(UroToday.com) The 2026 SESAUA annual meeting featured a bladder cancer session and presentation by Dr. Joon Kyung Kim discussing differences in restaging TURBT pathology outcomes based on index TURBT performed by an SUO fellowship trained or non-SUO trained urologist. TURBT has both diagnostic and therapeutic implications. For individuals diagnosed with T1 non muscle invasive bladder cancer, guidelines recommend restaging TURBT, given that up to 50% of individuals may have residual tumor and 20% may be understaged on repeat resection. Patients without residual T1 disease on restaging TURBT have decreased risk of recurrence and progression, and restaging TURBT can also reduce the risk of recurrence and progression compared to not performing a restaging TURBT at all.
TURBT may be associated with considerable morbidity, with 30 day complication rates ranging from 5%-43%, which include bleeding, UTIs, and bladder perforation. TURBT is also associated with a significant cost burden to the healthcare system, from the restaging TURBT itself, and moreover, if a complication occurs: $3,900 for a TURBT, with an increase to $7,300 for a complication. Given that index TURBT quality may also differ by surgeon experience, this study investigates restaging TURBT outcomes of patients with T1 non muscle invasive bladder cancer who underwent index TURBT with a Society of Urologic Oncology (SUO) fellowship trained urologist versus a non-SUO trained urologist.
This was a retrospective review of all patients who underwent restaging TURBT at a single institution between July 2021 and July 2024 after T1 non muscle invasive bladder cancer diagnosis on index TURBT. Completion of resection was assessed by the operative report. Presence of muscularis propria and stage on index and restaging specimens were assessed by reviewing pathology reports, and all outside index TURBT pathology specimens were internally reviewed. Recurrence free survival at first surveillance cystoscopy was assessed as an outcome.
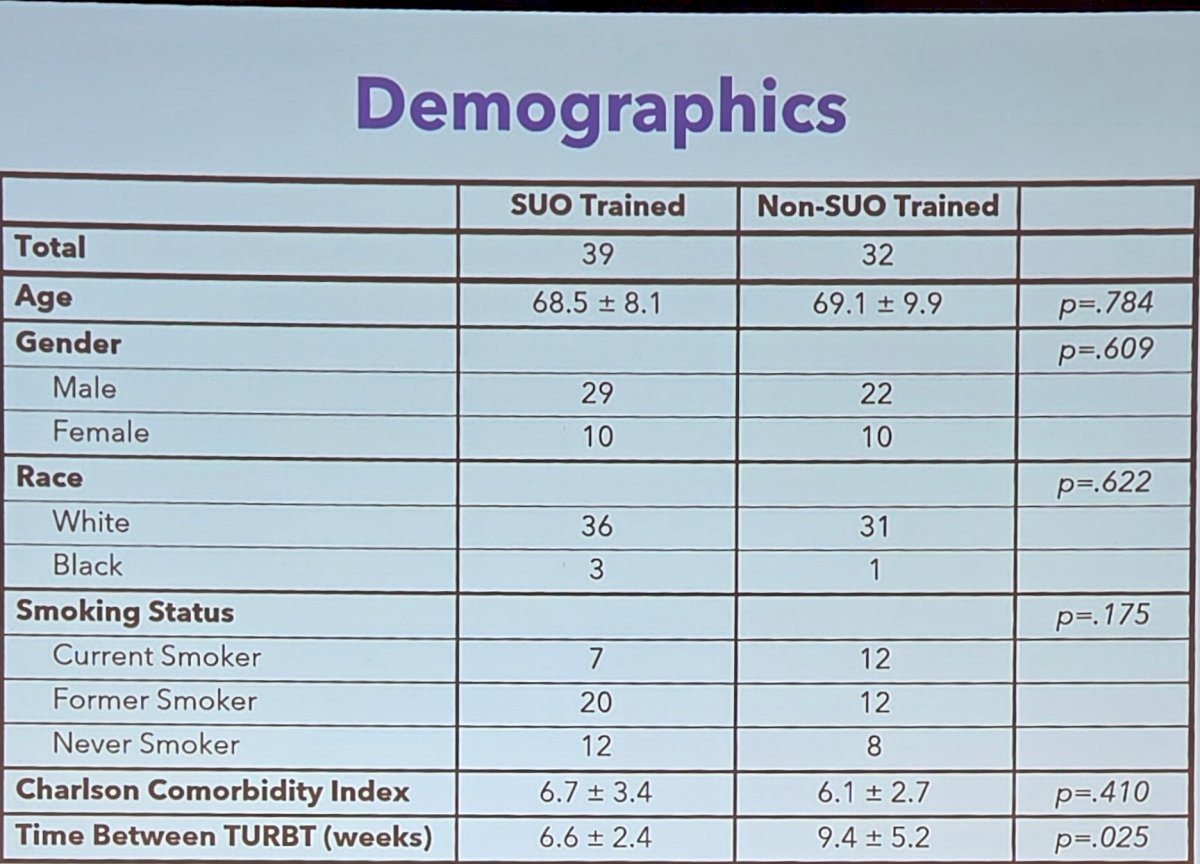
A total of 71 patients were identified, with 39 patients having an index TURBT with an SUO-trained urologist and 32 patients having an index TURBT with a non-SUO trained urologist:
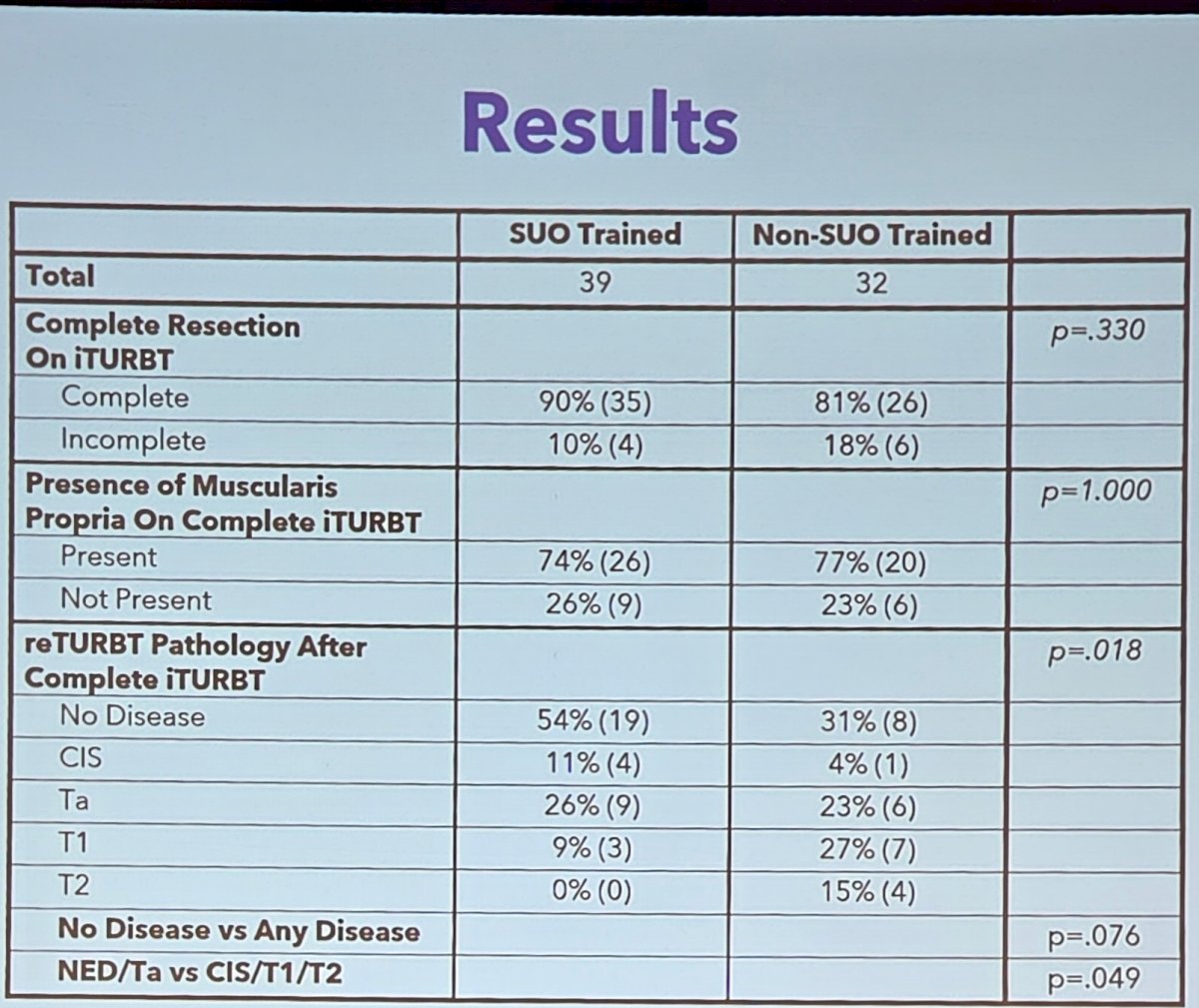
Complete resection rates (SUO 90% versus non-SUO 81%; p = 0.330) and muscularis propria sampling rates (SUO 74% versus non-SUO 77%; p = 1.00) on index TURBT were similar between both groups. On restaging TURBT, 54% of patients who underwent index TURBT with an SUO-trained urologist had no evidence of disease, and no patients had T2 disease on restaging TURBT among the SUO-trained cohort. Patients who had index TURBT with non-SUO trained urologists had a 31% incidence of no evidence of disease on restaging TURBT, and were upstaged to T2 disease in 15% of cases. As such, there was a significant difference in upstaging between the two groups (p = 0.018):
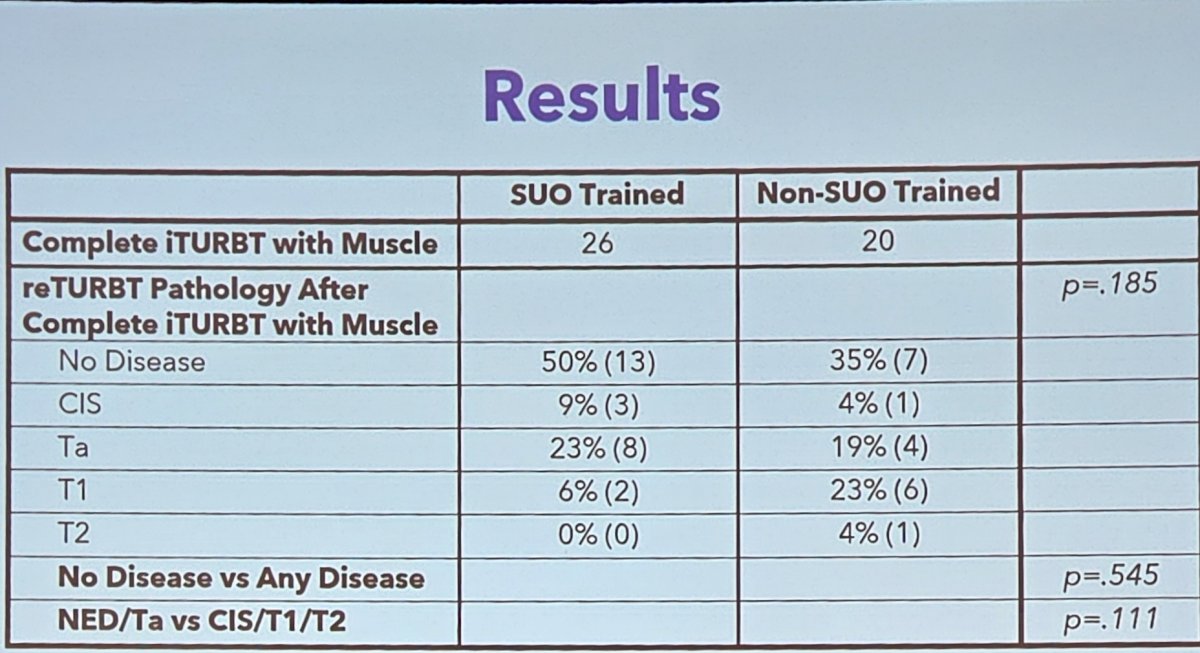
When only assessing patients who had a complete index TURBT with muscle in the sample were considered, the differences in restaging TURBT outcomes were no longer significant:
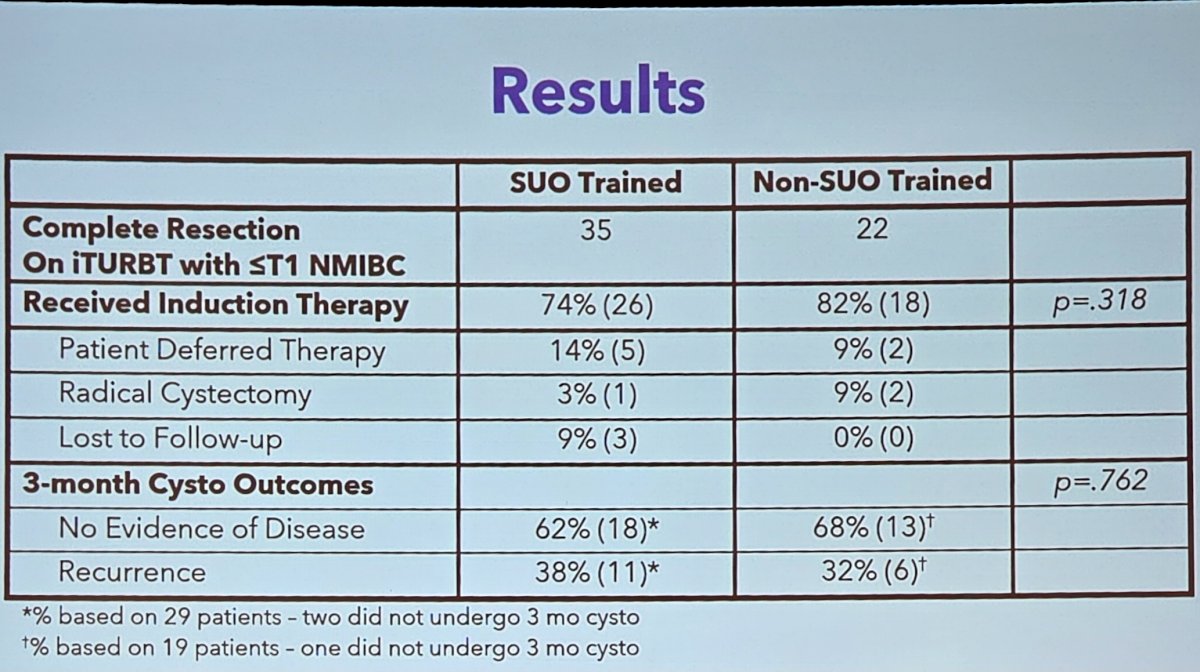
Regardless of fellowship training, recurrence free survival was similar at the time of the 3 month surveillance cystoscopy:
Dr. Kim concluded this presentation discussing differences in restaging TURBT pathology outcomes based on index TURBT performed by an SUO fellowship trained or non-SUO trained urologist, with the following take-home points:
- Lower rates of residual disease and pathologic upstaging at restaging TURBT are seen when index TURBT is performed by an SUO-trained urologist compared to a non-SUO trained urologist
- However, these differences diminish when evaluating patients who had adequate resection with muscle in the index TURBT sample
- Additionally, short term oncologic outcomes appear to be similar between groups if an adequate resection is initially performed
- This data is limited by its retrospective nature, and further investigation is also necessary to evaluate the prognostic significance of residual disease on restaging TURBT and oncologic outcomes stratified by surgeon experience
Presented by: Joon Kyung Kim, MD, University of Kentucky, Lexington, KY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Southeastern Section of the American Urological Association (SESAUA) Annual Meeting, San Juan, PR, Wed, Mar 18 – Sat, Mar 21, 2026.