitivity for pheochromocytomas, since this is a diagnosis clinicians do not want to miss. As such, it is reasonable to suggest biochemical testing for nodules with venous phase enhancement of >85 Hounsfield units, given that they are more likely to be pheochromocytomas than adenomas. Dr. Blake suggests that 1/3-2/3 of pheochromocytomas mimic adenoma washout. Additionally, pathologists cannot tell if a pheochromocytoma is malignant until metastasis declares itself, but Dr. Blake notes that all pheochromocytomas are surgical lesions due to their systemic effect on the circulation. As follows is a typical pheochromocytoma on T1W/T2W MRI:
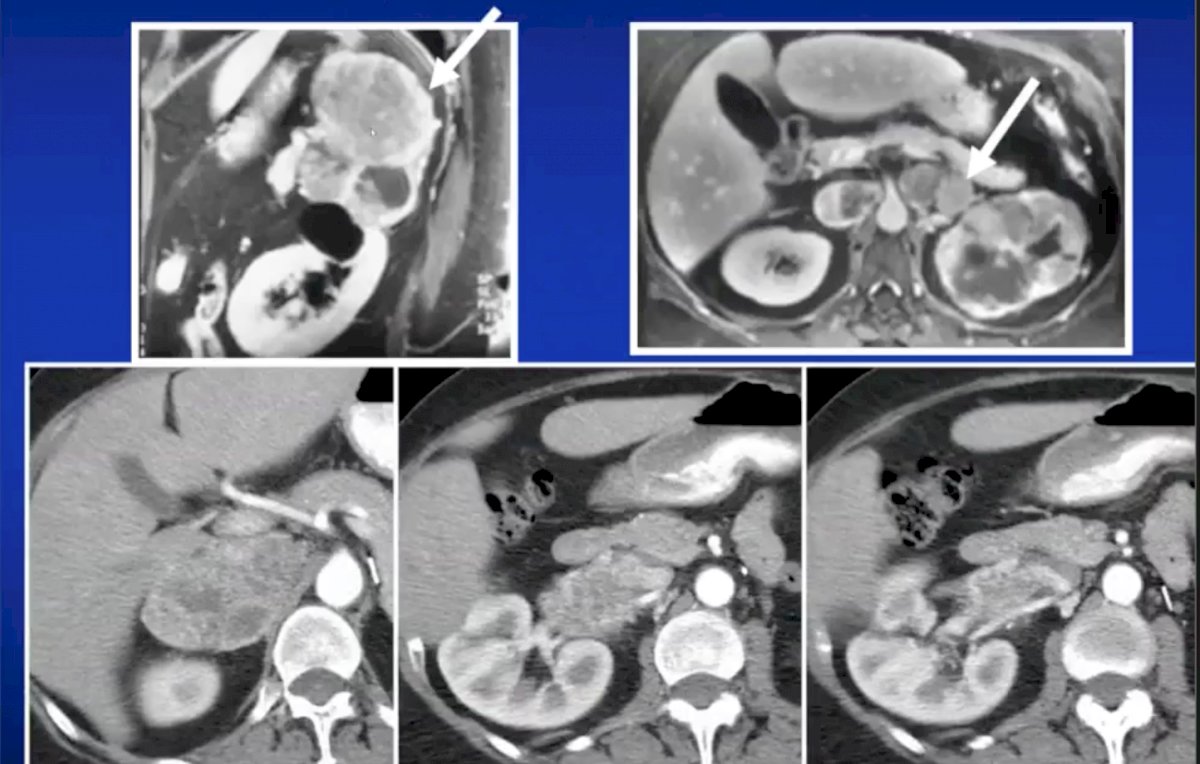
Given the nonfunctional behavior of many paragangliomas, autopsy series suggest that the prevalence may be higher than reported owing to underdiagnosis. Most paragangliomas are diagnosed in the third to fifth decades with a mean age of 47 years, and are often associated with MEN2A and MEN 2B syndrome, neurofibromatosis, hereditary paraganglioma-pheochromocytoma syndrome, and von Hippel Lindau disease. In these patients with a genetic predisposition to develop paragangliomas and pheochromocytomas, the mean age of diagnosis is younger than those diagnosed with sporadic paragangliomas. These tumors may arise from either the sympathetic or parasympathetic paraganglia in the head, neck, skull base, adrenal gland, or along the abdominopelvic sympathetic chain. These lesions may be nonsecretory or secrete catecholamines, and they are classified by the World Health Organization by anatomic site of origin, regardless of secretory status. The majority of paragangliomas are nonsecretory and are either incidentally discovered or produce symptoms secondary to local mass effect, particularly in the head, neck and skull base. Approximately 26% of paragangliomas are multiple, 15-20% are extra-adrenal, and 33-50% are associated with a hereditary syndrome. On CT imaging, paragangliomas demonstrate avid contrast enhancement with variable washout, whereas on MRI there is T1 hypointensity and may have high signal on T2 weighted imaging. Furthermore, on MRI these lesions may also demonstrate salt and pepper appearance, with pepper representing multiple areas of signal void of vessels and salt representing hyperintense foci due to slow-flow or hemorrhage. As follows is the salt-and-pepper appearance of paragangliomas on MRI:

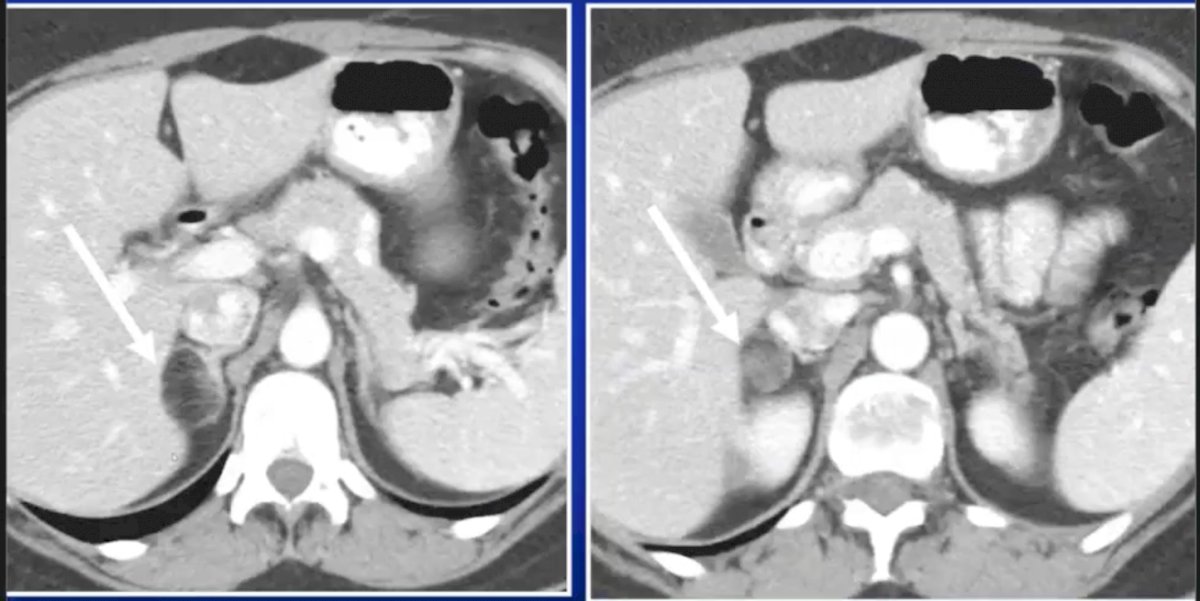
Adrenocortical carcinoma is typically characterized by an irregular shape, heterogeneous, and >4 cm in size. There also may be unilateral invasion, local metastases, calcification, and central areas of necrosis. On MRI, most T1 areas are hypointense and T2 areas are hyperintense. The following are representative images of adrenocortical carcinoma on CT:
Malignancies commonly metastasize to the adrenal gland, which most commonly includes metastases from the lung, breast, melanoma, kidney, hepatocellular carcinoma, esophageal, stomach, and colon. However, even in patients with known malignancies, almost half of the adrenal incidentalomas are benign adenomas.
Myelolipomas are easily characterized on CT or MRI secondary to their abundance of mature fat. The amount of recognizable macroscopic fat varies from almost 100% to none, however the detection of even the slightest macroscopic fat indicates that the lesion is a myelolipoma. Additionally, calcification can be present in ~20% of cases, and occasionally these lesions can be quite large (>5 cm) in which the myeloid elements of the lesion have a tendency to hemorrhage. Larger lesions may exert a mass effect on adjacent organs, and it may be difficult to ascertain myelolipomas from well-differentiated retroperitoneal liposarcoma (which typically engulf or displace the adrenal gland).
Other adrenal lesions include: cysts/pseudocysts, lymphoma, hemangiomas, ganglioneuromas, collision tumors, and pseudoadrenal masses such as gastric diverticulum, bowel, tortuous renal or splenic arteries, and/or pancreatic, splenic, renal or hepatic masses.
Dr. Blake concluded his presentation with the following take-home messages:
- CT and MRI can help characterize many adrenal lesions, including pheochromocytomas and paragangliomas
- CT and MRI are complementary to nuclear medicine imaging techniques
- For adenomas, non-contrast CT is <10 Hounsfield units, >40% RPW >60% APW at 15 minutes, and signal drop on out of phase imaging on MRI
- For pheochromocytomas and paragangliomas, these may be bright on T2 imaging on MRI and often hypervascular
Presented by: Michael Blake, MD, Associate Professor of Radiology, Massachusetts General Hospital, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the Society of Nuclear Medicine & Molecular Imaging – 2021 Virtual Meeting, June 11-15, 2021
References:
- Schieda N, Al Dandan O, Kielar AZ, et al. Pitfalls of adrenal imaging with chemical shift MRI. Clin Radiol. 2014;69:1186-1197.