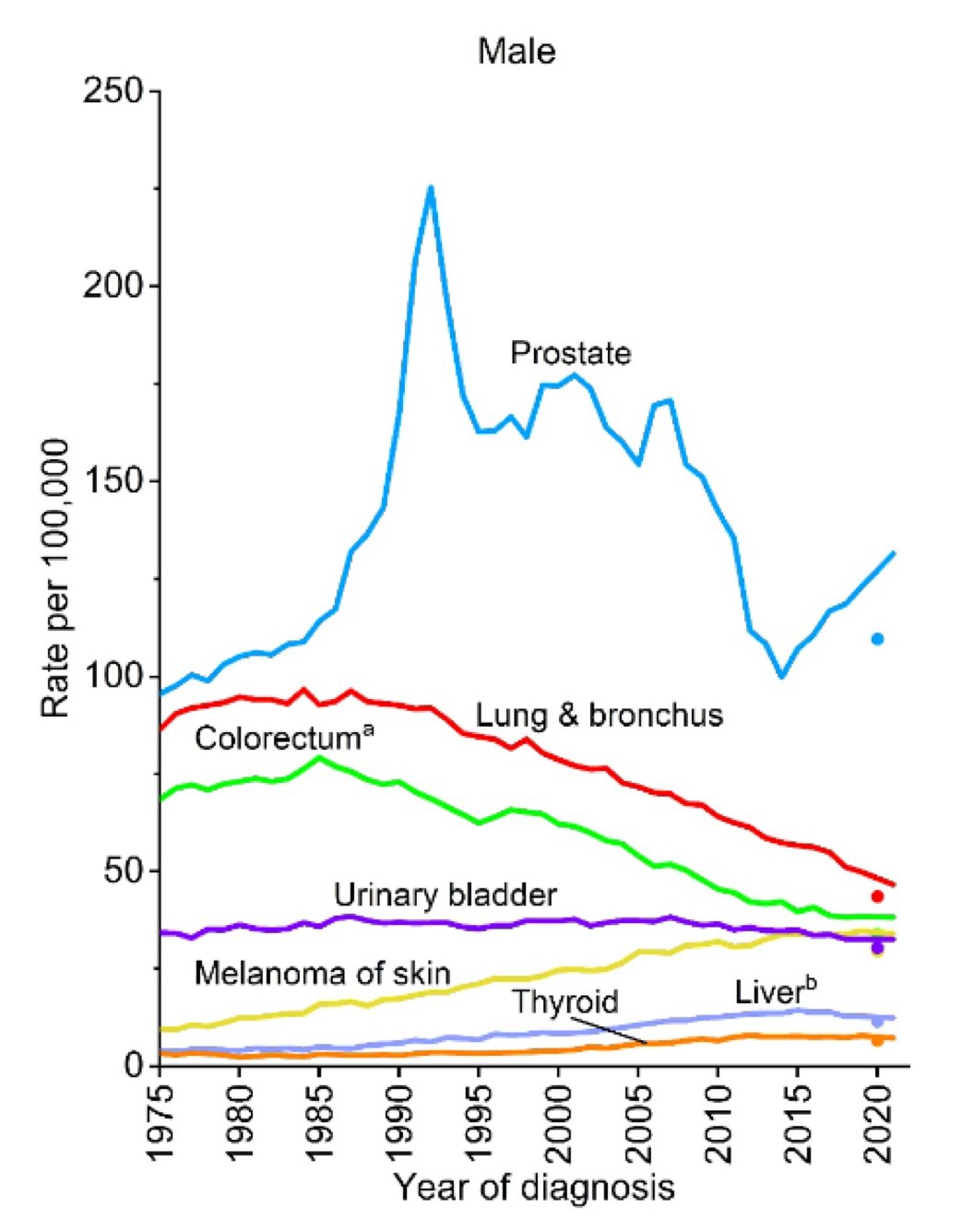
(UroToday.com) The 2026 SESAUA annual meeting featured a State of the Art Lecture by Dr. Sanoj Punnen discussing pathways for prostate cancer evaluation, including guidelines, tools, and best practices to optimize PSA based screening. Currently, prostate cancer is the most commonly diagnosed non-skin cancer among males in the United States, with an estimated 313,780 new cases this year. In terms of mortality, prostate cancer represents the second most lethal cancer among men, with an estimated 35,770 deaths this year, second only to lung and bronchus cancer (n = 64,190).
