(UroToday.com) The 2025 SESAUA annual meeting featured a prostate cancer session and a presentation by Dr. Paul Sieber discussing a post hoc analysis from the phase 3 EMBARK study assessing PSA dynamics. FDA approval of enzalutamide for treatment of non-metastatic CSPC with biochemical recurrence at high risk for metastasis, was based on data from the EMBARK trial.
This was a phase 3 trial that demonstrated that enzalutamide + leuprolide (enzalutamide combination) and enzalutamide monotherapy significantly improved metastasis-free survival versus placebo + leuprolide alone in high-risk biochemically recurrent prostate cancer patients.1 EMBARK included a treatment suspension at week 37 if PSA was <0.2 ng/mL and re-initiation at pre-defined PSA thresholds. This post hoc analysis of PSA dynamics in EMBARK aimed to understand the time course to undetectable PSA and likelihood of undetectable PSA after treatment re-initiation.
EMBARK enrolled high-risk biochemically recurrent patients, post definitive therapy. High-risk was defined as PSA doubling time ≤9 months and PSA ≥2 ng/mL above nadir post radiotherapy or ≥1 ng/mL post radical prostatectomy ± postoperative radiotherapy. Patients were randomized (1:1:1) to receive enzalutamide combination 160 mg/day (double blind), leuprolide alone (double blind), or enzalutamide monotherapy (open label). Leuprolide 22.5 mg was administered every 12 weeks: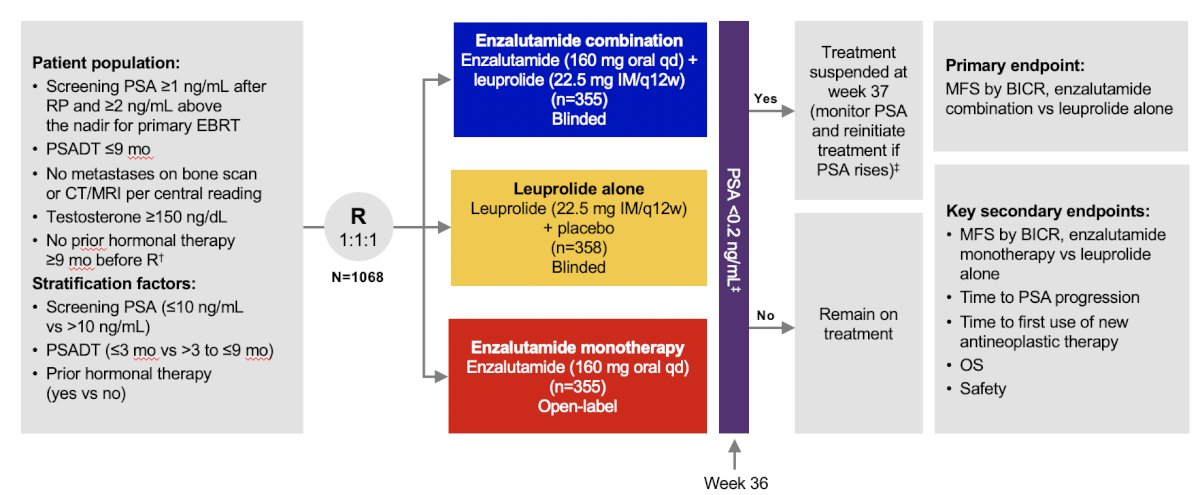
If serum PSA was <0.2 ng/mL at week 36, treatment was suspended at week 37 and restarted when PSA was ≥2 ng/mL for radical prostatectomy patients and ≥5 ng/mL for non-radical prostatectomy patients. A post hoc analysis of PSA dynamics was conducted in each treatment cohort.
The patient disposition based on treatment suspension status is highlighted in the following table: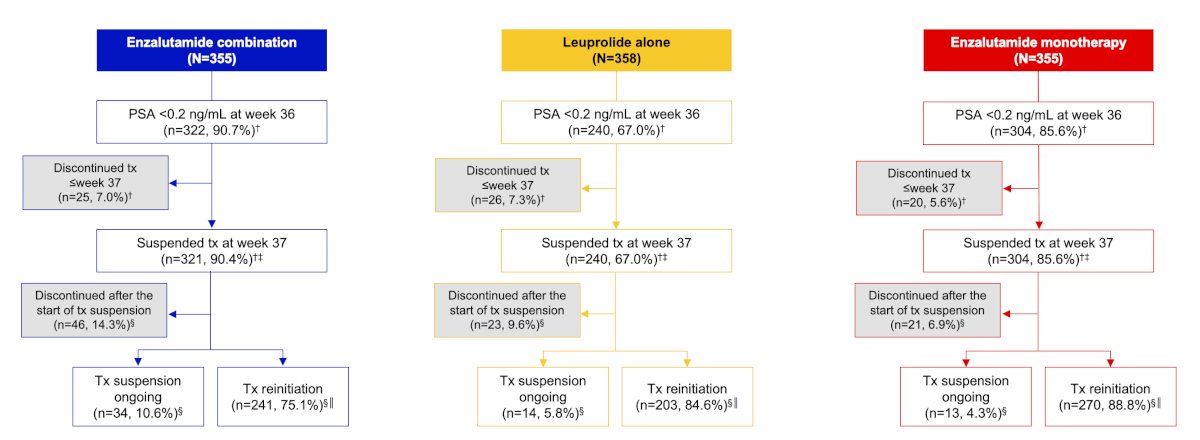
Of 1,068 eligible patients, most in all three treatment groups reached undetectable PSA (<0.2 ng/mL) by week 25, with percentages higher for enzalutamide combination and monotherapy versus leuprolide alone:
More patients had treatment suspended with enzalutamide combination and monotherapy versus leuprolide alone. Of patients who suspended treatment at week 37, 89% reinitiated treatment with enzalutamide monotherapy, 85% with leuprolide alone, and 75% with enzalutamide combination. Of patients who reinitiated treatment, 96% of men treated with enzalutamide combination and 90% treated with enzalutamide monotherapy reached undetectable PSA again versus 73% with leuprolide alone: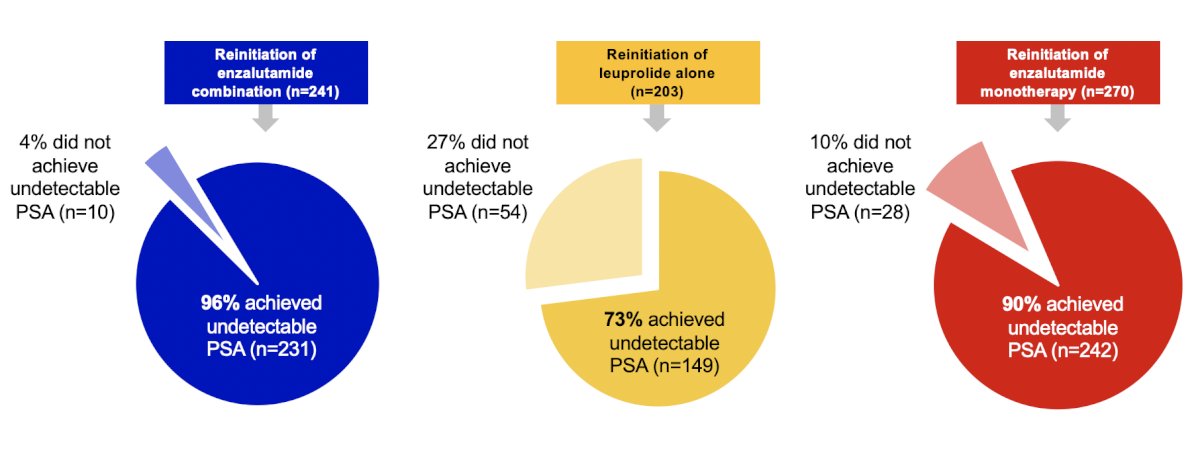
Metastasis free survival for patients who achieved or did not achieve undetectable PSA levels after treatment re-initiation is highlighted in the following figure:
Dr. Sieber concluded his presentation discussing a post hoc analysis from the phase 3 EMBARK study assessing PSA dynamics with the following take-home points:
- In patients with high-risk biochemical recurrence, more patients treated with enzalutamide (both as combination and monotherapy) versus leuprolide alone achieved:
- Undetectable PSA levels at week 36 and subsequent treatment suspension at week 37
- Undetectable PSA levels earlier (week ≤25)
- Undetectable PSA levels after treatment re-initiation
- Due to durable undetectable PSA levels (<0.2 ng/mL), more patients had treatment suspension ongoing in the enzalutamide combination group versus leuprolide alone after a median of 4 years 11 months
- Independent of treatment type, achievement of undetectable PSA levels after treatment re-initiation was associated with improved metastasis free survival
Presented by: Paul R. Sieber, MD, Keystone Urology Specialists, Lancaster, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Southeastern Section of the American Urological Association (SESAUA) 2025 Annual Meeting, Nashville, TN, Wed, Mar 12 – Sat, Mar 15, 2025.
References: