(UroToday.com) The 2025 SESAUA annual meeting featured a prostate cancer session and a presentation by Dr. Paul Sieber discussing outcomes of men with high-risk biochemically recurrent prostate cancer who suspended enzalutamide monotherapy treatment in the phase 3 EMBARK study. Biochemical recurrence occurs in 20-50% of patients with prostate cancer within 10 years of definitive therapy, which increases the risk of prostate cancer specific mortality. On November 16, 2023, enzalutamide received an FDA label extension for the treatment of nonmetastatic castration-sensitive prostate cancer with high risk biochemical recurrence. This was based on data from the EMBARK trial that showed enzalutamide + leuprolide and enzalutamide monotherapy improved metastasis-free survival versus leuprolide alone in patients with high-risk biochemically recurrent prostate cancer.1 In EMBARK, treatment was suspended in 304 (85.9%) patients who received enzalutamide monotherapy and 240 (67.8%) patients who received leuprolide alone. Outcomes by treatment suspension status were presented at SESAUA 2025.
EMBARK (NCT02319837) is a double-blind, phase 3 study. Patients with high-risk biochemically recurrent (PSA doubling time ≤9 months and PSA ≥2 ng/mL above nadir post radiotherapy or ≥1 ng/mL after radical prostatectomy ± postoperative radiotherapy) were randomized (1:1) to enzalutamide monotherapy (160 mg/day, open label) or leuprolide alone:
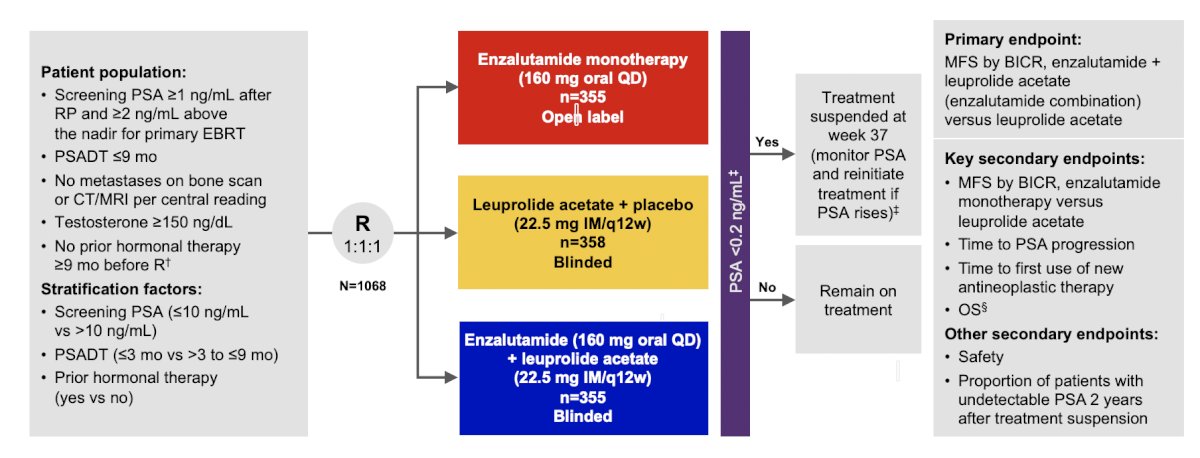
PSA <0.2 ng/mL at week 36 triggered treatment suspension at week 37 and treatment restarted at PSA ≥2 or ≥5 ng/mL for patients with or without primary radical prostatectomy, respectively. The proportion of patients with undetectable PSA 2 years after treatment suspension was a secondary endpoint, and metastasis-free survival (by blinded independent central review) was analyzed descriptively.
