(UroToday.com) The 2025 SESAUA annual meeting featured a bladder cancer session and a presentation by Dr. Joon Kyung Kim discussing an evaluation of systemic therapy and surgical consolidation in patients with node positive upper tract urothelial carcinoma. The recommended treatment for high-grade upper tract urothelial carcinoma includes radical nephroureterectomy with regional lymph node dissection for clinically organ-confined disease. The timing of peri-operative systemic therapy is multifactorial, with extrapolation of data from muscle-invasive bladder cancer in the neoadjuvant setting, and level 1 data for upper tract urothelial carcinoma in the adjuvant setting based on the POUT trial.1 The timing of peri-operative systemic therapy and need for surgical consolidation in the clinically node positive setting is even more unclear. The goal of this study presented at SESAUA 2025 was to compare survival in clinically node positive patients managed with neoadjuvant, adjuvant, and systemic therapy alone approaches.
Patients with cT0-4 N1-3 M0 upper tract urothelial carcinoma who received chemotherapy with or without nephroureterectomy between 2018 and 2021 in the National Cancer Database (NCDB) were included. Patients were stratified into three treatment groups: chemotherapy only, neoadjuvant chemotherapy followed by nephroureterectomy, and nephroureterectomy followed by adjuvant chemotherapy. Overall survival was analyzed using Kaplan-Meier analysis and log rank tests, and Cox proportional hazard models were used to adjust for potential confounders.
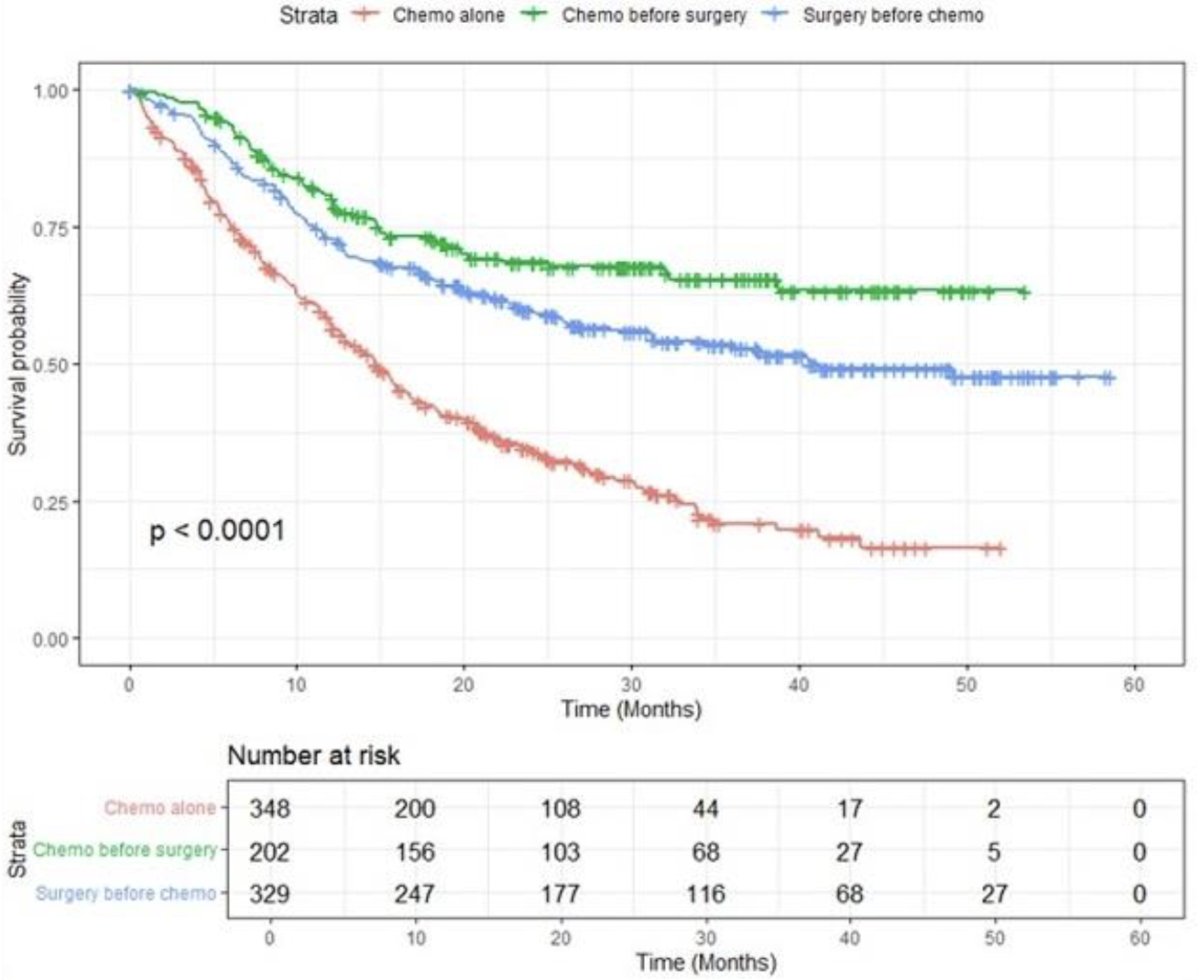
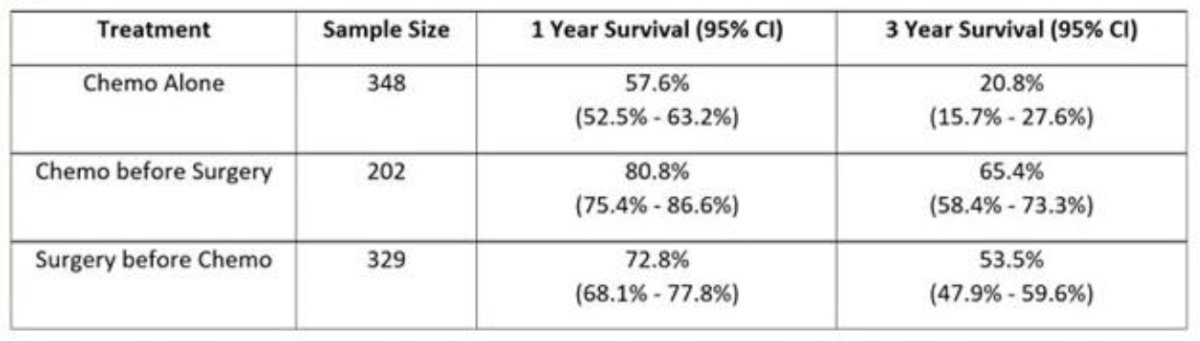
A total of 1,193 patients were included. Chemotherapy only, neoadjuvant chemotherapy followed by nephroureterectomy, and nephroureterectomy followed by adjuvant chemotherapy treatment groups consisted of 495, 287, and 411 patients, respectively. Patients in the chemotherapy-only group were older (p < 0.001), more commonly males (p < 0.001) compared with neoadjuvant chemotherapy followed by nephroureterectomy and nephroureterectomy followed by adjuvant chemotherapy cohorts. There was no significant difference in Charlson comorbidity index between the three groups. The pathologic complete response rate (ypT0N0) in the neoadjuvant chemotherapy followed by nephroureterectomy was 6.5%. Patients managed with neoadjuvant chemotherapy followed by nephroureterectomy exhibited the most favorable overall survival compared to nephroureterectomy followed by adjuvant chemotherapy and chemotherapy only (p < 0.0001), with 3-year overall survival 65.4% (95% CI 58.4%-73.3%), 53.5% (47.9%-59.6%), and 20.8% (15.7%-27.6%) in these groups, respectively:
On multivariate analysis controlling for age, sex, and clinical stage using neoadjuvant chemotherapy followed by nephroureterectomy as a referent, nephroureterectomy followed by adjuvant chemotherapy and chemotherapy only exhibited inferior overall survival (HR 1.48, 95% CI 1.06-2.06, p = 0.021 and HR 2.92, 2.14-4.00, p < 0.001, respectively):
Dr. Kim concluded his presentation by discussing an evaluation of systemic therapy and surgical consolidation in patients with node positive upper tract urothelial carcinoma with the following take-home points:
- The use of neoadjuvant chemotherapy followed by nephroureterectomy provides optimal survival outcomes in patients with clinically node positive high-grade upper tract urothelial carcinoma
- These data suggest that, when feasible, surgical consolidation is an important treatment component in patients with clinically node positive disease, likely owing to low rates of pathologic complete response
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (SESAUA) 2025 Annual Meeting, Nashville, TN, Wed, Mar 12 – Sat, Mar 15, 2025.
Related content: Comparing Therapy Approaches for Advanced Upper Tract Urothelial Carcinoma - Joon Kyung Kim
References:
- Birtle A, Johnson M, Chester J, et al. Adjuvant chemotherapy in upper tract urothelial carcinoma (the POUT trial): A phase 3, open-label, randomized controlled trial. Lancet 2020 Apr 18;395(10232):1268-1277.