(UroToday.com) The 2025 SESAUA annual meeting featured a bladder cancer session and a presentation by Dr. Peter Clark discussing a first-in-human study of TAR-210 erdafitinib intravesical system in patients with non-muscle invasive bladder cancer with select FGFR alterations.
To date, treatment options are limited for recurrent non–muscle-invasive bladder cancer. Activating fibroblast growth factor receptor genetic (FGFR) alterations are frequent in non-muscle invasive bladder cancer. Oral erdafitinib, a selective pan-FGFR tyrosine kinase inhibitor, demonstrated robust clinical efficacy in non-muscle invasive bladder cancer but had frequent systemic side effects. TAR-210 is a novel erdafitinib intravesical system designed to provide local, sustained release of erdafitinib within the bladder over 12-week cycles while limiting systemic toxicities. This open-label, multicenter phase 1 study (NCT05316155) evaluates the safety, pharmacokinetics, and efficacy of TAR-210 in patients with non-muscle invasive bladder cancer whose tumors harbor select FGFR alterations.
Study-qualifying FGFR alterations were identified in tumor tissue and/or urine cell-free DNA. Cohort 1 patients had recurrent, BCG-experienced, high-risk, non-muscle invasive bladder cancer (high-grade Ta/T1; papillary only) and refused or were ineligible for radical cystectomy. Cohort 3 patients had recurrent, intermediate-risk, non-muscle invasive bladder cancer (Ta/T1) with a history of only low-grade papillary disease. Before treatment, cohort 1 required resection of all visible non-muscle invasive bladder cancer, whereas cohort 3 required the presence of a visible tumor. Two TAR-210 dose levels were evaluated. Response is assessed every 3 months with continued treatment for up to 1 year if recurrence free (cohort 1) or in complete response (cohort 3):
Data from 21 patients in Cohort 1 and 43 patients in Cohort 3 who have been treated with TAR-210 were presented. The baseline characteristics are shown in the table below:
In cohort 1, 90% of patients were recurrence free at 12 months, the median recurrence free survival was not estimable, and the median duration of follow-up was 8.9 months: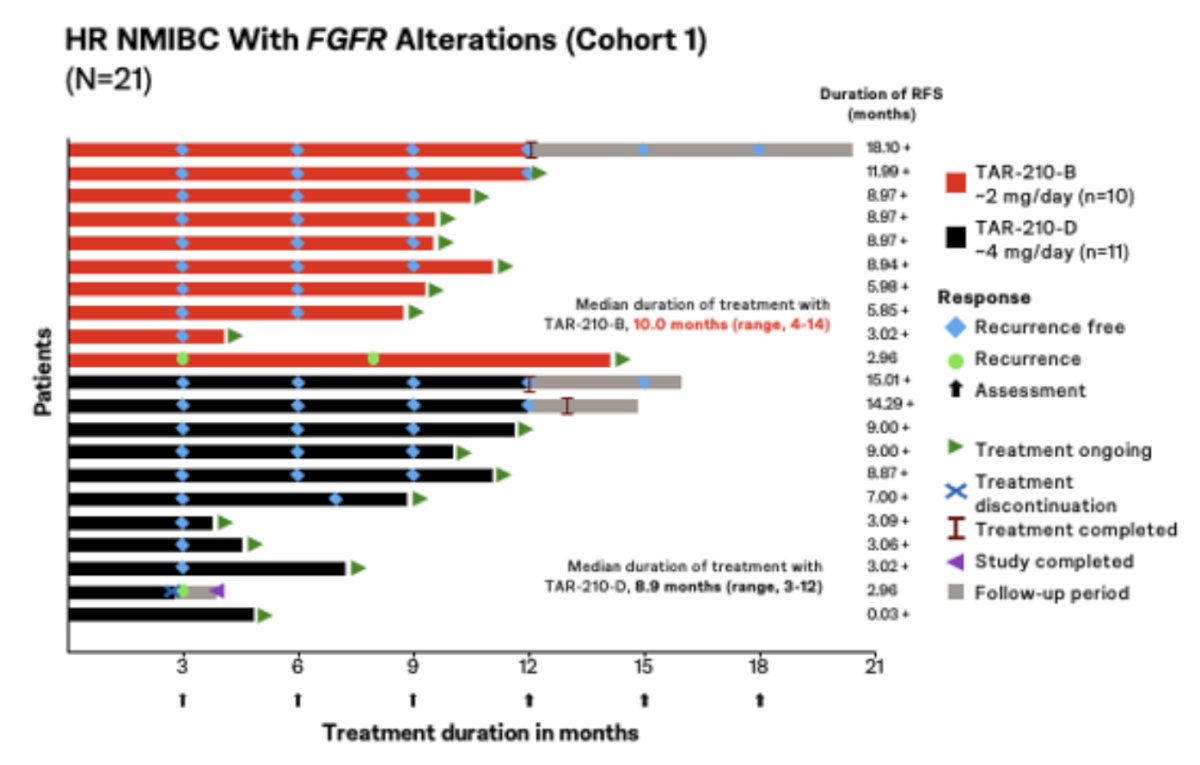
In cohort 3 only 31 patients were evaluable for response; 90% achieved a complete response rate, with 28/31 achieving a complete response at week 12. At the time of data analysis, 86% (24/28) of complete responses were ongoing:
TAR-210 provided sustained erdafitinib release in urine over 90 days with very low plasma concentrations: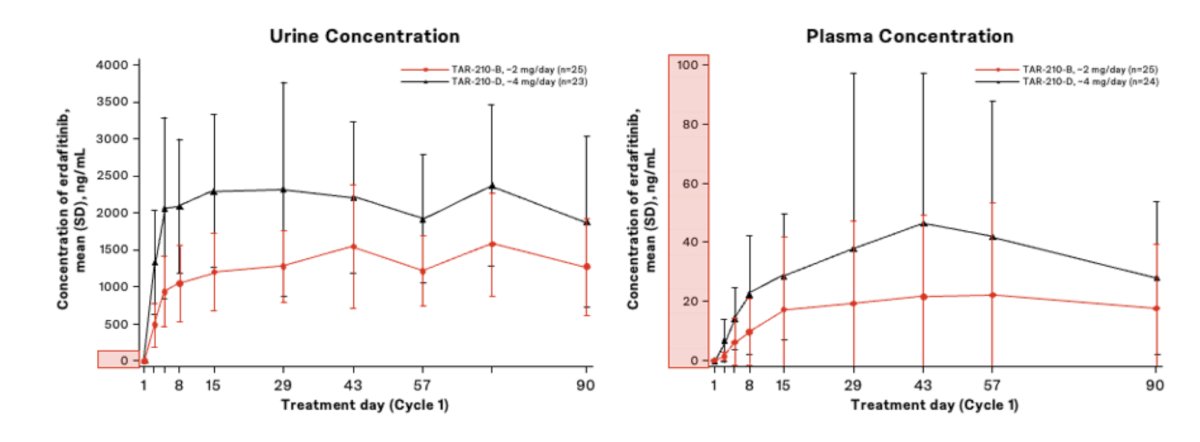
The most common treatment-related adverse events were grade 1/2 lower urinary tract adverse events. There were no dose-limiting toxicities. Two patients discontinued treatment due to adverse events of low-grade urinary symptoms, and one patient had serious adverse events of pyelonephritis and sepsis (unrelated to TAR-210). No deaths were reported, and from a safety standpoint, there were no dose-limiting toxicities:
Dr. Clark concluded his presentation discussing a first-in-human study of TAR-210 erdafitinib intravesical system in patients with non-muscle invasive bladder cancer with select FGFR alterations with the following take-home points:
- TAR-210 shows promising clinical activity in patients with FGFR-altered high risk intermediate risk non muscle invasive bladder cancer
- In BCG-experienced high risk non muscle invasive bladder cancer (Cohort 1), the estimated 12-month recurrence free survival risk was 90% (95% Ci 66-97)
- In intermediate risk non muscle invasive bladder cancer (Cohort 3), 90% (95% CI 74-98) of patients achieved a complete response at week 12, with 86% of complete response ongoing at the time of clinical cutoff
- TAR-210 provided high erdafitinib concentrations in the urine with very low plasma concentrations, limiting systemic toxicities
- The majority of treatment related adverse events were grade 1 or 2 lower urinary tract adverse events, and rates of treatment discontinuation due to treatment related adverse events were low (3%)
- Based on these first in human results, the phase 3 MoonRISe-1 study in FGFR-altered intermediate risk non muscle invasive bladder cancer has been initiated
Presented by: Peter Clark, MD, Atrium Health Levine Cancer Institute, Charlotte, NC
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Southeastern Section of the American Urological Association (SESAUA) 2025 Annual Meeting, Nashville, TN, Wed, Mar 12 – Sat, Mar 15, 2025.