(UroToday.com) The 2025 SESAUA annual meeting featured a kidney cancer session and a presentation by Dr. Maxwell Sandberg discussing results from a study of the Intercontinental Collaboration on Renal Cell Carcinoma Database assessing systemic therapy for renal cell carcinoma with tumor thrombus.
Renal cell carcinoma with tumor thrombus has traditionally been treated with surgical resection alone, but with advances in systemic therapy, clinicians are often now employing a multimodal approach to treatment. Thus, the true benefit of systemic therapy is unknown for renal cell carcinoma with tumor thrombus. The primary objective of this study presented at SESAUA 2025 was to assess the utility of using systemic therapy for these patients, and the secondary objective was to assess the utility of systemic therapy in subgroups of patients.
This was a multi-institutional study conducted across North America, Central/South America, and South Korea. Patient information was retrospectively reviewed from 1999 to 2024, and every patient underwent radical nephrectomy with tumor thrombectomy +/- systemic therapy. Systemic therapy was defined as chemotherapy, immunotherapy, targeted therapy, or any combination of these options. Patients were excluded if they had systemic therapy > 12 months from radical nephrectomy with tumor thrombectomy.
There were 459 patients included in the primary analysis (178 systemic therapy at any point before or after surgery and 281 no systemic therapy). In analysis #1 assessing non-metastatic renal cell carcinoma neoadjuvant systemic therapy, metastasis free survival was worse in patients with systemic therapy (p < 0.0001), and systemic therapy regimen did not affect metastasis free survival (p > 0.05):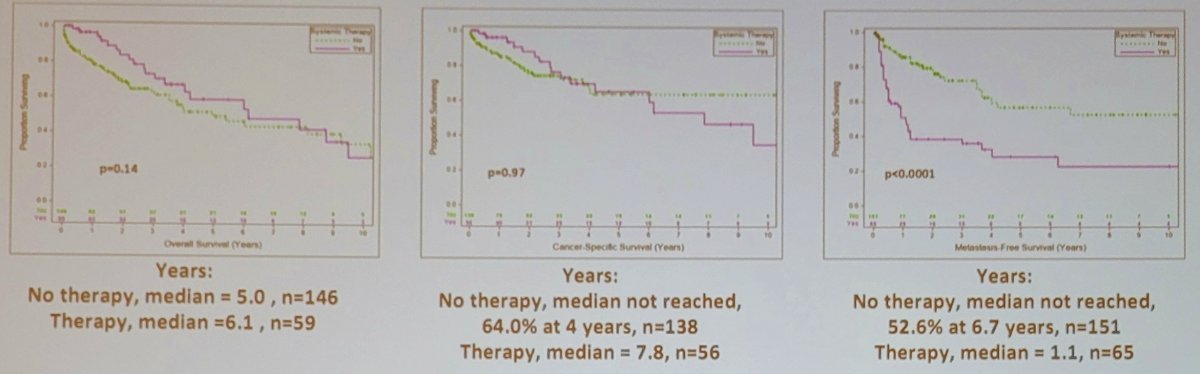
In analysis #2 assessing metastatic neoadjuvant systemic therapy, overall survival and cancer specific survival was superior in these patients receiving therapy who subsequently underwent cytoreductive nephrectomy: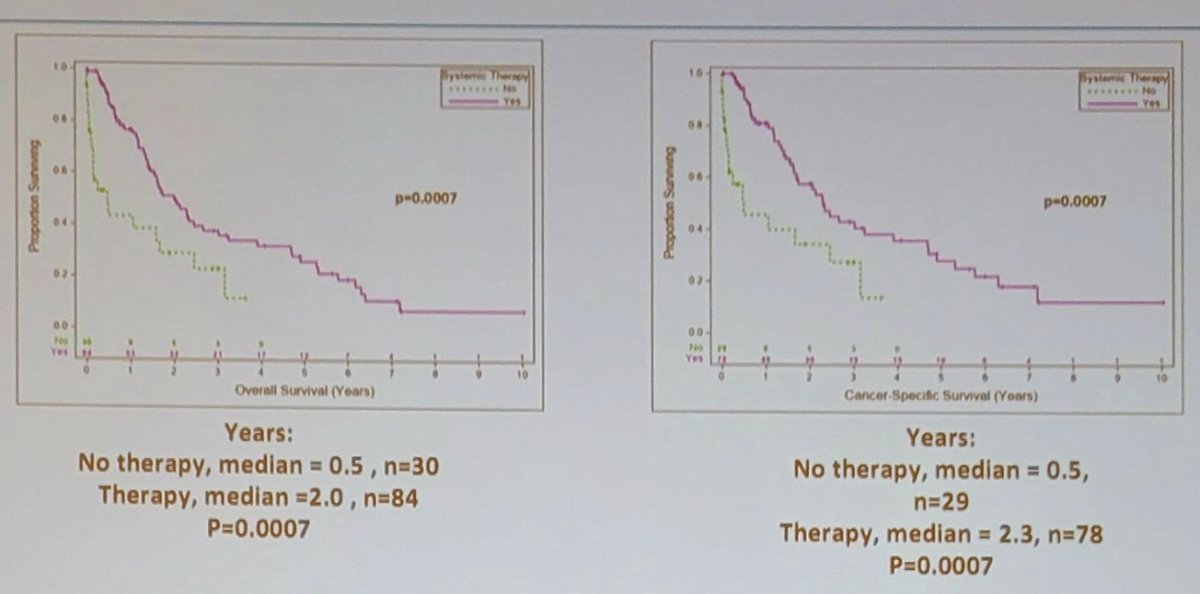
Additionally, in a sensitivity analysis, chemotherapy + immunotherapy had the greatest overall survival (p = 0.003) and cancer specific survival (p = 0.028). In analysis #3 assessing post-operative systemic therapy (excluding preoperative metastatic renal cell carcinoma tumor thrombus patients from the metastasis free survival analysis), there were no significant differences between groups, and no difference by systemic therapy regimen:
Dr. Sandberg noted several limitations of this study, including the retrospective nature, no standard regimens (and no standard doses or cycles), and additional analyses are needed by subtype. Moreover, there was an attempt to avoid systemic therapy for progression after radical nephrectomy with tumor thrombectomy in the third analysis, with a median time of 2.7 months after surgery.
Dr. Sandberg concluded his presentation discussing results from a study of the Intercontinental Collaboration on Renal Cell Carcinoma Database assessing systemic therapy for renal cell carcinoma with tumor thrombus with the following take-home points:
- In analysis #1, non-metastatic renal cell carcinoma tumor thrombus patients who received systemic therapy had worse metastasis free survival, although it is unlikely that systemic therapy is predisposing patients to metastasis, thus, the cause is difficult to ascertain
- In analysis #2, metastatic renal cell carcinoma tumor thrombus patients who receive neoadjuvant systemic therapy before cytoreductive nephrectomy have improved overall and cancer specific survival. In this cohort, chemotherapy + immunotherapy was the superior regimen
- In analysis #3, overall survival, cancer specific survival, and metastasis free survival were equivalent in patients who received postoperative systemic therapy, and there does not appear to be a role for systemic therapy after radical nephrectomy with tumor thrombectomy
Presented by: Maxwell Sandberg, MD, Atrium Health Wake Forest Baptist Medical Center, Winston Salem, NC
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Southeastern Section of the American Urological Association (SESAUA) 2025 Annual Meeting, Nashville, TN, Wed, Mar 12 – Sat, Mar 15, 2025.