Since 1987, PSA testing has been a key tool for prostate cancer screening. However, secondary to issues around recommendations for prostate cancer screening, there has been an uptick in prostate cancer diagnoses since ~2015:
Dr. Punnen notes that based on the summation of the European Randomized Screening for Prostate Cancer trial data, the benefits of prostate cancer screening increase with time:
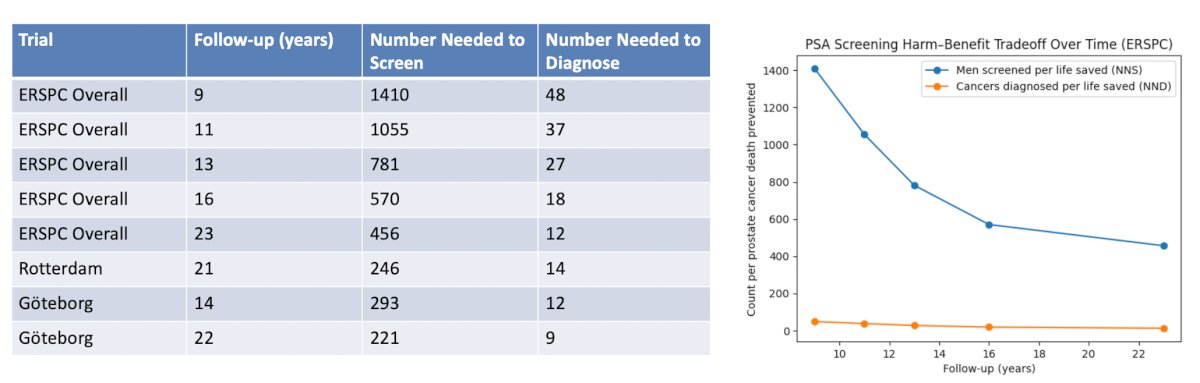
In the Rotterdam section of the European Randomized Study of Screening for Prostate Cancer, de Vos et al.1 found that the relative risk of prostate cancer-specific mortality was 0.73 (95% CI 0.61-0.88), favoring screening. For metastatic prostate cancer, the relative risk was 0.67 (95% CI 0.58-0.78), favoring screening, with a number needed to investigate and number needed to diagnose to prevent one metastasis of 121 and 7, respectively:
![In the Rotterdam section of the European Randomized Study of Screening for Prostate Cancer, de Vos et al. [1] found that the relative risk of prostate cancer-specific mortality was 0.73 (95% CI 0.61-0.88), favoring screening. For metastatic prostate cancer, the relative risk was 0.67 (95% CI 0.58-0.78), favoring screening, with a number needed to investigate and number needed to diagnose to prevent one metastasis of 121 and 7, respectively:](/images/com-doc-importer/257-ses-aua-2026/ses-aua-2026-pathways-for-prostate-cancer-evaluation-guidelines-tools-and-best-practices-to-optimize-psa-based-screening/image-2.jpg)
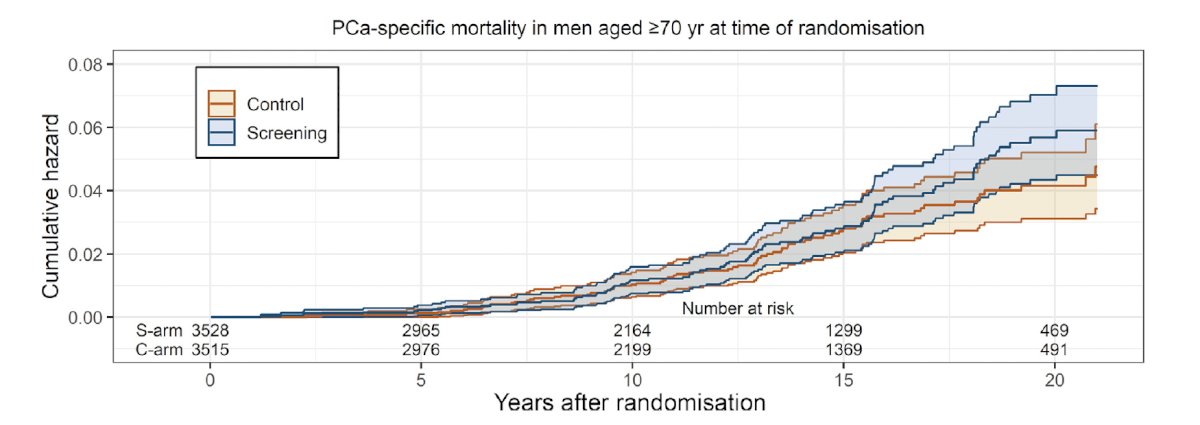
There was no statistical difference in prostate cancer-specific mortality (relative risk of 1.18, 95% CI 0.87-1.62) observed in men aged ≥70 years at the time of randomization:
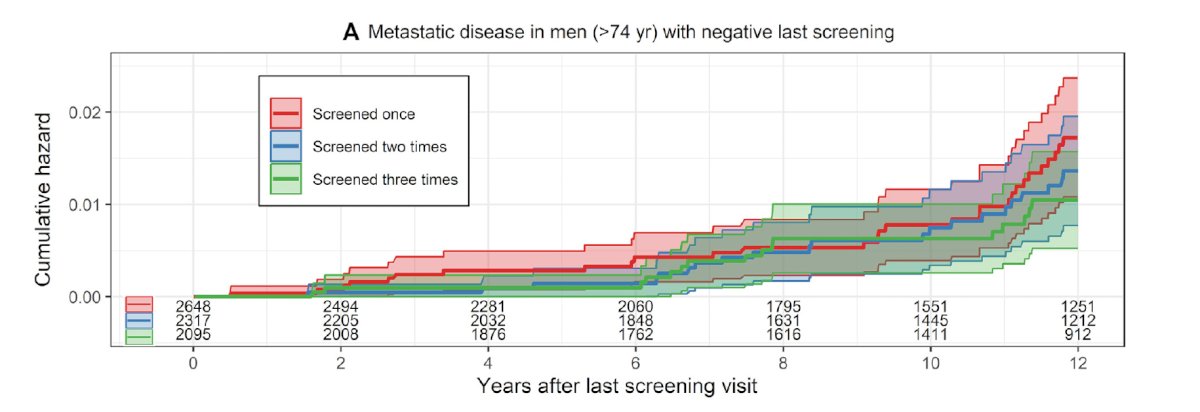
In the screening arm, higher rates of prostate cancer-specific mortality and metastatic disease were observed in men who were screened only once and in a selected group of men above the screening age cut-off of 74 years:
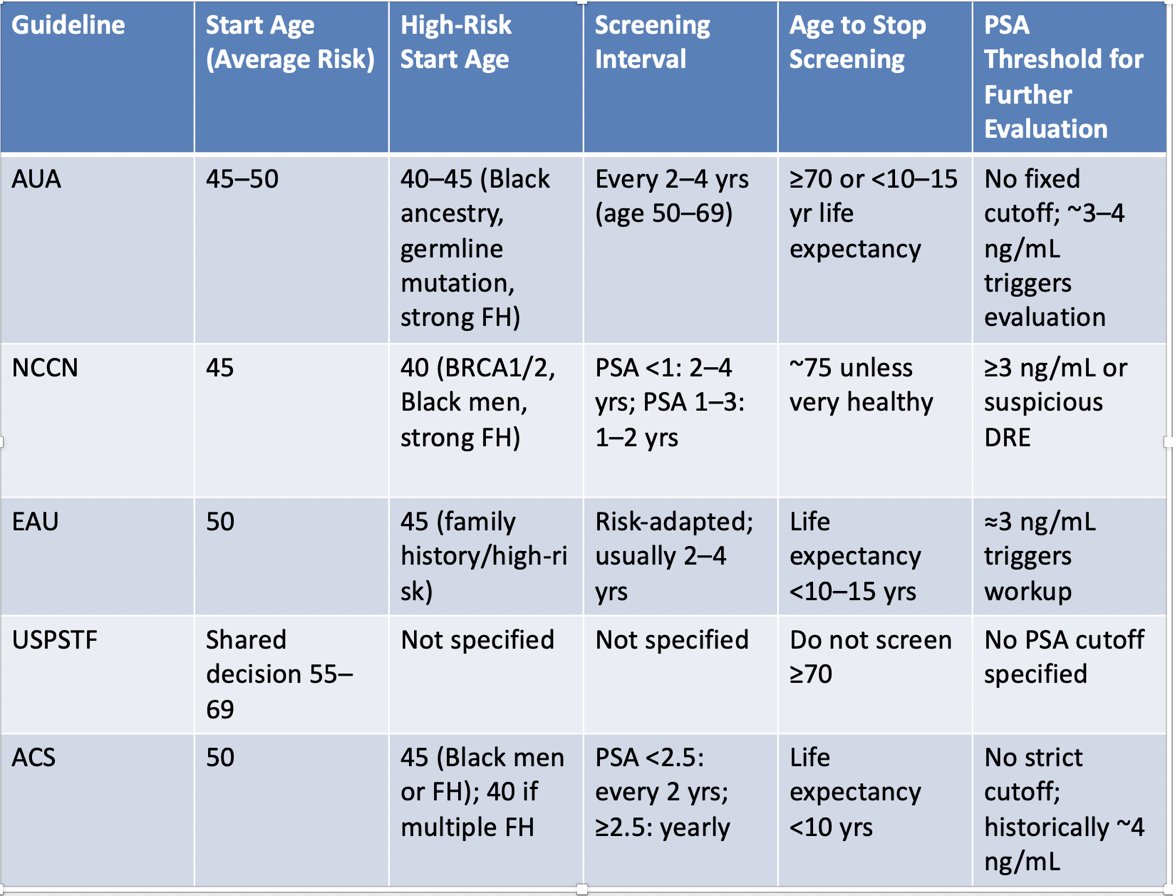
Based on the available prostate cancer screening guidelines, the recommendation is to start screening at age 45-50 years, to screening every 2-4 years if the PSA is < 1 ng/mL, to screen every 1-2 years if the PSA is > 1 ng/mL, to proceed with intervention if the PSA is 3-4 ng/mL, and to stop screening at age 70-75 years of age if the life expectancy is less than 10 years:
Several groups and guideline committees have published detailed algorithms regarding PSA testing. In 2025, Ashraf and colleagues2 proposed the following clinical workflow for PSA testing for primary care physicians and appropriate urology referral in an era of conflicting guideline recommendations and debate:
![Several groups and guideline committees have published detailed algorithms regarding PSA testing. In 2025, Ashraf and colleagues [2] proposed the following clinical workflow for PSA testing for primary care physicians and appropriate urology referral in an era of conflicting guideline recommendations and debate:](/images/com-doc-importer/257-ses-aua-2026/ses-aua-2026-pathways-for-prostate-cancer-evaluation-guidelines-tools-and-best-practices-to-optimize-psa-based-screening/image-6.jpg)
Dr. Punnen also highlighted the AUA’s guidelines for prostate cancer screening algorithm:
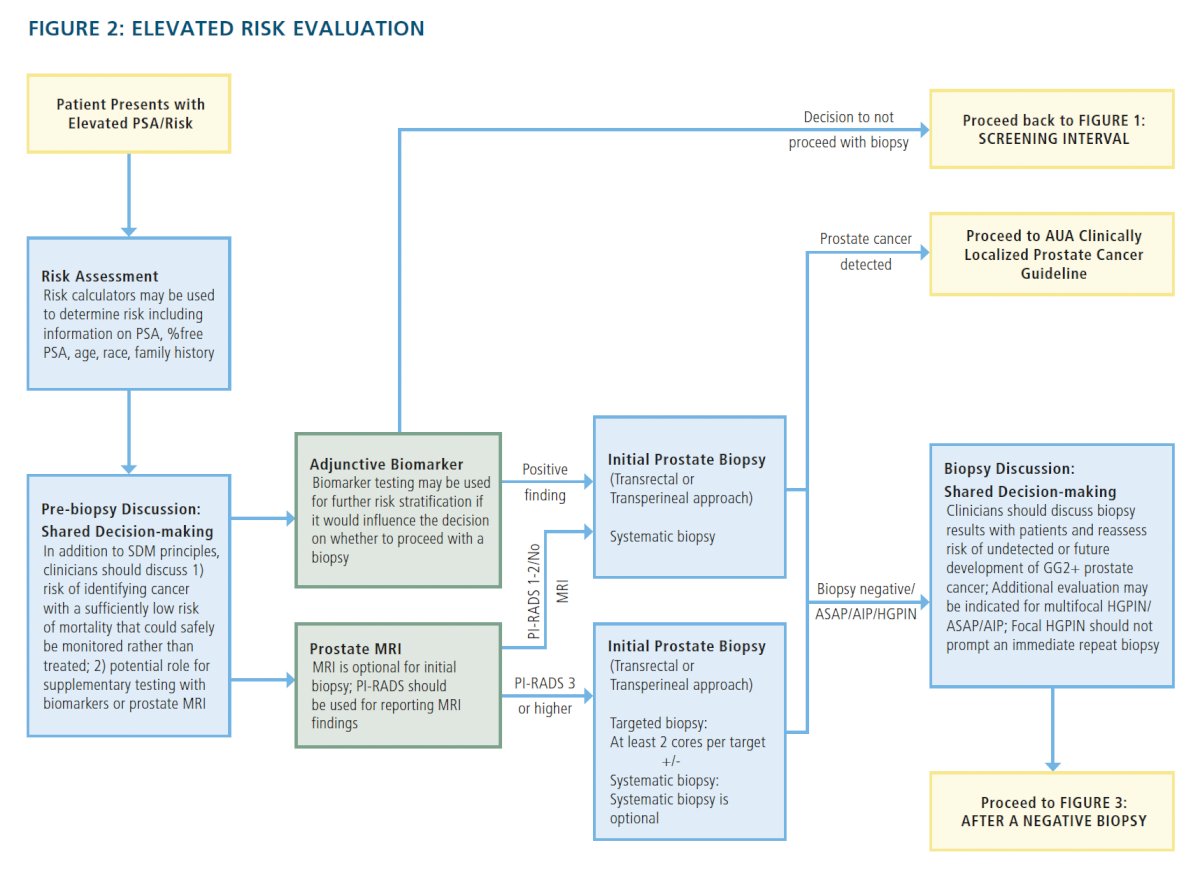
What is the role of prostate MRI in the setting of prostate cancer screening? Based on the work from the NCI,3 STHLM3,4 and PRECISION,5 Dr. Punnen notes that a prostate mpMRI:
- Reduces the number of biopsies
- Allows for better detection of clinically significant prostate cancer
- Detects less indolent prostate cancer
In 2020, Sathianathen et al.6 performed a systematic review and meta-analysis of the available literature to update the negative predictive value of mpMRI for clinically significant prostate cancer. Among 42 studies with 7321 patients, the negative predictive value was assessed at 90-93%, which translates to 7-10% of men (depending on the setting) having missed clinically significant prostate cancer with a negative mpMRI if they do not proceed with a prostate biopsy. Next, Dr. Punnen discussed the PROMIS study,7 which demonstrated that MRI outperformed systematic biopsy with an increased sensitivity (93%) and negative predictive value (89%), with the possibility for biopsy avoidance in 27% of cases (negative MRI):

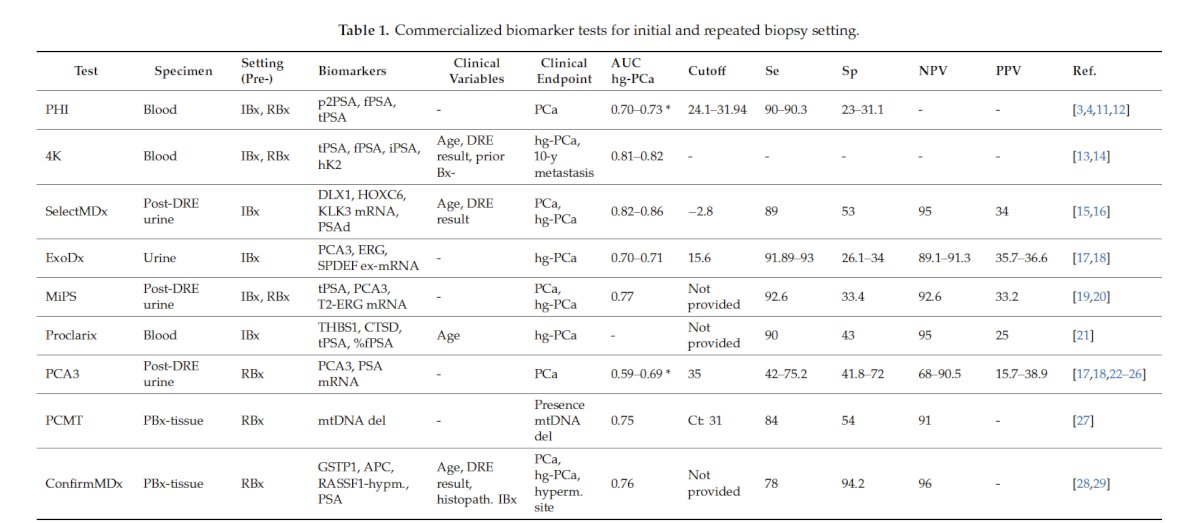
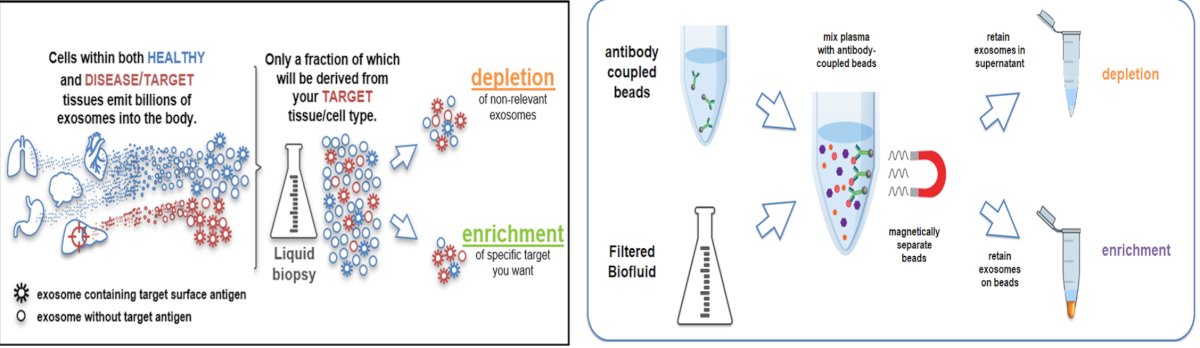
Dr. Punnen also discussed the role of biomarkers for prostate cancer evaluation, highlighting the following table of commercially available tests in the initial and repeat biopsy setting:
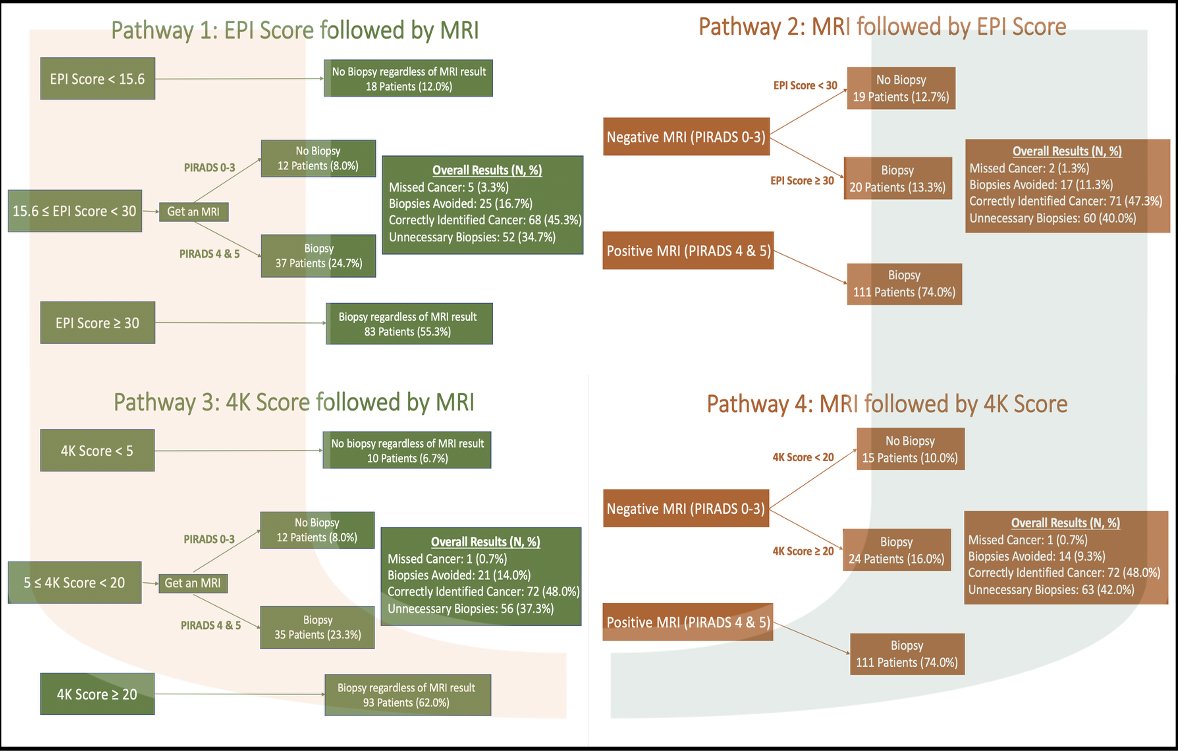
At the University of Miami Miller School of Medicine, Dr. Punnen is the principal investigator of the Marker-Driven Selection of patients for prostate biopsy and management: The University of Miami MDSelect Protocol. This protocol is based on four distinct pathways:
- Pathway 1: EPI score followed by MRI
- Pathway 2: MRI followed by EPI score
- Pathway 3: 4K score followed by MRI
- Pathway 4: MRI followed by 4K score
In 2024, Auvinen and colleagues8 published the results of the ProScreen randomized trial, which sought to assess the rates of Grade Group 1 and Grade Groups 2-5 prostate cancer identified among men invited to participate in a prostate cancer screening protocol consisting of a PSA test, a 4-kallikrein panel, and an MRI scan. Among 60,745 eligible men, 15,201 were randomized to be invited, and 45,544 were randomized not to be invited for PSA screening:
For the 7,744 men who were invited and participated, 32 Grade Group 1 prostate cancers were diagnosed (cumulative incidence: 0.41%), and 128 Grade Group 2-5 prostate cancers were diagnosed (cumulative incidence: 1.65%). During a median follow-up of 3.2 years, in the group not invited to undergo screening, 65 Grade Group 1 prostate cancers (cumulative incidence: 0.14%) and 282 Grade Group 2-5 prostate cancers (cumulative incidence: 0.62%) were detected. The risk difference for the entire group randomized to the screening invitation versus the control group was 0.11% (95% CI, 0.03%-0.20%) for Grade Group 1 and 0.51% (95% CI, 0.33%-0.70%) for Grade Group 2-5 prostate cancer:
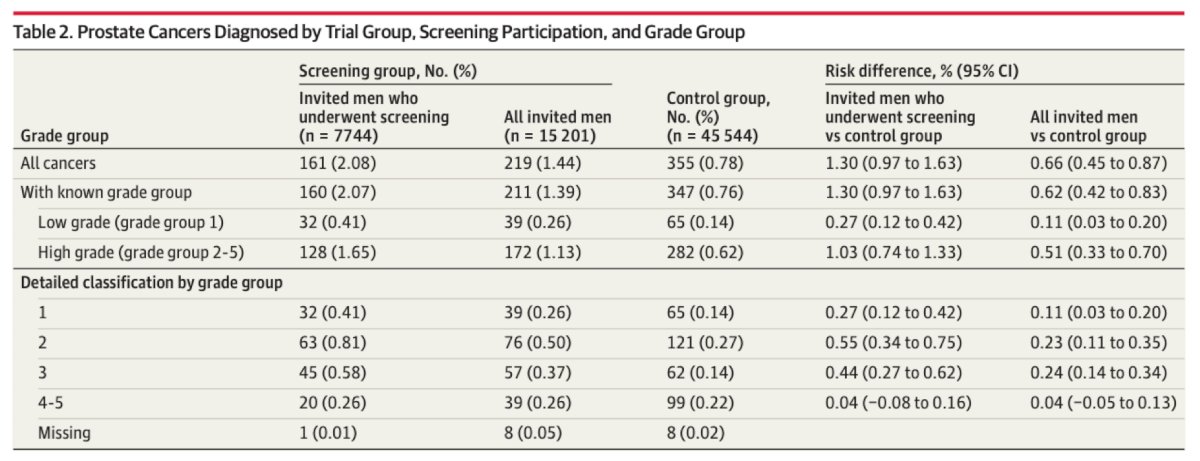
From the initial results of ProScreen, 1 additional Grade Group 2-5 prostate cancer per 196 men, and 1 Grade Group 1 prostate cancer per 909 men were detected among those randomized to a single prostate cancer screen versus those who were not invited to undergo screening.
Importantly, men from underrepresented communities have a higher risk of prostate cancer incidence and mortality, as well as lower rates of screening. As such, at the University of Miami, Dr. Punnen and colleagues have initiated targeted prostate cancer screening among underrepresented communities through the GameChanger mobile screening initiative. This platform utilizes geo-spatial mapping to identify areas of risk and uses GameChanger infrastructure and partners to offer community-based cancer screening. The impact of this initiative is:
- There have been 1,000 men from underrepresented, diverse communities around the Sylvester Comprehensive Cancer Center who have been screened
- Approximately 10% have been enrolled in a research protocol
- This is 1 of 3 mobile prostate cancer screening vehicles in the world
- This was awarded the Research Scholar Award from the American Cancer Society

Finally, Dr. Punnen noted several future directions. The first is the use of artificial intelligence for prostate MRI:

Second, is enhancing prostate cancer biomarkers, for which Dr. Punnen is the principal investigator of a prospective study:
Third, the use of PSMA PET/CT for prostate cancer diagnosis. The PRIMARY multicenter study assessed the additive diagnostic value of PSMA PET/CT to mpMRI in the diagnosis of prostate cancer.9 In this study, there were 296 men enrolled with suspected prostate cancer, with no prior biopsy or MRI, recent MRI (6 months), and planned transperineal biopsy based on clinical risk and MRI. Among 291 patients, combined PSMA PET + MRI improved the negative predictive value compared with MRI alone (91% versus 72%, test ratio 1.27 [1.11-1.39], p < 0.001). Sensitivity also improved (97% versus 83%, p < 0.001), and specificity was reduced (40% versus 53%, p = 0.011). Of all men, 19% were PSMA PET + MRI negative (38% of PI-RADS 2/3) and could potentially have avoided biopsy, risking delayed clinically significant prostate cancer detection in 3.1% men with clinically significant prostate cancer (5/162) or 1.7% (5/291) overall. The BI-PASS trial is also assessing the ability of PSMA PET/CT to reduce the number of unnecessary biopsies without missing clinically significant prostate cancer:
![Third, the use of PSMA PET/CT for prostate cancer diagnosis. The PRIMARY multicenter study assessed the additive diagnostic value of PSMA PET/CT to mpMRI in the diagnosis of prostate cancer.9 In this study, there were 296 men enrolled with suspected prostate cancer, with no prior biopsy or MRI, recent MRI (6 months), and planned transperineal biopsy based on clinical risk and MRI. Among 291 patients, combined PSMA PET + MRI improved the negative predictive value compared with MRI alone (91% versus 72%, test ratio 1.27 [1.11-1.39], p < 0.001). Sensitivity also improved (97% versus 83%, p < 0.001), and specificity was reduced (40% versus 53%, p = 0.011). Of all men, 19% were PSMA PET + MRI negative (38% of PI-RADS 2/3) and could potentially have avoided biopsy, risking delayed clinically significant prostate cancer detection in 3.1% men with clinically significant prostate cancer (5/162) or 1.7% (5/291) overall. The BI-PASS trial is also assessing the ability of PSMA PET/CT to reduce the number of unnecessary biopsies without missing clinically significant prostate cancer:](/images/com-doc-importer/257-ses-aua-2026/ses-aua-2026-pathways-for-prostate-cancer-evaluation-guidelines-tools-and-best-practices-to-optimize-psa-based-screening/image-16.jpg)
Dr. Punnen concluded his presentation discussing pathways for prostate cancer evaluation, including guidelines, tools, and best practices to optimize PSA based screening, with the following take-home points:
- Prostate cancer screening with PSA reduces prostate cancer mortality, and the benefit increases with time
- MRI and biomarkers improve the selection of patients for biopsy, but utilization is variable
- Artificial intelligence, reduced cost of sequencing, and next-generation imaging will enhance prostate cancer evaluation, but at what cost?
Presented by: Sanoj Punnen, MD, Sylvester Comprehensive Cancer Center, University of Miami, Miami, FL
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Southeastern Section of the American Urological Association (SESAUA) Annual Meeting, San Juan, PR, Wed, Mar 18 – Sat, Mar 21, 2026.
References:
- de Vos II, Meertens A, Hogenhout R, et al. A detailed evaluation of the effect of prostate-specific antigen-based screening on morbidity and mortality of prostate cancer: 21-year follow-up results of the Rotterdam Section of the European Randomized study of screening for prostate cancer. Eur Urol. 2023 Oct;84(4):426-434.
- Ashraf M, Choudry M, Frendl D, et al. An evidence-based review and common-sense approach to prostate cancer screening for primary care physicians, in an era of conflicting guidelines, recommendations, and debate. J Prim Care Community Health. 2025 Jan-Dec: 16:21501319251401393.
- Ahdoot M, Wilbur AR, Reese SE, et al. MRI-Targeted, Systematic, and Combined Biopsy for Prostate Cancer Diagnosis. N Engl J Med. 2020 Mar 5;382(10):917-928.
- Eklund M, Jaderling F, Discacciati, et al. MRI-targeted or standard biopsy in prostate cancer. N Engl J Med. 2021 Sep 2;385(10)908-920.
- Kasivisvanathan V, Rannikko AS, Borghi M, et al. MRI-targeted or standard biopsy for prostate cancer diagnosis. N Engl J Med 2018;378(19):1767-1777.
- Sathianathen NJ, Omer A, Harriss E, et al. Negative predictive value of multiparametric magnetic resonance imaging in the detection of clinically significant prostate cancer in the Prostate Imaging Reporting and Data System Era: A systematic review and meta-analysis. Eur Urol. 2020 Set;78(3):402-414.
- Ahmed HU, El-Shater Bosaily A, Brown LC, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017;389(10071):815-822.
- Auvinen A, Tammela TLJ, Mirtti T, et al. Prostate Cancer Screening with PSA, Kallikrein Panel, and MRI: The ProScreen Randomized Trial. JAMA 2024 May 7;331(17):1452-1459.
- Emmett L, Butaeu J, Papa N, et al. The Additive Diagnostic Value of Prostate-specific Membrane Antigen Positron Emission Tomography Computed Tomography to Multiparametric Magnetic Resonance Imaging Triage in the Diagnosis of Prostate Cancer (PRIMARY): A Prospective Multicentre Study. Eur Urol. 2021 Dec;80(6):682-689.