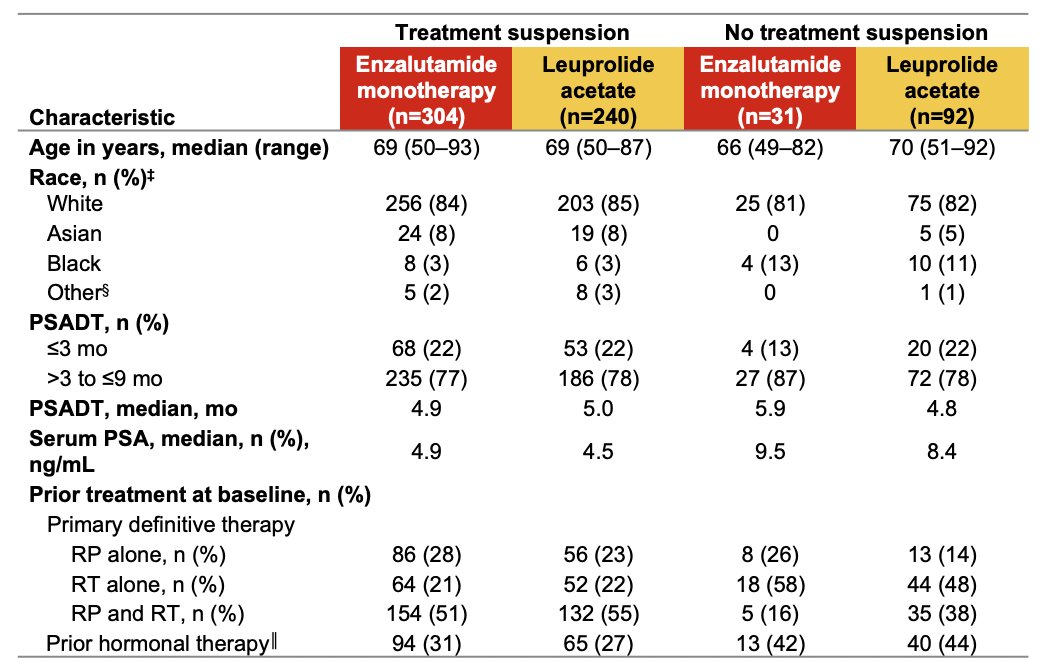
The baseline demographics for those who underwent treatment suspension versus those with no treatment suspension were well balanced and as follows:
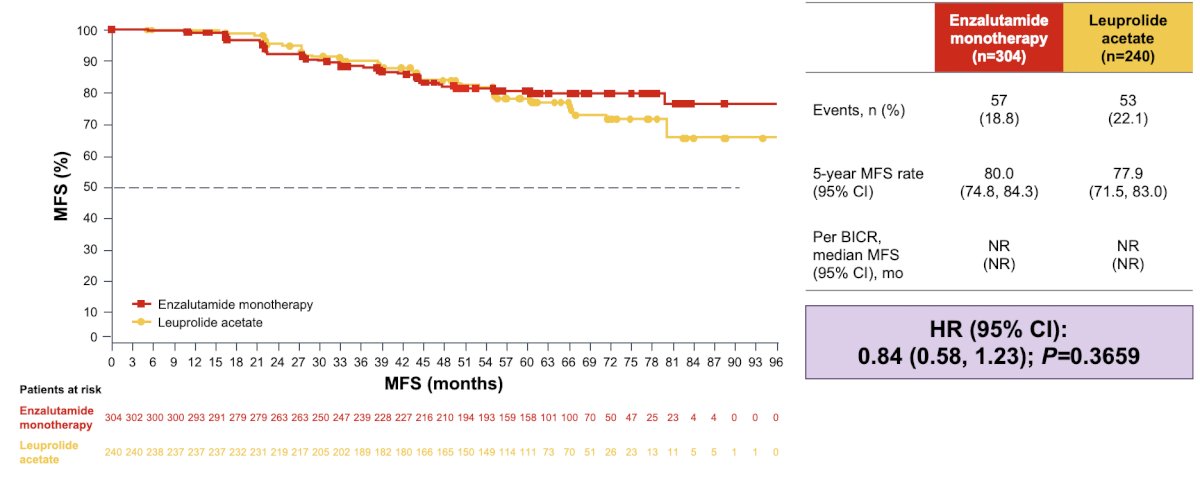
In the suspension group, 3-year metastasis-free survival rate was 88.1% (95% CI 83.8-91.4%) for enzalutamide monotherapy and 90.0% (95% CI 85.3-93.2%) for leuprolide alone. There was no meaningful difference in metastasis-free survival (HR 0.840, 95% CI 0.58-1.23):
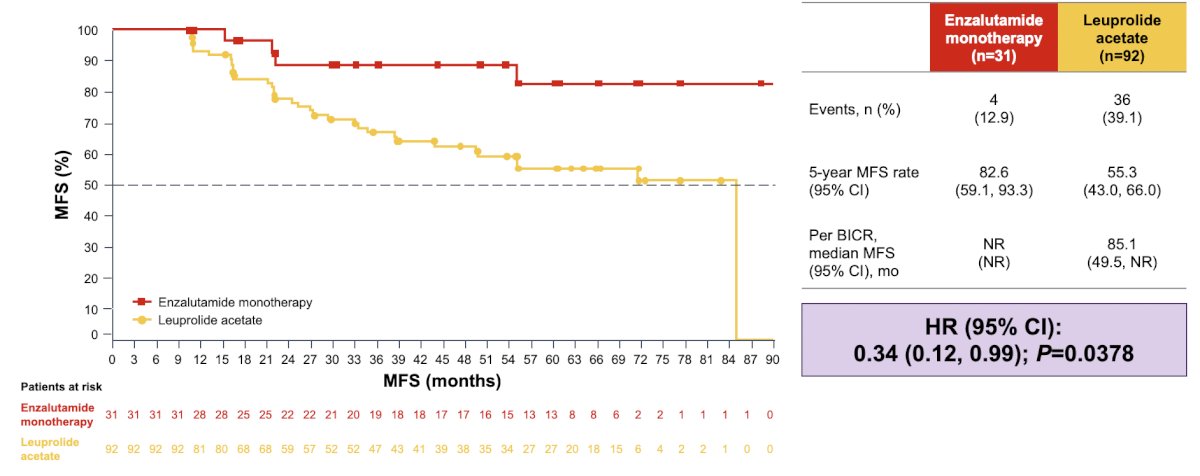
In the no suspension group, 3-year metastasis-free survival rates were 88.5% (95% CI 68.5-96.2%) and 66.9% (95% CI 55.4-76.1%), respectively; metastasis-free survival events were limited (n=4) for enzalutamide monotherapy (HR 0.34, 95% CI 0.12-0.99):
In the suspension versus the no suspension group, more patients received prior radical prostatectomy (enzalutamide monotherapy: 78.9% versus 41.9%; leuprolide alone: 78.3% versus 52.2%) or radical prostatectomy and radiotherapy (enzalutamide monotherapy: 50.7% versus 16.1%; leuprolide alone: 55.0% versus 38.0%), however, the baseline median PSA doubling time was similar (enzalutamide monotherapy: 4.9 months versus 5.9 months; leuprolide alone: 5.0 months versus 4.8 months). The proportion of patients with undetectable PSA 2 years after treatment suspension was 4.6% (95% CI 2.5-7.6%) for enzalutamide monotherapy and 9.6% (95% CI 6.2-14.0%) for leuprolide alone (p = 0.0326). The three most common treatment emergent adverse events for enzalutamide monotherapy cohort with and without treatment suspension were fatigue, gynecomastia, and arthralgia. The safety profile for enzalutamide monotherapy independent of treatment suspension status was comparable to that of the enzalutamide monotherapy arm of the overall study population:

Dr. Sieber concluded his presentation by discussing outcomes of men with high-risk biochemically recurrent prostate cancer who suspended enzalutamide monotherapy treatment in the phase 3 EMBARK study with the following take-home points:
- In patients with high-risk biochemical recurrence, more patients achieved treatment suspension with enzalutamide monotherapy (86%) compared with leuprolide alone (67%)
- In patients who suspended treatment, metastasis free survival was similar between enzalutamide monotherapy and leuprolide alone
- In patients who did not suspend treatment, enzalutamide monotherapy prolonged metastasis free survival versus
leuprolide alone- The number of metastasis free survival events was limited for enzalutamide monotherapy (n = 4 [13%]) compared with leuprolide alone (n = 36 [39.1%])
- Two years following treatment suspension, <10% of patients in both treatment groups had undetectable PSA levels
- No new safety signals were reported. Following treatment with enzalutamide monotherapy, adverse events for patients who suspended treatment and for those who did not suspend treatment were comparable to those reported for the overall study population for enzalutamide monotherapy
Presented by: Paul R. Sieber, MD, Keystone Urology Specialists, Lancaster, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (SESAUA) 2025 Annual Meeting, Nashville, TN, Wed, Mar 12 – Sat, Mar 15, 2025.
References: